
Abstract
Abstract
Introduction:
Both patent ductus arteriosus (PDA) and vascular rings often require surgical treatment to prevent complications and alleviate symptoms, respectively. Management in infants and children has traditionally required an open thoracotomy. However, given the known advantages of the thoracoscopic approach, increased technical experience, and improved instrumentation, the minimally invasive technique to repair these thoracic vascular anomalies has grown in popularity.
Subjects and Methods:
We report our experience with thoracoscopic PDA ligation and vascular ring division at a single institution. From October 1993 to March 2014, 78 patients underwent thoracoscopic PDA ligation, and 13 patients presented with vascular rings. Ages ranged from 2 days to 17 years (mean, 18 months), and weights ranged from 2 to 60 kg (mean, 8.5 kg) for the thoracoscopic PDA group, whereas ages ranged from 6 weeks to 13 years (mean, 19 months), and weights ranged from 3.6 to 38 kg (mean, 10 kg) for the thoracoscopic vascular ring division group. In the thoracoscopic PDA group, the mean operative time was 36 minutes. Complications consisted of one death not related to the procedure, one conversion to open for a torn ductus, one recurrence requiring re-operative thoracoscopic repair, and one residual PDA requiring cardiac catheterization with occlusion. In the vascular ring group, one procedure was unable to be completed thoracoscopically and was converted to open. In 2 cases, thoracoscopic exploration revealed no significant compression from the vascular ring, and dissection was stopped.
Conclusions:
Thoracoscopic closure of PDA and division of vascular rings are safe and effective techniques that minimize physiologic and cosmetic adverse effects.
Introduction
B
Subjects and Methods
From October 1993 to March 2014, 78 patient who underwent thoracoscopic PDA ligation and 13 patients who underwent thoracoscopic vascular ring division were retrospectively reviewed. Preoperative workup consisted of an echocardiogram for all patients and a computed tomography angiogram or magnetic resonance angiogram for the patients with vascular rings.
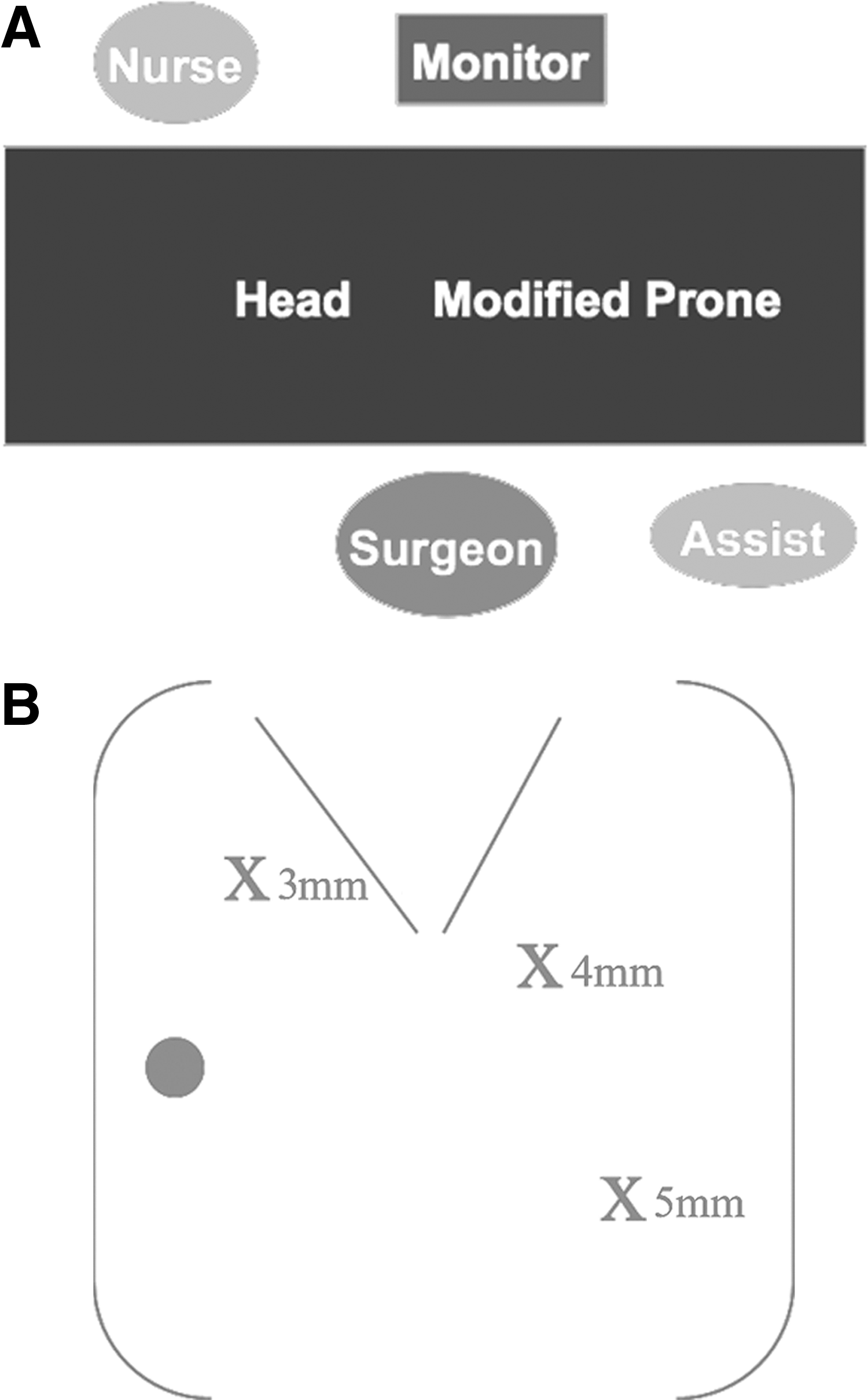
For thoracoscopic PDA ligation, patients were placed in a modified right lateral decubitus position with the left side elevated approximately 30°. Three ports were used, with a 4-mm port placed just posterior to the tip of the scapula for the camera. A 3-mm port was placed anteriorly approximately 1–2 interspaces above, and a 3-mm port, which was changed to a 5-mm port for clip application, was placed posteriorly 1–2 interspaces below, the camera port (Fig. 1). All patients were monitored with pre- and postductal pulse oximetry. The lung was retracted medially, and the parietal pleura overlying the proximal descending aorta and PDA was dissected free. There is usually a small vessel over the PDA, which was sealed initially to prevent bleeding with the dissection. The recurrent laryngeal nerve could clearly be visualized, and care was taken throughout to avoid injury. The PDA was then carefully dissected free on the both sides. The ductus was test-clamped with an atraumatic grasper to ensure no negative hemodynamic events occurred with compression of the structure. The posterior port was changed to a 5-mm port, and the clip applier was introduced. A clip was then applied to the PDA close to the aorta (Fig. 2).
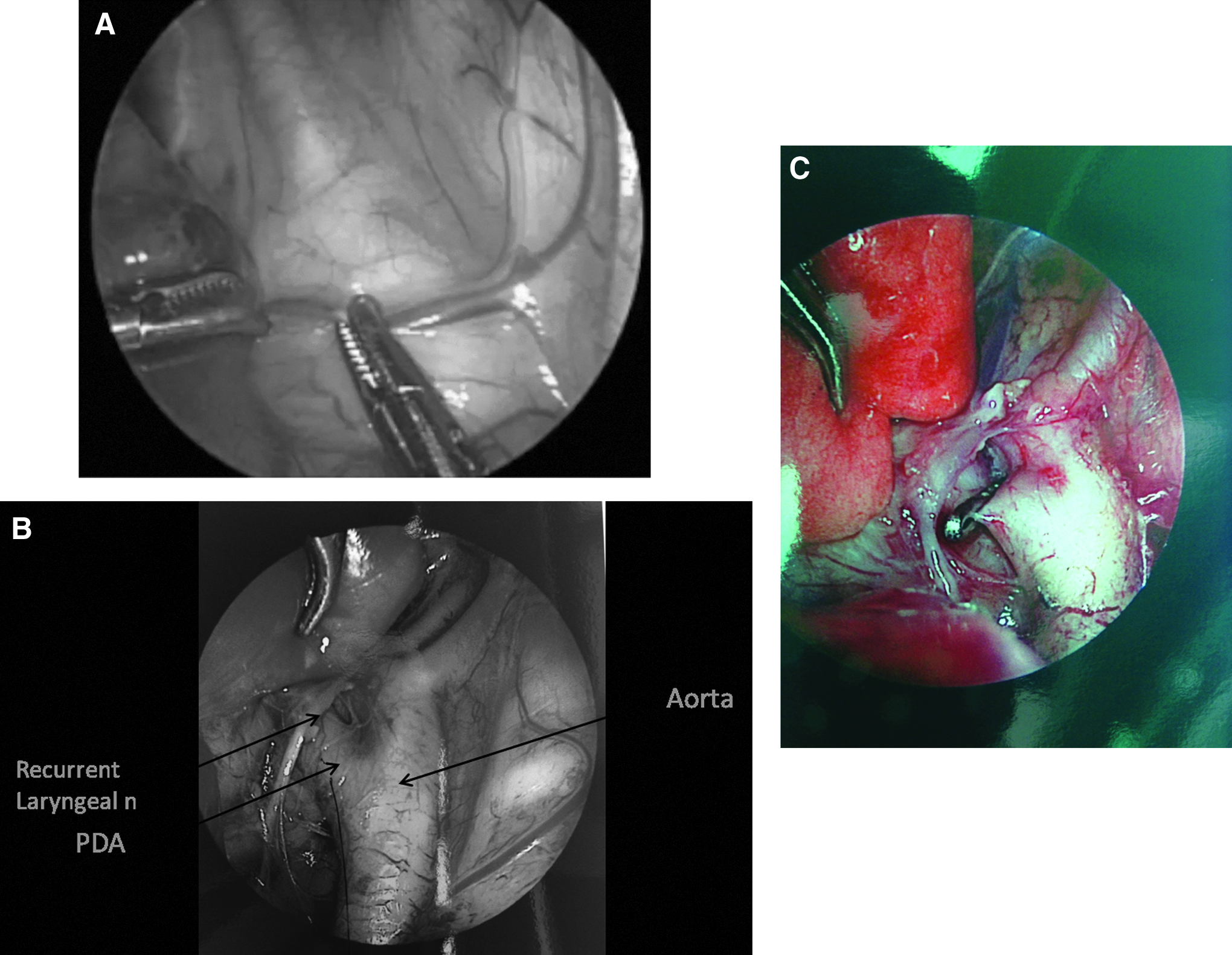
Intraoperative photographs of
For thoracoscopic vascular ring division, the room set-up, port placement, and monitoring were similar to those for thoracoscopic PDA ligation. In cases with a right arch, division of the ligamentum arteriosum was all that was necessary. The ligamentum was mobilized, divided between two clips or ties, and then divided. In cases of a double arch, the atretic left arch was mobilized and divided as well. A suture or vessel loop may be placed around the ligamentum and arch to provide traction and achieve length on the vessel to help with safe mobilization, ligation, and division. All vessels should be assumed to be patent and ligated accordingly. In all cases, the fibrous bands over the esophagus were then completely divided to alleviate any residual compression (Fig. 3).
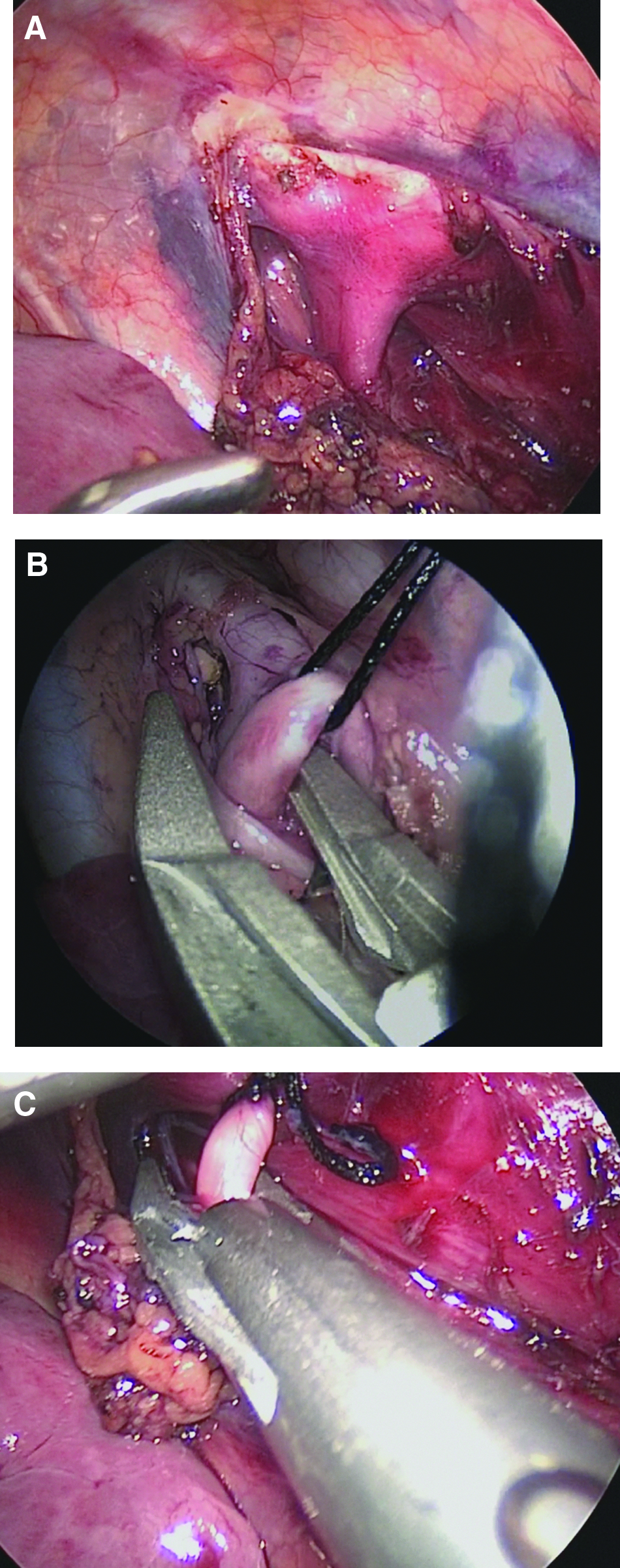
Intraoperative photographs of
Results
Ages ranged from 2 days to 17 years (mean, 18 months), and weights ranged from 2 to 60 kg (mean, 8.5 kg) for the thoracoscopic PDA group. Ages ranged from 6 weeks to 13 years (mean, 19 months), and weights ranged from 3.6 to 38 kg (mean, 10 kg) for the thoracoscopic vascular ring division group. In the thoracoscopic PDA group, the mean operative time was 36 minutes. Complications consisted of one death not related to the procedure, one conversion to open for a torn ductus, one recurrence requiring re-operative thoracoscopic repair, and one residual PDA requiring cardiac catheterization with occlusion (Table 1).
LOS, length of stay; PDA, patent ductus arteriosus.
Of the 80 patients in the PDA group, 38 patients (48%) weighed less than 5 kg. Sixteen patients were less than 2 kg, with 2 patients being 1 kg. The operative technique was the same for all weights. The larger-size children were more likely to be in the beginning of the series, whereas all of the patients in the last half of the series were less than 4 kg. The operative times were shorter (26.5 versus 46.7 minutes) in the <5 kg group compared with the >5 kg group, although they were also performed later in the series.
In the vascular ring group, 7 patients underwent division of the ligamentum only, and 4 underwent division of the atretic left arch and ligamentum. One patient had a complete double arch, and the procedure was converted to open after successful division of the ligamentum. In 2 cases, thoracoscopic exploration revealed no significant compression from the vascular ring, and dissection was stopped. Operative times ranged from 30 to 70 minutes, and length of stay ranged from 1 to 6 days (average, 2.8 days). All patients symptomatically improved after division of the vascular ring.
Discussion
Both PDA and vascular rings often require surgical treatment. Persistent PDAs can lead to congestive heart failure, failure to thrive, and pulmonary hypertension as well as an increase in the risk of endocarditis. As such, intervention should be pursued when detected. Since surgical ligation of PDAs was first successfully performed by Gross 1 in 1939, many large series have shown this technique to be safe and effective. Abnormalities of the aortic arch that encircle or impinge on the esophagus or trachea can lead to dysphagia or airway obstruction and respiratory distress. Division of the vascular structures compressing the trachea and/or esophagus is required to relieve the compression and provide symptomatic relief. Gross 2 first described this procedure in 1945.
However, both of these procedures have historically been performed through a thoracotomy with the potential for respiratory dysfunction and future musculoskeletal morbidity. Several authors have shown success with the thoracoscopic technique for both PDA ligation and vascular ring division.3–6 This series demonstrates the effectiveness of the minimally invasive approach for various types of thoracic vascular conditions that require surgical intervention. As surgeons become more comfortable with the approach, smaller patients can be operated on using the thoracoscopic technique. The magnification afforded by the telescope allows the anatomy to be clearly identified and dissected even in a small chest cavity. However, in patients weighing less than 1 kg, visualization and maneuverability become more difficult with the limited size.
For PDAs, percutaneous catheters have also been described to close the ductus by avoiding a thoracotomy.7,8 However, a high rate of persistent shunting and complications such as embolization and migration have been reported. 9 Finally, patients must be over 10 kg to be a candidate for this technique. Thus, the thoracoscopic approach appears to be more favorable at this time for PDA closure.
Conclusions
Thoracoscopic closure of PDAs and division of vascular rings are safe and effective techniques that minimize physiologic and cosmetic adverse effects. The minimally invasive technique affords magnification of the vascular structures and avoids the morbidity of a thoracotomy. For vascular rings, a double aortic arch without a dominant arch is the most technically challenging thoracoscopically.
Footnotes
Disclosure Statement
No competing financial interests exist.