
Abstract
Abstract
Background:
Although the cuff of tracheal tubes can reduce airflow leakage and prevent aspiration, excessive intracuff pressure can cause tracheal mucosal injury. Robot-assisted laparoscopic surgery (RALS) can increase intracuff pressure by the Trendelenburg position and pneumoperitoneum. The aim of our current study was to investigate the effect of tracheal cuff shape on the intracuff pressure increase by comparing two different-shaped cuffs during RALS.
Materials and Methods:
Ninety-eight patients undergoing RALS were allocated randomly into two groups (tapered-shaped cuff [TSC] and cylindrical-shaped cuff [CSC] groups). The intracuff pressure was measured at nine specific time points: after intubation, immediately after surgical preparation (Trendelenburg position with CO2 insufflation), at 5, 10, 15, 30, 60, and 90 minutes after surgical preparation, and at the end of surgery. Postintubation airway symptoms were measured by assessing sore throat, hoarseness, and excessive cough 1 hour after postanesthesia care unit admission.
Results:
Intracuff pressure significantly increased during surgery in both groups. The trend of intracuff pressure change decreased in the TSC group compared with the CSC group, although no statistically significant changes were found (P=.450). Also, there were no statistically significant differences in the postintubation airway symptom between the two groups.
Conclusions:
The TSC tube has a tendency to decrease intracuff pressure change compared with the CSC tube during RALS. However, neither of them was beneficial in preventing intraoperative intracuff pressure increase during RALS.
Introduction
T
An intracuff pressure higher than 30 cm of H2O can compromise mucosal capillary blood flow and cause mucosal erosion.2,4 The type of tracheal cuff affects the intracuff pressure, as well as exerting an air-sealing effect.1,5 Compared with the conventional cylindrical-shaped cuff (CSC) (Mallinckrodt™ Hi-Lo™; Covidien, Norwalk, CT) tube, the tapered-shaped cuff (TSC) (Taperguard™; Covidien) tube may improve the air-sealing effect, 1 yield a smaller mucosa contact area, 3 and prevent nitrous oxide (N2O)–related cuff pressure increase 6 during general anesthesia.
Robot-assisted laparoscopic surgery (RALS) has many advantages over conventional open abdominal surgery, such as a shorter hospital stay and less postoperative pain.7,8 In RALS, not only is the patient placed in the Trendelenburg position, but also pneumoperitoneum is induced via CO2 insufflation to achieve a good surgical field. However, CO2 insufflation together with the Trendelenburg position may increase intrathoracic pressure, thereby increasing both airway and intracuff pressure.9,10 Consequently, risk of excessive intracuff pressure can be increased during RALS compared with other types of surgery, including open abdominal surgery, in the supine position. Therefore, special considerations would be needed to prevent an increase in intracuff pressure during RALS.
Although the TSC tube has shown some benefits, little is known about the effect of the tracheal cuff shape on the intracuff pressure change during RALS. Therefore, we hypothesized that intracuff pressure would be increased less in using the TSC tube than in using the CSC tube in RALS. In our present study, therefore, we aimed to compare the change in intracuff pressure between conventional CSC and TSC tubes during RALS with the patient under general anesthesia. Moreover, we investigated postintubation airway symptoms (PIASs) to evaluate the clinical effect of tracheal cuff shape.
Materials and Methods
Patients
This randomized controlled clinical trial was performed at Asan Medical Center (Seoul, Korea) between July 2012 and April 2013. After approval was received from the Institutional Review Board of Asan Medical Center, written informed consent was obtained from all patients. Patients less than 20 years of age, with any history of severe cerebral, cardiovascular, or pulmonary disease, showing an abnormal pulmonary function test or obesity (body mass index ≥30 kg/m2), and/or a current smoker (including ex-smokers for less than 1 year) were excluded from the study. To attenuate the bias of the surgical procedure on the intraoperative intracuff pressure change, the type of surgery was limited to robot-assisted laparoscopic prostatectomy (RALP) or robot-assisted lower anterior resection (RALAR). Patients were randomly allocated into two groups (CSC and TSC) by a computer-generated random table. In the CSC group (n=48), patients were intubated using a conventional high-volume, low-pressure tracheal tube with a CSC. In the TSC group (n=48), a TSC tube was used for tracheal intubation.
Anesthesia protocol
None of the patients received premedication. Intraoperative monitoring included arterial blood pressure, electrocardiography, peripheral oxygen saturation, esophageal temperature, and end-tidal carbon dioxide. General anesthesia was induced with thiopental sodium (5 mg/kg), and rocuronium bromide (0.6 mg/kg) was used to facilitate tracheal intubation. After intubation, the tracheal tube cuff was inflated with air using a manometer, and the intracuff pressure was adjusted to 25 cm of H2O as the baseline. Anesthesia was maintained by administration of 2–3 vol% sevoflurane and 2 L/minute of medical air with 50% oxygen. Fluid management was performed by continuous infusion of crystalloid solution at 4–6 mL/kg/hour and intermittent bolus (50 mL) administration of colloid solution (Voluven®; Fresenius Kabi, Bad Homberg, Germany) repeatedly when mean arterial pressure was measured below 65 mm Hg. Mechanical ventilation was performed with a tidal volume of 8 mL per ideal body weight and a respiratory rate of 8–15 breaths/minute to maintain 30–35 mm Hg of end-tidal CO2 during surgery. During surgery, CO2 was continuously insufflated to maintain intraabdominal pressure at 15 cm of H2O. At the end of surgery, patients were gently extubated and transferred to the postanesthesia care unit (PACU). An hour after PACU admission, fully alert patients were asked if they had symptoms of sore throat, hoarseness, and/or excessive cough. In the PACU, an intravenous bolus of fentanyl (0.5–1 μg/kg) was administered when the patient's pain was assessed at more than 5 points by visual analog scale.
Outcome measurement
Intracuff pressure was measured with a manometer (VBM cuff pressure gauge; VBM Medizintechnik GmbH, Sulz am Neckar, Germany). In both groups, the cuff was initially inflated to achieve an intracuff pressure of 25 cm of H2O as a baseline value. Then, the manometer was connected to the pilot balloon of the tracheal tube via a T-port. Intracuff pressure was measured at nine specific time points: after intubation, immediately after surgical preparation (Trendelenburg position with CO2 insufflation), at 5, 10, 15, 30, 60, and 90 minutes after surgical preparation, and at the end of surgery.
For evaluation of PIAS, fully awake patients at 1 hour after PACU admission were asked about their symptoms by an independent observer unaware of the patient groups. The presence of three airway symptoms was assessed: sore throat, dysphagia, and hoarseness (0=no discomfort, 1=presence of discomfort with any severity).
Statistical analysis
In a pilot study, the minimum detectable mean difference between the two cuff types was 2.5 cm of H2O, and the standard deviation was 4.2 cm of H2O. From this result, we calculated that 44 patients were required in each group to detect differences with a power of 0.8 and with a type I error of 0.05. Considering a 10% measurement error, we finally enrolled 96 patients. Statistical analyses were performed using SPSS version 13.0 software (SPSS Inc., Chicago, IL). A normality test was performed using the Shapiro–Wilk test. Two-way repeated-measure analysis of variance was used to compare the intracuff pressure between the two groups at each time point, as well as the intracuff pressure change during surgery. For post hoc analysis, we used Tukey's method. A Mann–Whitney rank sum test or t test was used to compare numerical variables of demographics or intraoperative data. A Fisher's exact test or chi-squared test was used to compare the categorical data of postoperative outcomes between the two groups. All data were expressed as numbers (%) or mean±standard deviation values. P<.05 was considered statistically significant.
Results
In total, 96 patients undergoing RALP or RALAR were enrolled; none dropped out (Fig. 1). Patient demographics and intraoperative data are shown in Table 1. There were no differences between the CSC and TSC groups in terms of patient characteristics and preoperative pulmonary function test results. In addition, the proportion of surgery type and intraoperative data were similar between the two groups. The change in intracuff pressure is shown in Figure 2. After CO2 insufflation and the Trendelenburg position, the intracuff pressure increased significantly compared with that of baseline, and increased cuff pressure was maintained during surgery. The intracuff pressure of the TSC group tended to decrease compared with that of the CSC group at each time point during surgery, but there were no statistically significant differences between the two groups (P=.450) (Fig. 2).
CONSORT flow chart.
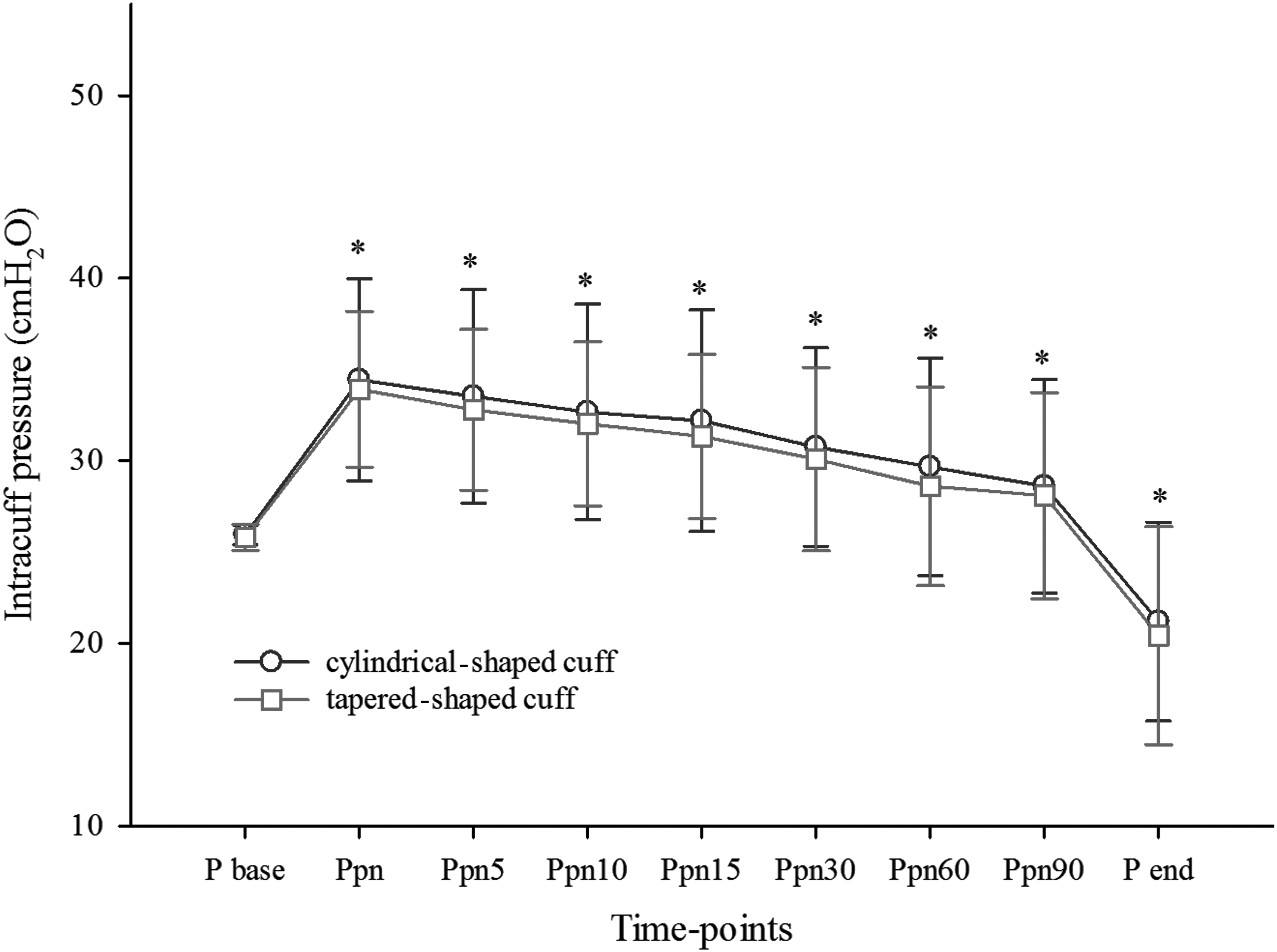
Intracuff pressure (P) changes during surgery. The intracuff P value measured at all time points showed significant changes compared with the baseline value. The trend of intracuff P change decreased in the tapered-shaped cuff group compared with the cylindrical-shaped cuff group, although no statistically significant changes were found (*P=.450).
Data are mean±standard deviation values or numbers as indicated.
CSC, cylindrical-shaped cuff; F, female; FEV1, forced expiratory volume in 1 minute; FVC, forced vital capacity; M, male; RALAR, robot-assisted lower anterior resection; RALP, robot-assisted laparoscopic prostatectomy; TSC, tapered-shaped cuff.
Regarding postoperative outcomes, the incidence of PIAS is also shown in Table 2. Three symptoms (sore throat, hoarseness, and cough) were assessed at 1 hour after PACU admission. Although overall complications were more frequently observed in the CSC group than in the TSC group (11 [23.9%] versus 7 [15.2%] cases), there were no statistically significant differences in the symptoms. Between the two groups, the analgesic requirement in the PACU was similar (101.13±13.16 μg in the CSC group versus 100.0±18.68 μg in the TSC group, P=.43).
Data are number (%).
CSC, cylindrical-shaped cuff; PACU, postanesthesia care unit; TSC, tapered-shaped cuff.
Discussion
In our present study, intracuff pressure increased after CO2 insufflation and the Trendelenburg position in RALS. The TSC tube has a tendency to decrease intracuff pressure change compared with the CSC tube during RALS, although no statistically significant changes were found. However, neither of them was beneficial in preventing intraoperative intracuff pressure increase during RALS. The incidence of PIASs at PACU, such as sore throat, hoarseness, and cough, was not found to differ between the CSC and TSC tubes. This is to our knowledge the first clinical report to compare the effect of tracheal cuff shape on the intracuff pressure change during RALS.
Tracheal cuffs are inflated to make contact with the tracheal wall, thereby producing a sealing effect and preventing the aspiration of oral contents. 4 However, increased intracuff pressure can result in mucosal injury, and several techniques, such as use of a N2O/oxygen mixture or isotonic saline and a gas-barrier cuff, have been applied to minimize tracheal mucosal injury. 11 The mucosal blood flow in the tracheal wall can be compromised at 30 cm of H2O and totally obstructed at 50 cm of H2O. 4 Thus, intracuff pressure should be maintained below 30 cm of H2O during mechanical ventilation. In case of overpressure, the tracheal mucosa may cause ischemic injury that manifests as erythema, erosion, and ulceration.2,11 Moreover, ischemic mucosal injury has been correlated with the severity of clinical symptoms. 2 In RALS, pneumoperitoneum via CO2 insufflation is applied, and, particularly in RALP or RALAR, the Trendelenburg position is also required to achieve a good surgical field. 9 The combination of the Trendelenburg position and CO2 insufflation can increase intrathoracic pressure, thereby increasing the external pressure on the patient's trachea. Therefore, these maneuvers may increase the risk of tracheal mucosal injury during surgical procedures, even with normal intracuff pressure in the supine position or without N2O use.
TSC tubes have been reported to have a good sealing performance.12,13 In a previous study using model trachea, TSC tubes showed a reduced airflow leakage at lower peak inspiratory pressure 1 and a reduced intracuff pressure increase after N2O exposure. 6 Fewer longitudinal folds formed between the cuff membrane and trachea wall, which was suggested to cause less of a pressure increase with N2O diffusion. In the present study, we assumed that the TSC tube would show a reduced intracuff pressure increase and have a smaller mucosal contact area than the conventional CSC tube in clinical situations that can lead to increased airway pressure such as RALS. The trend of intracuff pressure change decreased in the TSC group compared with the CSC group, although no statistically significant changes were found (P=.450). However, both TSC and CSC tubes have no favorable effect in preventing intraoperative intracuff pressure increase during RALS. Therefore, care should be taken for the monitoring of the intracuff pressure during RALS.
PIASs such as sore throat, hoarseness, and cough can be related to the presence of intubation and the intracuff pressure increase.3,14,15 Management to reduce intracuff pressure during mechanical ventilation can help to reduce PIAS.2,15 In our present study, the incidences of overall and individual PIASs were similar between the two groups. Because of relatively small sample size and analgesics that were administered in the PACU, it could be possible that the result did not show statistical difference. As there were no significant differences in the change in intracuff pressure between the two groups, the incidence of mucosal damage-related PIAS might have also shown similar results. However, as other factors affecting PIASs, such as use of oropharyngeal airway or application of cricoid pressure during intubation,3,16 were not assessed in our study, care should be taken when interpreting the relationship between PIASs and TSC tubes. Therefore, further studies will be needed to determine the effect of tracheal cuff shape on mucosal lesions by fiber optic bronchoscopy.
There were some limitations to the present study of note. First, we initially adjusted the intracuff pressure to 25 cm of H2O as a baseline in all patients to prevent aspiration after CO2 insufflation/Trendelenburg position during RALS. Because our aim was to evaluate the intracuff pressure change during RALS, we applied the same initial intracuff pressure in both groups, even though the advantage of TSC tubes is that a good seal can be obtained with a relatively low initial inflation pressure. Thus, further study will be needed to identify whether an initial intracuff pressure to prevent airflow leakage by applying a minimum occlusive cuff pressure 17 might affect the prevention of an intracuff pressure increase during RALS. Second, we did not use N2O during surgery. N2O can diffuse into the tracheal tube cuff and increase intracuff pressure.2,5,6 A previous in vitro study reported that the use of N2O can increase intracuff pressure to even more than 50 cm of H2O. 6 In our current study, because the use of N2O was expected to excessively increase the intracuff pressure during RALS, we could not use N2O, despite the benefits of TSC tubes over CSC tubes.
In conclusion, the TSC tube has a tendency to decrease intracuff pressure change compared with the CSC tube during RALS. However, neither of them was beneficial in preventing an intraoperative intracuff pressure increase during RALS. Further work-up will be needed to prevent intracuff pressure increase during RALS.
Footnotes
Disclosure Statement
No competing financial interests exist.
J-.G.S. was responsible for study design, data analysis, manuscript preparation, and revision. H.S. was responsible for data collection and writing up of the first draft of the article. J.-y.B. was responsible for data collection and analysis. J.O. and W.-J.C. were responsible for data analysis. G.-S.H. was responsible for study conduct and manuscript revision.