
Abstract
Abstract
Objective:
For laparoscopic low anterior resection of the rectum, a small additional incision is needed to extract the specimen. We describe an adjustment technique, which inserted the anvil and extracted the specimen through transanal pathway.
Methods:
Between July 2010 and July 2012, 23 patients underwent laparoscopic rectal surgery with transanal anvil insertion and transanal prolapsing specimen extraction. All perioperative data and short-term outcomes were recorded in a database.
Results:
The mean patient age was 61.3 years (range 47–68 years). Of the 23 patients, 17 underwent resection for rectal carcinoma and 6 had tubulovillous adenomas. No intraoperative complications occurred. The mean operative time was 137 minutes (range 118–170 minutes). The distal margins, circumferential resection margins, and lymph node dissections were oncologically adequate for all malignancies. One patient experienced anastomotic leakage (4.3%), treated conservatively. One male patient with benign prostatic hyperplasia suffered from postoperative urinary retention. The average postoperative hospital stay was 11.3 days (range 7–21 days). No patients experienced anal dysfunction. At a median follow-up of 26 months, there were no tumor recurrences.
Conclusion:
The technique of transanal prolapsing specimen extraction for laparoscopic low anterior resection of the rectum is feasible and safe for selected patients.
Introduction
C
Patients and Methods
Patients
Twenty-three patients underwent laparoscopic low anterior resection of the rectum with transanal prolapsing specimen extraction between July 2010 and July 2012. Seventeen patients had rectal carcinoma, and 6 patients had tubulovillous adenomas. All pathologies were diagnosed by clinical examination, abdominal computed tomography, endoanal ultrasound, magnetic resonance imaging, and colonoscopy with biopsy.
Inclusion criteria were as follows: (1) no significant comorbidities; (2) normal sphincter function with no anal strictures; (3) tumors located 4–6 cm from the anal verge; (4) a histological grading of well differentiated or moderately differentiated for rectal cancer, with no distant metastases and a preoperative stage of T2 carcinoma; (5) a tubulovillous adenoma larger than 3 cm that was not able to be treated using endoscopy or transanal excision; (6) a body mass index (BMI) <25 kg/m2; (7) no history of previous rectal surgery; (8) all procedures were elective. Patients were excluded if their tumor covered over half of the rectal circumference or if they were obese, with a large amount of fat in the mesorectum.
All procedures were performed by a single surgeon who had done more than 300 laparoscopic rectal resections. Written informed consent was obtained from all patients, and the study was approved by the Ethics Committee of Shengjing Hospital of China Medical University.
Surgical technique
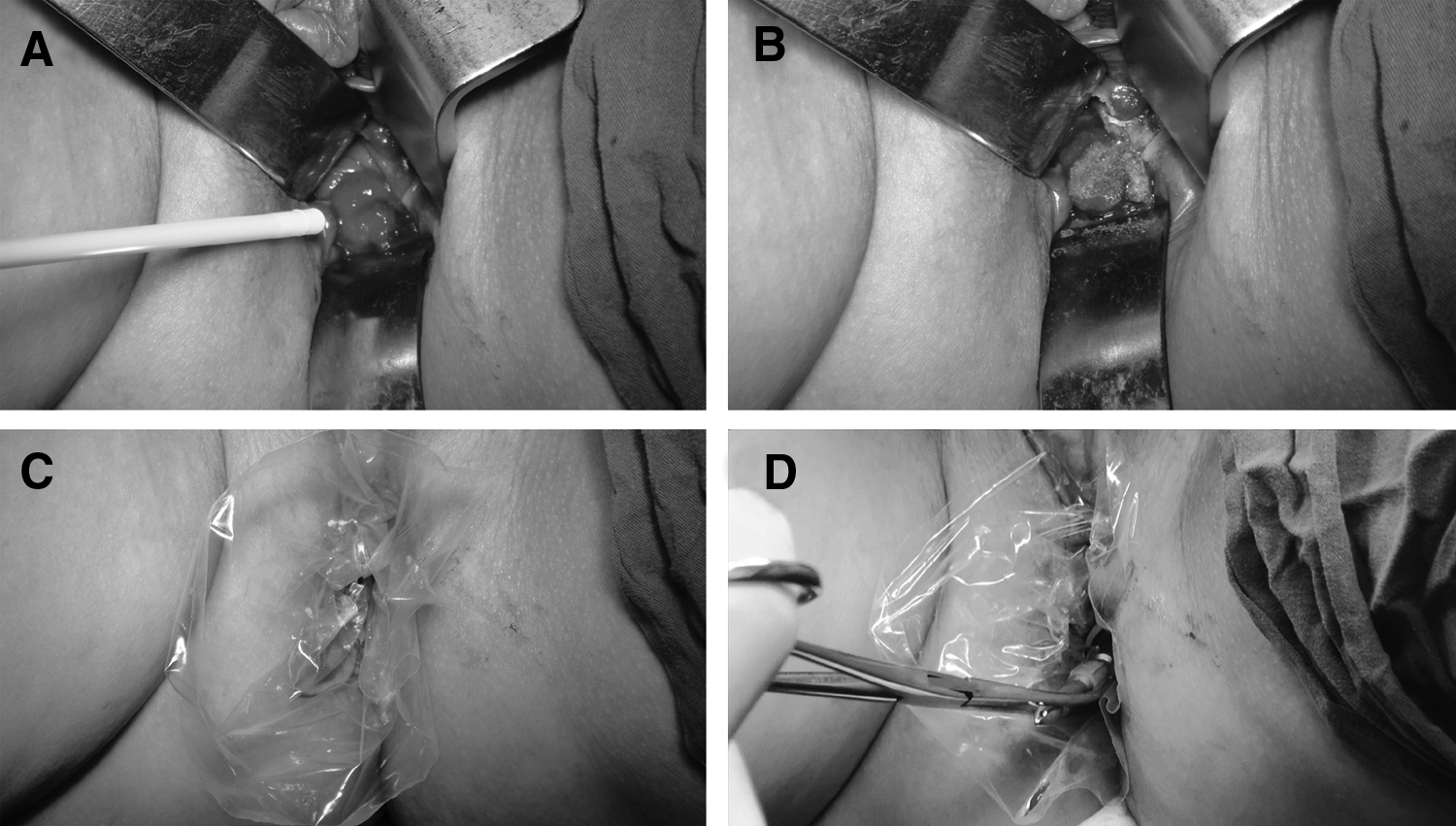
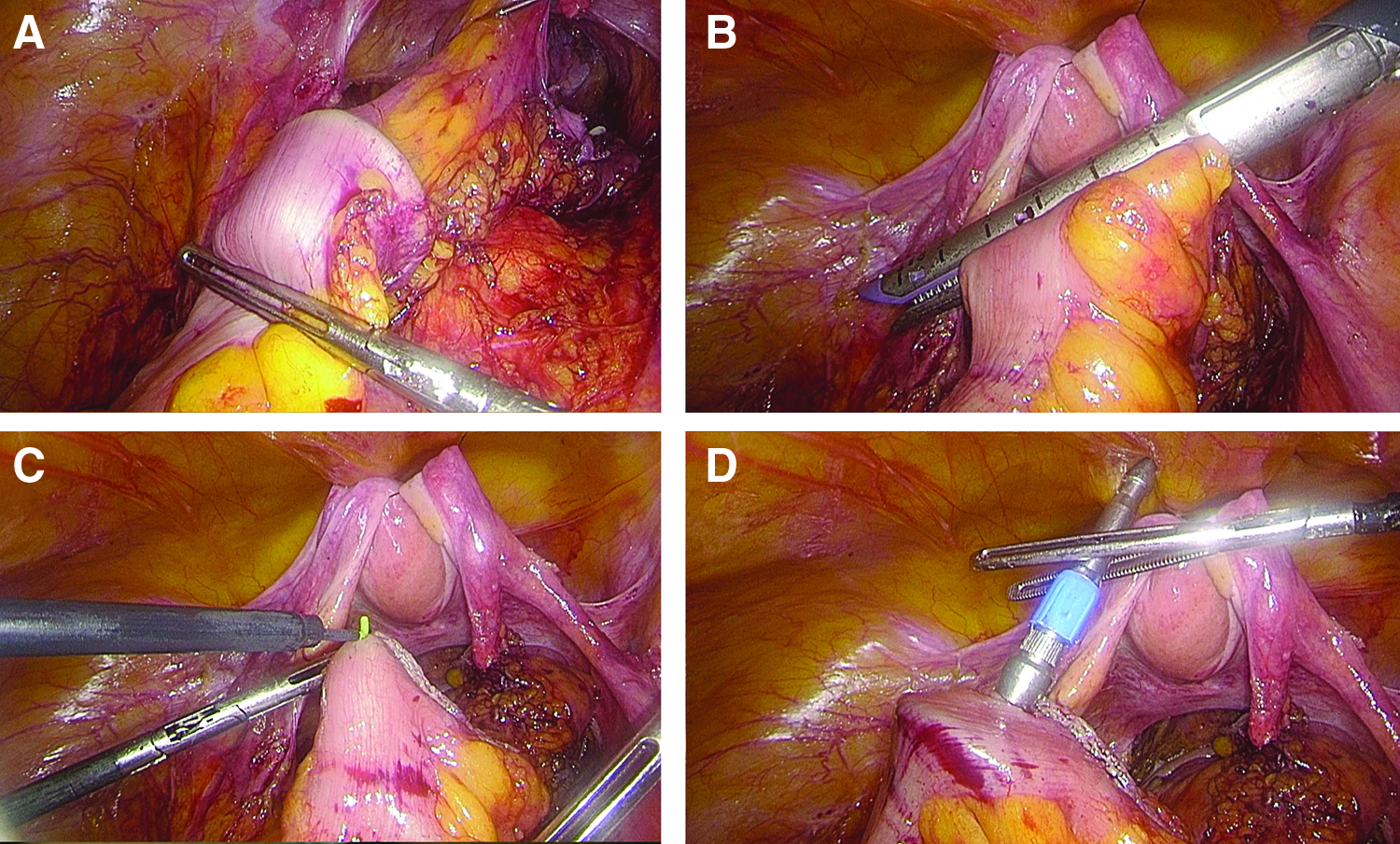
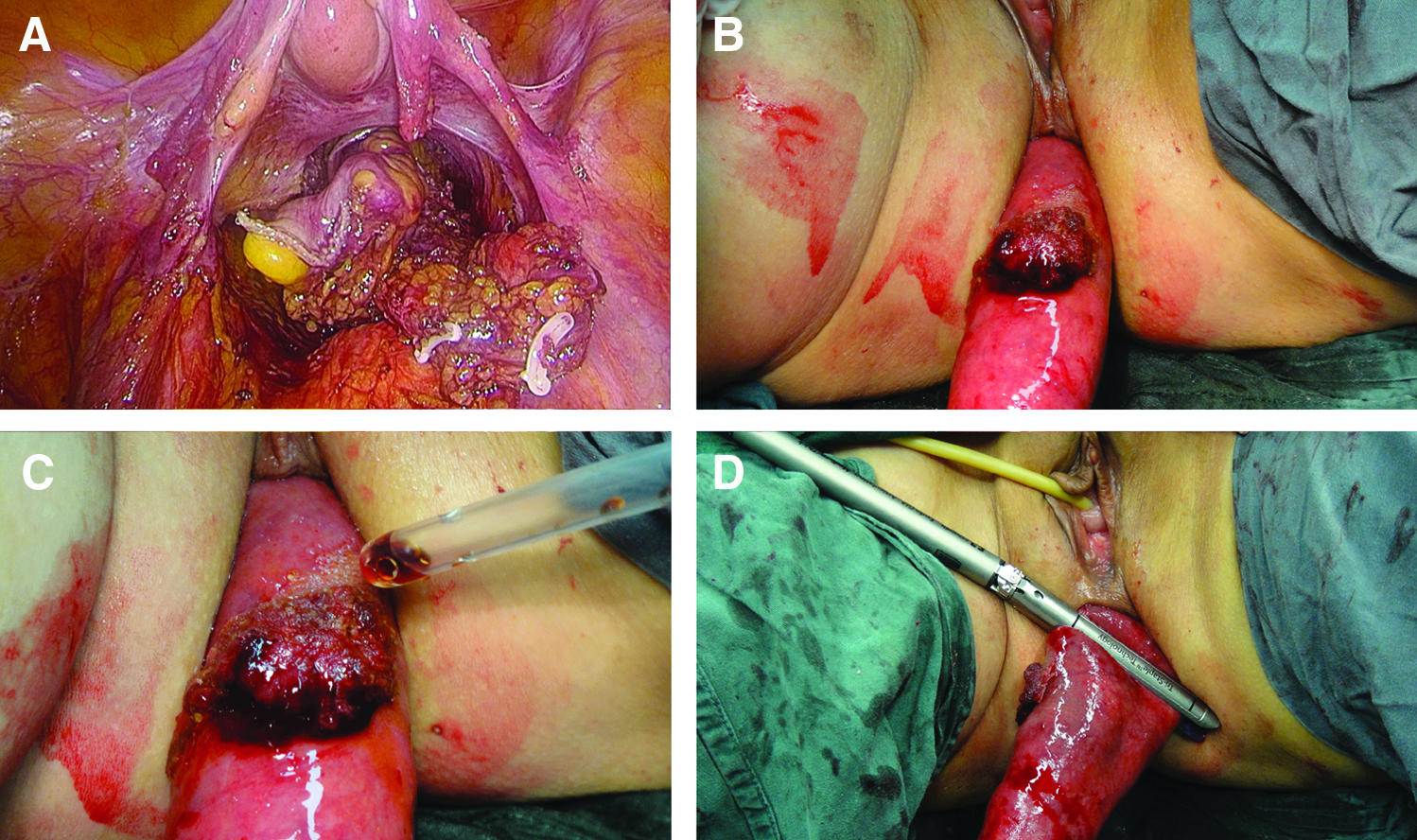
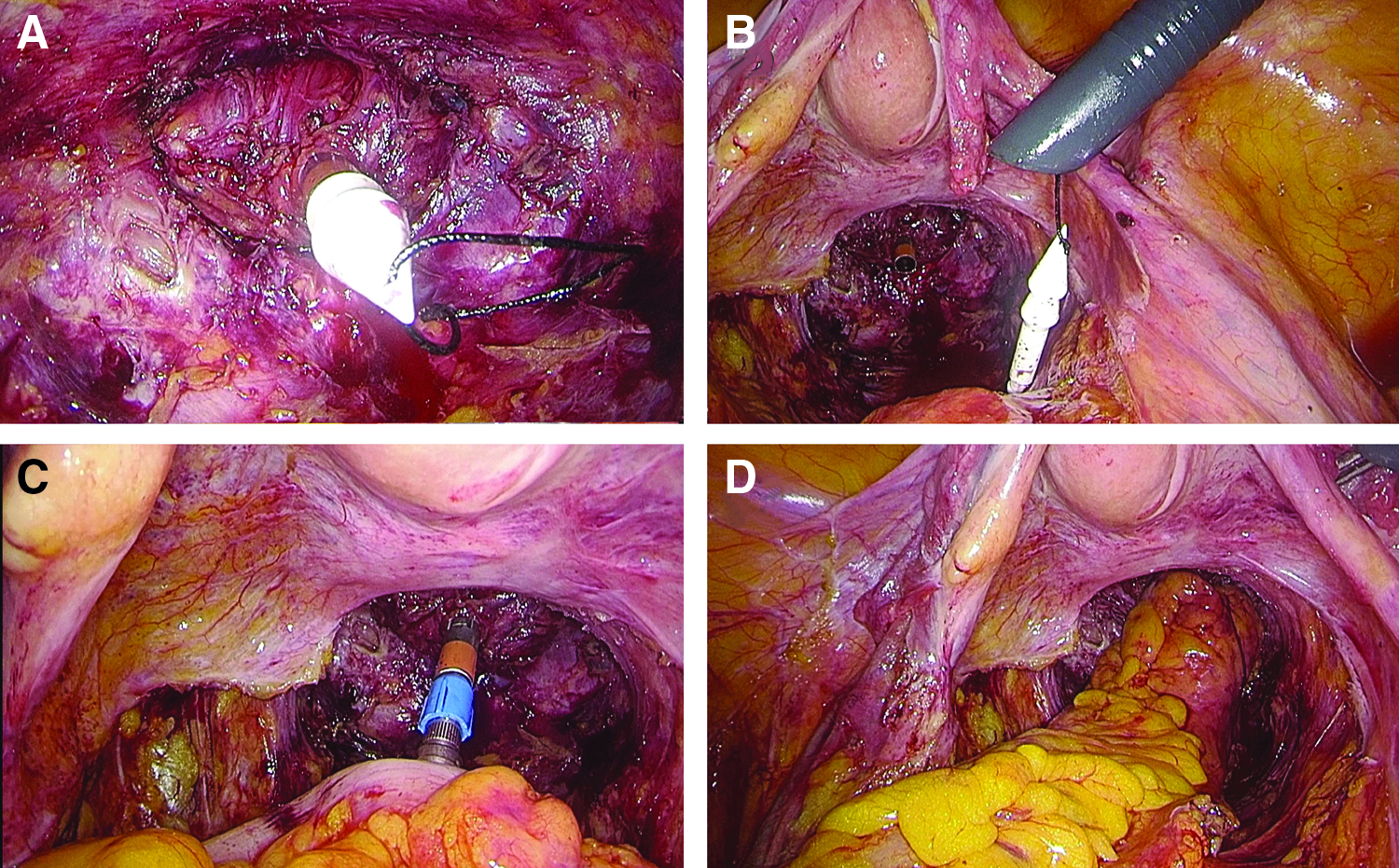
Under general anesthesia, patients were placed in a modified lithotomy position. Pneumoperitoneum was established through a transumbilical Veress needle. A 10 mm port was placed at the umbilicus, and a 12 mm port (Versaport™ PlusV2 bladed trocars; Covidien PLC, Mansfield, MA) was placed at the right iliac fossa; the other ports were VERSAPOINT V2 5 mm ports (Tyco Healthcare Group LP, Norwalk, CT). Trocar positioning is shown in Figure 1. The inferior mesentery pedicle was isolated in patients with malignant disease. For benign disease, the left colic artery was preserved. The splenic flexure did not need to be mobilized in any patient. The mesentery was dissected to ensure adequate resection without tension for the later coloanal anastomosis. Subsequently, a standard total laparoscopic mesorectal excision was performed down to the levator ani muscle plane. The proximal resection line was placed 10 cm above the tumor. Then, the sigmoid mesentery was dissected, and the relevant area of bowel was completely freed from the mesocolon. The lumen at this site was occluded with a pair of atraumatic laparoscopic bowel forceps. The surface of the tumor was painted with an n-Butyl-2-cyanoacrylate Biogel compound (Compont Medical Adhesive; Beijing Compont Medical Devices Co. Ltd., Beijing, China) under direct transanal visualization. This Biogel formed a protective membrane that prevented tumor cell exfoliation during the procedure; we have previously described this technique. 11 Distal rectal lavage was then carried out using diluted povidone–iodine solution and saline. The plastic laparoscopic camera bag, about 10 cm in length, was introduced through the anus and advanced beyond the tumor to protect the oncological specimen. Through the plastic bag, the anvil of a 28 or 31 mm circular stapler (Premium Plus CEEA™; Covidien PLC) was pushed transanally into the proximal intended resection line using sponge forceps (Fig. 2). The bowel was then divided using a 60 mm endoscopic linear stapler (Endo GIA™ Ultra Universal Stapler with purple medium/thick cartridges; Covidien PLC). The shaft of the anvil punctured the bowel at the antimesenteric border of the stapled line and was gently pulled out through the enterotomy (Fig. 3), leaving the proximal part of the anastomosis ready for use. The anus was carefully dilated, a grasping forceps was inserted from the anus to hold the stump of the distal rectum, and the distal rectum was gradually everted and pulled outside the body. The prolapsed rectum was carefully irrigated with diluted povidone–iodine solution and saline. The distal rectum was transected at the appropriate site under direct visualization using the same 60 mm endoscopic linear stapler with a new cartridge (Fig. 4). Frozen pathology was routinely performed to confirm the integrity of the distal margin. The stump of the rectum was then retracted through the anus into the pelvis. The spike of the stapler was secured with a 2–0 silk suture at the hole in its tip, so it could be removed conveniently, and the stapler was then inserted transanally to the level of the staple line. The spike punctured the stump of the rectum at the middle of the staple line and was then removed and delivered from the pelvis through the 12 mm port. The anastomosis was created intracorporeally using a triple-stapled end-to-end technique (Fig. 5). All anastomotic doughnuts were complete. Protective ileostomy was not required in any patient. All patients had two closed suction drain tubes inserted into the pelvic cavity. All surgical specimens were examined pathologically (Fig. 6).
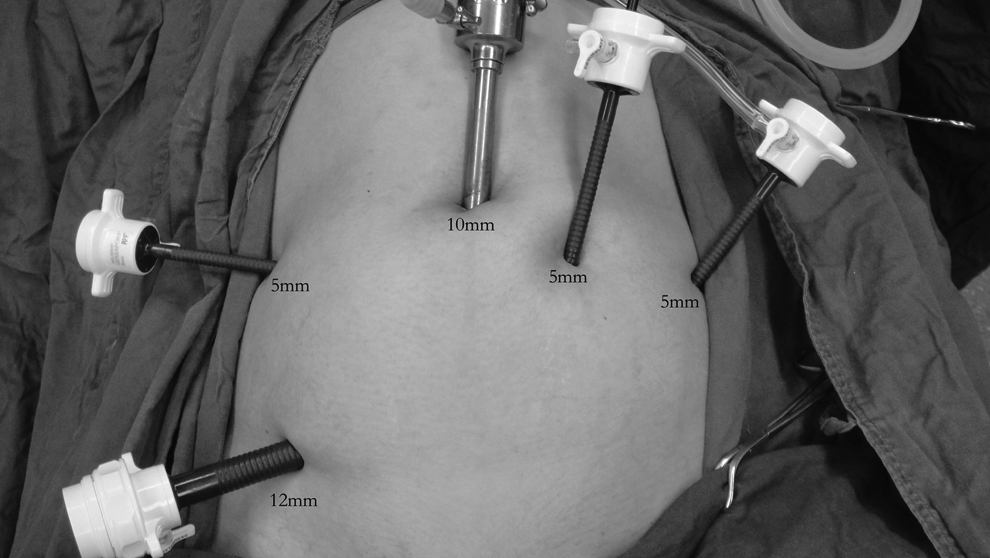
Trocar size and position.
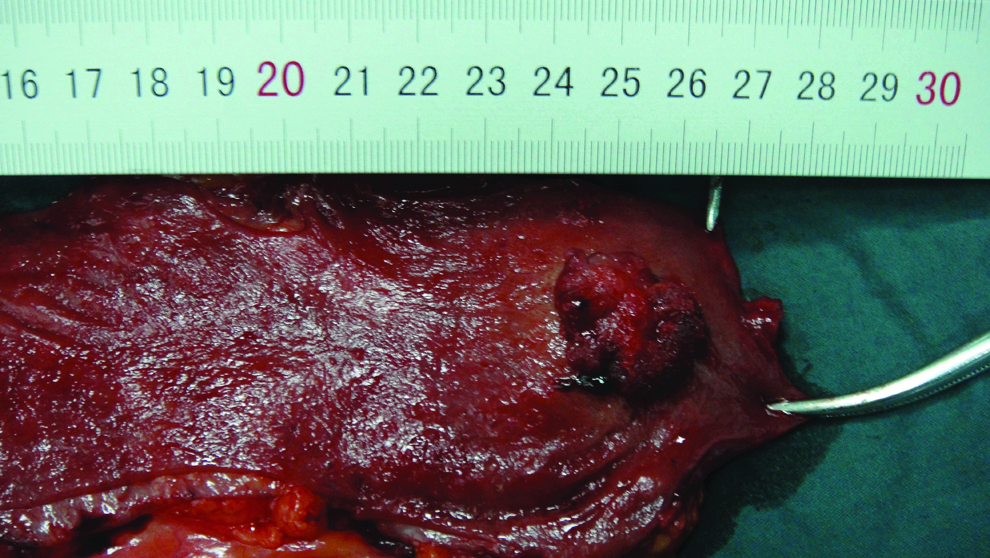
Pathologic examination of the specimen.
Postoperative care
Oral liquids were started on postoperative day 1, and an oral soft diet was made available 48 hours after surgery. All patients received intravenous flurbiprofen axetil, 50 mg every 12 hours, for 3 days.
Incontinence was assessed 1 month after surgery using the continence score of Jorge and Wexner (Wexner score). 12 Anal sphincter function was evaluated preoperatively and at 3 and 12 months after surgery using the PC-Polygraf HR function system (CTD-Synectics, Stockholm, Sweden). All patients were followed every 3 months for 2 years postoperatively, then every 12 months thereafter.
Statistical analysis
Continuous variables are presented as means and standard deviations (SD), and categorical variables are expressed as percentages. The parameters of anal sphincter function before and after surgery were compared using one-way repeated samples measures analysis of variance (ANOVA), and the Bonferroni test was used for posttest analysis. All analyses were performed using Statistical Package for the Social Sciences (SPSS) software, version 13.0 (SPSS, Inc., Chicago, IL). A P value of less than .05 indicates statistical significance.
Results
The described technique was attempted in 23 patients (9 males and 14 females) with a mean age of 61.3 years (range 47–68 years) and a mean BMI of 23.2 kg/m2 (range 20.7–24.8 kg/m2) (Table 1). Three patients had undergone previous abdominal surgery (cholecystectomy, hysterectomy, and appendectomy). No adverse events occurred during surgery. For 74% (17/23) of patients, two cartridges were adequate to divide the proximal and distal bowel, results that are similar to the conventional minilaparotomy specimen extraction technique. The mean operating time was 137 minutes (range 118–170 minutes), and the mean blood loss was 25 mL (range 10–50 mL). The mean length of the extracted specimen was 18.4 cm (range 15.1–22.1 cm), and the mean distal resection margin from the tumor edge was 1.8 cm (range 1.1–2.3 cm) (Table 2).
BMI, body mass index.
For 17 patients with rectal cancer.
On histological examination, all malignant tumors had negative distal margins, negative circumferential resection margins, and an adequate lymph node dissection. The TNM classification of rectal carcinoma was stage I in 13 patients (T1N0M0 in 2 and T2N0M0 in 11), stage II (T3N0M0) in 2 patients, and stage III (T2N1M0) in 2 patients. One patient experienced a minor anastomotic leakage on postoperative day 7, confirmed by stool leaking from the surgical drain. He was managed conservatively and was discharged after 14 days. Another male patient with a history of benign prostatic hyperplasia suffered from urinary retention, which was successfully treated using indwelling catheterization and oral tamsulosin hydrochloride sustained release capsules for 7 days. The mean time to first ambulation and first passage of flatus was 9 and 55 hours, respectively. The average postoperative hospital stay was 11.3 days (range 7–21 days). There were no readmissions within 30 days. The trocar sites healed very well with almost no scarring. Two patients in stage III treated with capecitabine and oxaliplatin (XELOX) as adjuvant therapy. No patients complained of anal dysfunction or incontinence, and the median Wexner incontinence score 1 month after surgery was 2.7. All patients were followed for 21–36 months (mean 26 months) (Table 2). There was no local recurrence or metastasis detected.
Neither the maximum resting nor squeezing anal pressure at 3 and 12 months postoperatively was significantly different than their preoperative values (all P > .05). The resting and squeezing vector volumes were lower at 3 months (all P < .05) and recovered to preoperative levels by 12 months (all P > .05) (Table 3). The anal inhibitory reflex was positive in 65.2% of patients (15/23) at 3 months and in 91.3% (21/23) at 12 months.
Compared with preoperative, P < .05.
MRAP, maximum resting anal pressure; MSAP, maximum squeezing anal pressure; RVV, resting vector volume; SVV, squeezing vector volume.
Discussion
Conventional laparoscopic anterior resection of the rectum requires an abdominal mini-incision to extract the specimen and to introduce the anvil of the stapler into the proximal colon for intracorporeal anastomosis. Although this incision is shorter than that used in traditional open surgery, wound complications are not rare. The incidence of infection at the extraction site ranges from 3.1% to 17.2%.13–17 A recent randomized controlled trial by Lauscher et al. 16 showed that the rate of surgical site infection in laparoscopic-assisted colorectal resection using plastic wound ring drapes is as high as 12.8%. Incisional hernia after laparoscopic colorectal surgery is also not uncommon, with rates of 7.8%–24.3% reported.13,18 Winslow et al. 13 determined that the extraction site accounts for 85.7% of all wound complications in patients undergoing laparoscopic colon resection. It appears that laparoscopic colorectal surgery, as currently performed, does not affect a reduction in wound complications compared with open surgery because of the high incidence of extraction site-related complications. 13 Therefore, avoiding minilaparotomy has the potential benefit of reducing incisional postoperative complications, which could lead to faster patient recovery.
Recently, the concept of natural orifice surgery has prompted research into the best method of avoiding this minilaparotomy. The technique of natural orifice specimen extraction was described by Franklin et al. as early as 1993 19 ; many modified techniques have subsequently been recommended.5,6,10,20–23 Morris et al. reported a series of 179 patients who underwent laparoscopic low anterior resection with transanal specimen extraction for rectal cancer. The intraoperative information, postoperative complications, and 2-year follow-up outcomes were acceptable. 24 There are two main access sites for NOSE in laparoscopic colorectal surgery: through the anorectum and through the vagina. Transvaginal extraction, of course, is applicable in female patients only and requires an incision through a normally uninvolved organ. 25 We do not prefer the transvaginal route, as only sexually active women patients are eligible, and there is a risk of tumor implantation along the colpotomy site. In most studies on the NOSE technique, the stapler anvil is introduced into the peritoneal cavity through the anus and the opened rectum, with the specimen retrieved using the same passage. The anvil is also inserted into the proximal colon to prepare the anastomosis at the opened sigmoid colon. One possible concern of this approach is the risk of bacterial contamination leading to postoperative intraperitoneal abscess. Leroy et al. reported that peritoneal fluid cultures were positive for polybacterial growth in 16 of 16 patients tested; they also demonstrated the expected spectrum of microbial pathogens. 26 We decided that this technique was not optimal and attempted a new procedure that would facilitate anvil placement and avoid additional abdominal incisions.
To the best of our knowledge, there are no other reports of laparoscopic rectal surgery using the technique of both transanal anvil placement and transanal prolapsing specimen extraction. Our patients had different indications for using this combined technique, in which the anus is the natural orifice used, both for specimen extraction and anvil delivery. 27 We were initially concerned that this new technique might result in anal leakage, but this fear was not borne out by our results.
The mean postoperative hospital stay in our patients (11.3 days) is longer than that reported by other authors for the NOSE technique.8,20,24 This may be due either to surgical complications or to the differing socioeconomic backgrounds of patients and systems of medical insurance in China. For example, readmission within 15 days of hospital discharge is not covered under the original procedure by the Chinese insurance system.
Transanal placement of the stapler anvil together with transanal prolapsing specimen extraction technique in laparoscopic rectal surgery does have potential advantages. Transanal placement of the anvil could avoid exteriorization of healthy bowel and contamination of the peritoneal cavity. The prolapsing technique can help surgeons transect the distal rectum at the appropriate location—when the distal divided line is very low in the pelvis, it becomes more difficult to achieve rectal transection laparoscopically. In addition, for small-stage T2 tumors, it can be difficult to determine the inferior margin; the prolapsing technique allows for direct extracorporeal visualization. This technique is minimally invasive in a very real sense, with the potential for less stress on the patient and a shorter hospital stay. Undoubtedly, avoiding the minilaparotomy incision eliminates the risk of complications at that wound site. The excellent cosmetic outcome is also attractive, although it is not the primary purpose of this treatment. Factors limiting the applicability of this technique include the presence of anal strictures, a bulky tumor or mesorectum, and stenosis of the rectum greater than half of its circumference.
The potential for tumor implantation following transanal passage of the anvil and prolapsing of the distal rectum must be considered. Before anvil insertion, spraying the surface of the tumor with a Biogel compound under direct visualization may create a protective membrane over the tumor. Using the plastic camera bag as a sleeve for the introduction of the anvil may also provide protection against tumor cell seeding. With these precautions, subsequent steps in the procedure can be carried out without touching the tumor directly, possibly reducing the risk of seeding. Colorectal washout before transection and after prolapsing is necessary for this prevention; however, there is still a risk of remnant tumor cells remaining.28,29 Nishimura et al. instruct that objects, such as forceps, that come into contact with the rectal mucosa should not subsequently touch the peritoneum. 9 With our technique, laparoscopy is used to dissect the portion of the rectum intended for prolapse from the pelvic floor surrounding the anal canal. The distal rectum is everted gently and gradually to avoid squeezing the tumor or splitting the rectal wall. These steps are an attempt to eliminate the risk of cancer cell exfoliation, implantation, and subsequent local recurrence. Most importantly, we only perform this technique in patients with benign disease or relatively small T2 carcinomas. This technique may not be feasible in patients with locally advanced cancers or very large and bulky tumors, which are associated with a high risk of cancer cell implantation.
Digital dilation of the anus with passage of a bulky specimen may lead to compromised sphincter function. Fukunaga et al. report that rectal eversion does not appear to damage anal function. 30 In our experience, we recommend step-by-step dilation of the anal sphincter and avoiding rough eversion of the distal rectum; good anesthesia and relaxation are also necessary. Air trapping within the isolated specimen may increase its volume and hamper transanal extraction; therefore, pneumoperitoneum should be released before the rectum is everted. To avoid damaging the anal sphincter, we choose to abandon transanal extraction of the specimen if there is great resistance to its passage. In our small series, no patients experienced postoperative anal incontinence.
For low colorectal or coloanal anastomoses, ∼30%–60% of patients experience functional disturbances, collectively termed as anterior resection syndrome.31,32 Most authors believe this syndrome is caused by injury of the anal sphincter and mucosa. We were concerned about inducing this syndrome with transanal specimen extraction, but this was not borne out by our results. Anorectal vectorial manometry showed normal maximum resting and squeezing anal pressures 3 months after surgery, and no patients complained of anal dysfunction or incontinence. Further prospective studies should be performed, with a large number of patients, a long follow-up period, and anal manometry evaluation, to assess the risk of damaging anal sphincter function with this technique.
Conclusion
The current preliminary experience at our center is too limited to draw wide ranging conclusions, but we do believe that laparoscopic low anterior resection of the rectum with transanal anvil insertion and transanal prolapsing specimen extraction is feasible, safe, and oncologically acceptable for selected patients. This technique modification has the potential advantages of eliminating the minilaparotomy incision traditionally used and enhancing recovery. Further randomized controlled trials with long-term follow-up are necessary to evaluate whether this procedure is an appropriate option for patients undergoing laparoscopic low anterior resection of benign or malignant rectal disease.
Footnotes
Disclosure Statement
No competing financial interests exist.