
Abstract
Abstract
Introduction:
This report evaluates the results of a two-surgeon experience with thoracoscopic repair in patients with long gap esophageal atresia (EA).
Materials and Methods:
From March 2000 to February 2015, 14 consecutive patients with pure EA were repaired thoracoscopically. The gap length was then evaluated by contrast gastrostomy tube study. Patients were operated on between 4 to 8 weeks of age. Patient weights ranged from 2.6 to 3.8 kg. The longest gap was 7½ vertebral bodies. Dissection was carried well up into the thoracic inlet on the upper pouch and down to the esophageal hiatus on the lower pouch. A 15th patient was not referred until 3 months of age.
Results:
All 15 procedures were completed successfully thoracoscopically. Operative times ranged from 60 to 135 minutes. There were two leaks; both resolved with conservative therapy. Feeds were started on Day 5 in all other patients. Six of 13 patients required dilations (one to nine), and 8 required a Nissen fundoplication for severe reflux. All patients are currently on full oral feeds. No patient has any evidence of chest wall asymmetry, winged scapula, or clinically significant scoliosis.
Conclusions:
Thoracoscopic repair of long gap EA has proven to be an effective and safe technique when performed in the first 2 months of life. The improved visualization and access to the upper pouch and lower pouches allow for maximal mobilization. The results are superior to those of documented open series and avoid the morbidity of repeated operations in the neonatal period.
Introduction
N
Ever since the first successful thoracoscopic repair of a pure EA in 1999 1 and the first thoracoscopic tracheoesophageal fistula (TEF) in 2000, 2 one of us (S.S.R.) has used a thoracoscopic approach for all patients with pure EA and EA/TEF, whereas the other (A.W.F.) adopted the approach in 2008. This article describes a two-surgeon experience with long gap EA using only the thoracoscopic approach.
Materials and Methods
From March 2000 to February 2015 (S.S.R.) and from September 2008 to February 2015 (A.W.F.), 14 consecutive patients at two institutions with pure EA were repaired by or under the direct supervision of the authors. No patient was excluded based on gap length.
All patients initially underwent placement of a gastrostomy tube (G-tube). All patients were then kept in the hospital in the Level 2 nursery to allow for growth and upper pouch suctioning. The gap length was evaluated approximately every 2 weeks by contrast G-tube study with downward pressure placed on the nasogastric tube (Fig. 1) or by placement of bougies in the upper and lower pouches under fluoroscopy (Fig. 2).
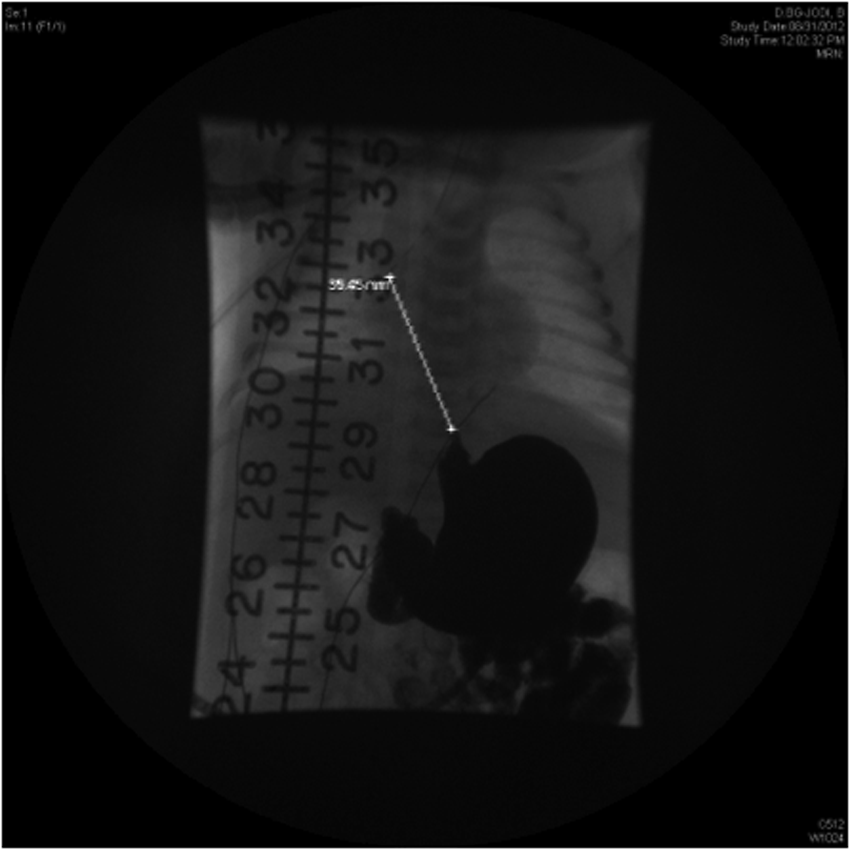
Upper gastrointestinal series through the gastrostomy tube showing a gap of over six vertebral bodies after 2 months.
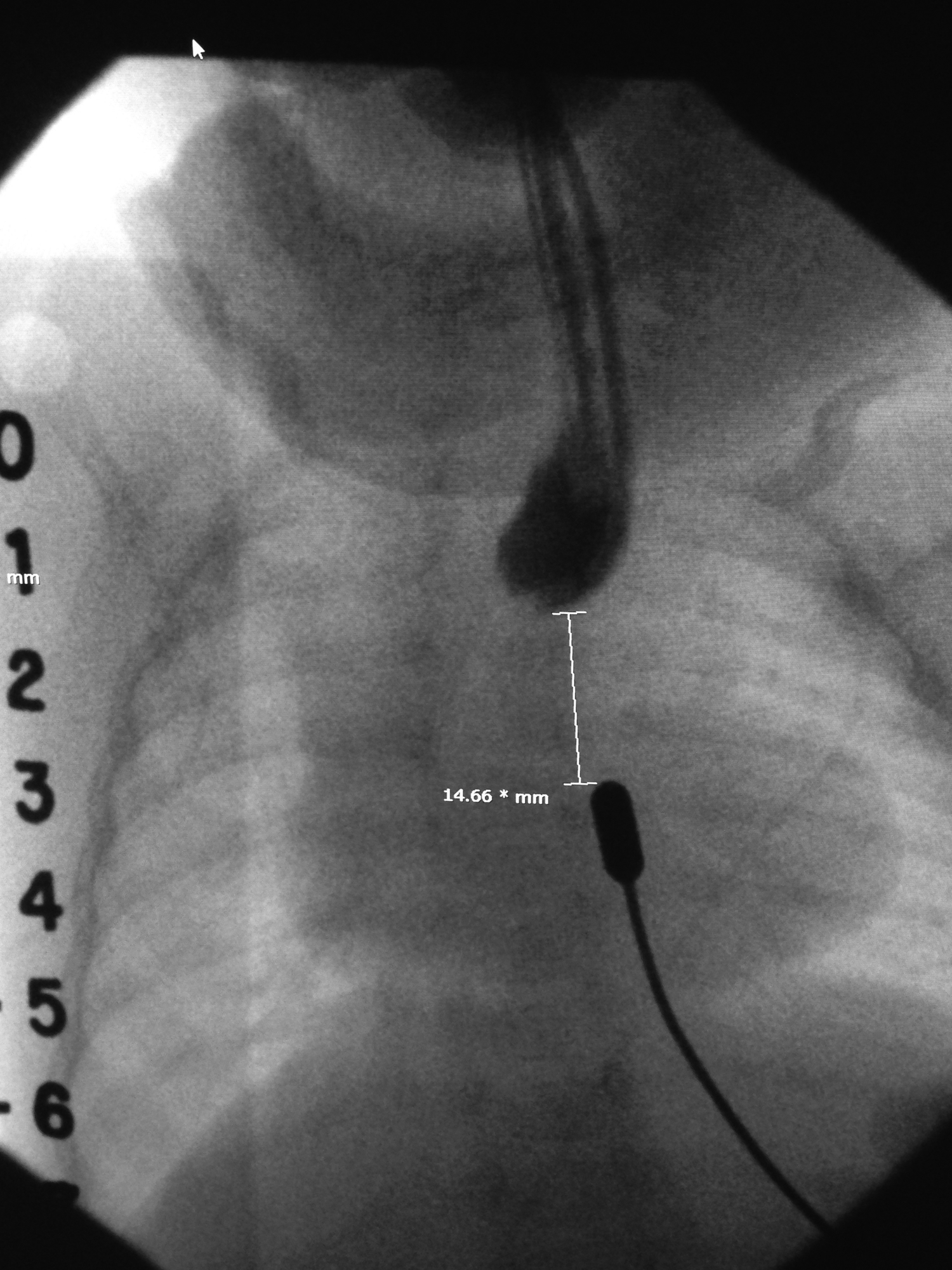
Gap study using metal bougies to apply maximal pressure to determine gap length.
The patients were operated on between 4 to 8 weeks of age at the discretion of the surgeon, but factors considered included patient size, overall condition, and a failure to show any improvement in gap length. Patients with gaps over six vertebral bodies were allowed to grow for 2 months prior to operation. Patient weights ranged from 2.6 to 3.8 kg. Six patients had significant associated congenital anomalies, 5 with congenital heart disease and 2 with imperforate anus, which were treated initially by colostomy. The longest gap was 7½ vertebral bodies.
The repairs were performed using a three-port technique as previously described.3,4 Dissection was carried well up into the thoracic inlet and into the neck on the upper pouch (Fig. 3). The lower pouch was mobilized as much as necessary to achieve the anastomosis. In most cases this was down to the esophageal hiatus; however, the hiatus was not breached in any case. The anastomosis was performed with monofilament absorbable suture placed in a single interrupted fashion (Fig. 4). A transanastomotic tube was left by S.S.R., and chest drains were left in all cases.

Upper pouch dissection well into the thoracic inlet to obtain added length.
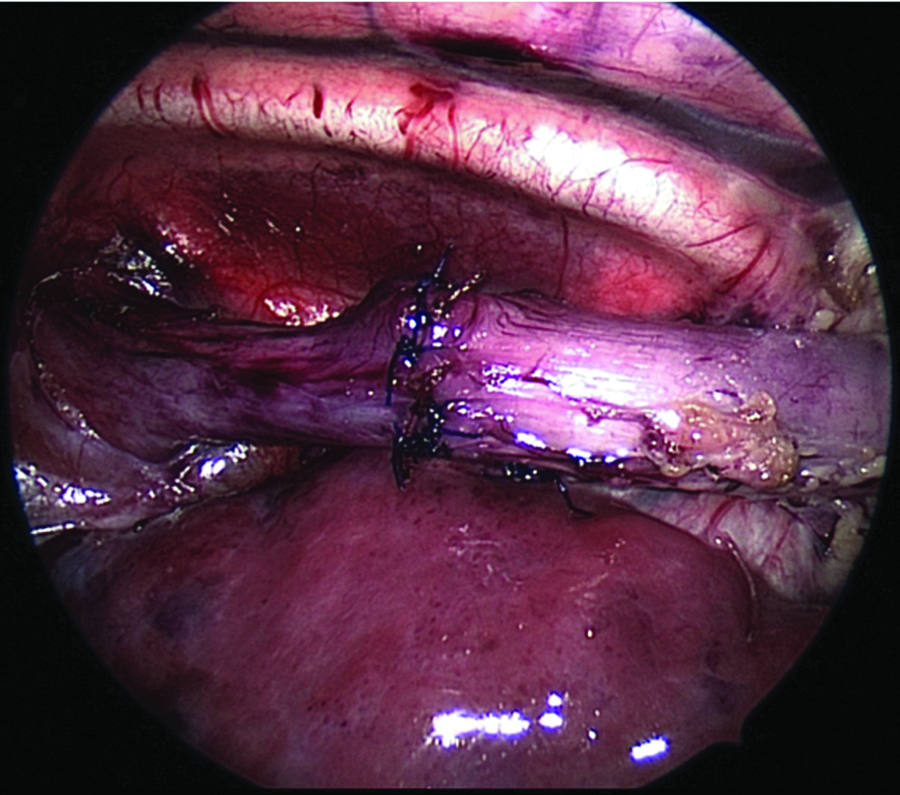
Anastomosis after maximal mobilization of the upper and lower pouches.
A 15th patient was not referred until 3 months of age. The patient's weight was 4.2 kg. This patient had a gap of five vertebral bodies under tension and ended up having an upper pouch fistula. This patient was approached through the left chest.
Results
All 15 procedures were completed successfully thoracoscopically. Operative times ranged from 60 to 135 minutes. There were two leaks; both resolved with conservative therapy. Feeds were started on Day 5 in all other patients. Six of 13 patients required dilations (one to nine), and 8 required a Nissen fundoplication for severe reflux. Two patients required a second Nissen for a hiatal hernia. All patients are currently on full oral feeds except for the patient just done 2 weeks ago. He remains on full G-tube feeds but is working on oral feeds. No patient has any evidence of chest wall asymmetry, winged scapula, or clinically significant scoliosis.
Discussion
The management of patients with long gap EA remains a significant challenge. Most pediatric surgeons agree that all attempts should be made to preserve the esophagus initially and that a repair should be tried after a period of growth. Spitz 5 has suggested that in some cases of extreme long gap that a primary anastomosis is not the best treatment and that a gastric pull-up may be the better option, performed at 2–3 months of age. However, initial management at most institutions is placement of a gastrostomy button, upper pouch suctioning, and growth, with intermittent gap studies.
Many different techniques have been advocated to induce esophageal growth. These have included upper and lower pouch stretching with bougies. The procedure of Kimura and Soper 6 attempts upper pouch elongation by serial stretching on the anterior chest wall. Other surgical approaches have included the use of circular myotomies or flaps.7,8 More recently a great deal of attention has been given to dynamic stretching with traction sutures (the Foker procedure), which attempts early primary anastomosis. 9 This has been done both by open thoracotomy or thoracoscopically. 10 Unfortunately, all of the procedures have variable success and can be associated with significant short- and long-term morbidity.
Since the first thoracoscopic repair of a pure EA in 1999 and TEF in 2000, we have used this approach as our primary technique for patients. This approach, which has been modified slightly over the last decade, provides incredible visualization and exposure, especially in patients with pure EA who tend to be operated on when they are slightly larger (average, 3.4 kg). This exposure allows for exceptional visualization and dissection up into the neck. This approach easily allows the surgeon to dissect up to the level of the thyroid. We believe this technique allows greater mobilization than through an open thoracotomy and that extra length is achieved this way. In the case of the patient of the upper pouch fistula, the fistula was easily mobilized and divided thoracoscopically. It is important to remember that patients with presumed pure EA can have a high incidence of a proximal TEF, and we feel all should be evaluated with bronchoscopy. 11 This is not surprising, as we had previously reported our ability to approach H-type fistulas this way. 12
The second part is the ability to mobilize the distal pouch all the way down to the hiatus under direct vision and mobilization. Some have expressed concerns about devascularizing the lower pouch with extensive mobilization, but others have documented this can be done safely, and we have not found this to be an issue. 13 The 1–2 months of bolus G-tube feeds tends to dilate and thicken the lower pouch, giving the tissue more integrity under tension, when the anastomosis is finally attempted. The last part is the ability to perform the anastomosis in situ with the chest closed. We believe this diminishes the gap length and tension on the anastomosis. It is likely this is only a slight benefit, but in these long gaps millimeters may be the difference between success and failure.
The major difficulty of this technique is that in general all of the tension is placed on one suture at a time as opposed to laying in multiple sutures and spreading the tension over a series of sutures. In general, this is not a problem, and if we start to see tearing of the esophageal wall, we tie an air knot and place a second suture to spread the tension. Others have advocated placing corner-stay sutures that are brought out through the chest wall to help approximate the ends and spread the tension. Either way, there are techniques that can be used to avoid the problem of all the tension on one stitch.
To date we have not had to re-operate on any of the anastomoses for leak or stricture. The stricture rate requiring dilation is about 40%, and this is not surprising, but all patients thus far have responded favorably to dilation. Reflux is a significant problem, and this is also not surprising. Over 50% have required a fundoplication, and the redo rate stands at over 20% and is likely to go higher.
The combination of a short esophagus and hiatal hernia is the primary cause, and these patients may be candidates for early Collis–Nissen. But, these patients have tolerated their laparoscopic Nissens well, and the redos have been performed with out complication.
We have also used this technique in patients with Type III TEF and gaps of over four vertebral bodies. We did not include these patients in this analysis as we feel all patients with a distal fistula should be able to have a primary thoracoscopic repair.
There is no question that we have simply been lucky that we have not encountered a patient in whom we could not achieve a primary anastomosis. Our longest gap is 7½ vertebral bodies, and it is likely that a longer gap would be impossible to bridge. In these cases we would agree with Spitz 5 and do a gastric pull-up, but not until we proved that an anastomosis could not be achieved thoracoscocopically.
We believe that a period of growth of 1–2 months with G-tube feeds, followed by a thoracoscopic approach for anastomosis, provides the optimal approach in patients with a long gap EA and avoids much of the morbidity of early intervention, including multiple operations and prolonged intensive care unit stays.
Footnotes
Disclosure Statement
No competing financial interests exist.