
Abstract
Abstract
Purpose:
Laparoscopic gastric greater curvature plication (LGGCP) is an emerging, alternative form of restrictive weight loss surgery. We present our experiences of LGGCP with the primary focus on surgical techniques and weight loss. In addition, an investigation was performed on the food tolerance of LGGCP patients.
Materials and Methods:
This study was conducted by retrospectively reviewing the prospectively collected data of patients who underwent LGGCP from March 2013 to February 2015.
Results:
Of the 64 patients were eligible for the study, 59 (92.2%) were female. Mean (range) patient age was 34 (21–49) years. Mean ± standard deviation (SD) preoperative body mass index was 31.4 ± 4.3 kg/m2. There were no mortalities or postoperative complications. Immediate postoperative nausea and vomiting occurred in 58 patients (90.6%), mean postoperative hospital stay duration was 2.3 days (range, 1–7 days), and mean percentage excess body mass index losses at 1, 3, 6, 12, and 18 months were 34.7% (n = 64), 50.8% (n = 60), 61.1% (n = 40), 82.1% (n = 19), and 82.9% (n = 12), respectively. Follow-up endoscopy was performed at 12 months postoperatively in 19 patients, and reflux esophagitis of grade LA-M was observed in 16 patients (84.2%), LA-A in 2 patients (10.5%), and LA-B in 1 patient (5.3%). Mean ± SD satisfaction score with current eating and total food tolerance score was 4.27 ± 0.55 and 20.95 ± 4.30, respectively.
Conclusions:
LGGCP is an intervention that may be comparable with sleeve gastrectomy or adjustable gastric banding, especially for Class I or II obesity in an Asian population. Furthermore, quality of eating, as determined using food tolerance scores, was excellent.
Introduction
I
A procedure that is restrictive, such as laparoscopic adjustable gastric banding (LAGB) or laparoscopic sleeve gastrectomy (LSG), acts to reduce oral intake by limiting gastric volume, produces early satiety, and leaves the alimentary tract in continuity, minimizing the risks of surgical and metabolic complications. LAGB has been popular since its introduction in the early 1990s because of the simplicity of the procedure, adjustability, and low operative morbidities. However, not uncommonly, we have witnessed disturbance of food passage and proximal dilatation above the band. Furthermore, infection and migration of the band system remain a chronic problem and a cause of band removal. According to recent worldwide statistics, 1 LSG is being increasingly adopted worldwide, and in line with this increase, the use of gastric banding is decreasing. However, LSG is not without complication, and some of these, such as staple line leak, although rare, result in severe clinical conditions.
Laparoscopic gastric greater curvature plication (LGGCP) is an emerging, alternative form of restrictive weight loss surgery and has the potential to reduce complications associated with LAGB and LSG by creating a small tubular stomach without cutting the stomach or implant use. In this study, we present our experience of LGGCP among an Asian population with a lower mean body mass index (BMI) (<35 kg/m2) than has previously been studied with a primary focus on surgical techniques to facilitate early weight loss and minimize complications. In addition, we investigated the food tolerances of LGGCP patients to determine whether LGGCP is a clinically relevant form of restrictive surgery.
Materials and Methods
All procedures performed in this study were in accordance with the ethical standards of the institutional committee at our institution and with the 1964 Declaration of Helsinki and its later amendments. This clinical study involved a retrospective review of the prospectively collected data of the patients who underwent LGGCP at Gil Medical Center (Gachon University College of Medicine and Science, Incheon, Republic of Korea) from March 2013 to February 2015. The guidelines issued by the Asian Consensus Meeting on Metabolic Surgery (ACMOM 2008, Trivandrum, India) for BMI restriction using bariatric surgery (available at www.acmoms.com/acmom_2008.html) were followed throughout. In addition, we included patients with a range of BMI values from 25 to 30 kg/m2 who were refractory to nonsurgical treatment for obesity (a BMI in this range poses moderate risk to Asians 2 ). LGGCP was offered to patients as alternative surgery to LSG and LAGB according to the patient's preference, unless there was an absolute medical contraindication. Informed consent was obtained from all individual participants included in the study, who were specifically informed that LGGCP included an experimental procedure.
All surgical procedures took place with the patient under general endotracheal anesthesia. Transorally a 36 French bougie was inserted to the midesophagus level by an anesthesiologist before the patient was placed in the reverse Tredelenburg position at 30°. A five-trocar port technique at the upper abdomen was used (one 12-mm trocar was placed on the umbilicus, two 5-mm trocars were placed on both anterior axillary lines 3–4 cm subcostally, and two 12-mm trocars were placed at both midclavicular lines, 5 cm subcostally).
Dissection of the omentum started at the watershed area (where the right and the left gastroepiploic vessels meet) on the greater curvature. Using a Harmonic™ scalpel (Ethicon Endo-Surgery, Inc., Cincinnati, OH), we mobilized the greater omentum away from the greater curvature up to near the gastroesophageal junction. The plain of dissection was kept 1–2 cm away from the stomach to avoid thermal injury and to minimize the vascular congestion after plication. The left side of the crus was carefully prepared with the phrenogastric fat pads, and small vessels around the gastroesophageal junction were preserved as much as possible. In the other direction, dissection was continued down to the pyloric antrum 3–4 cm above the pylorus. The right gastroepiploic artery was preserved.
The esophageal 36 French bougie was then further advanced into the gastric lumen, directing toward the pylorus. Gastric infolding was performed using two layers of nonabsorbable sutures [inner interrupted sutures of 2-0 poly(ethylene terephthalate) Ethibond® (Ethicon Endo-Surgery, Inc.) and outer continuous sutures of 2-0 polypropylene (Prolene®; Ethicon Endo-Surgery, Inc.) or V-Loc™; Covidien, Norwalk, CT)]. The first row of sutures was started 2 cm below the gastroesophageal junction and proceeded until 3–4 cm proximal to the pylorus (usually 8–10 full-thickness nonabsorbable interrupted stitches are necessary to complete the first row) (Figs. 1 and 2).
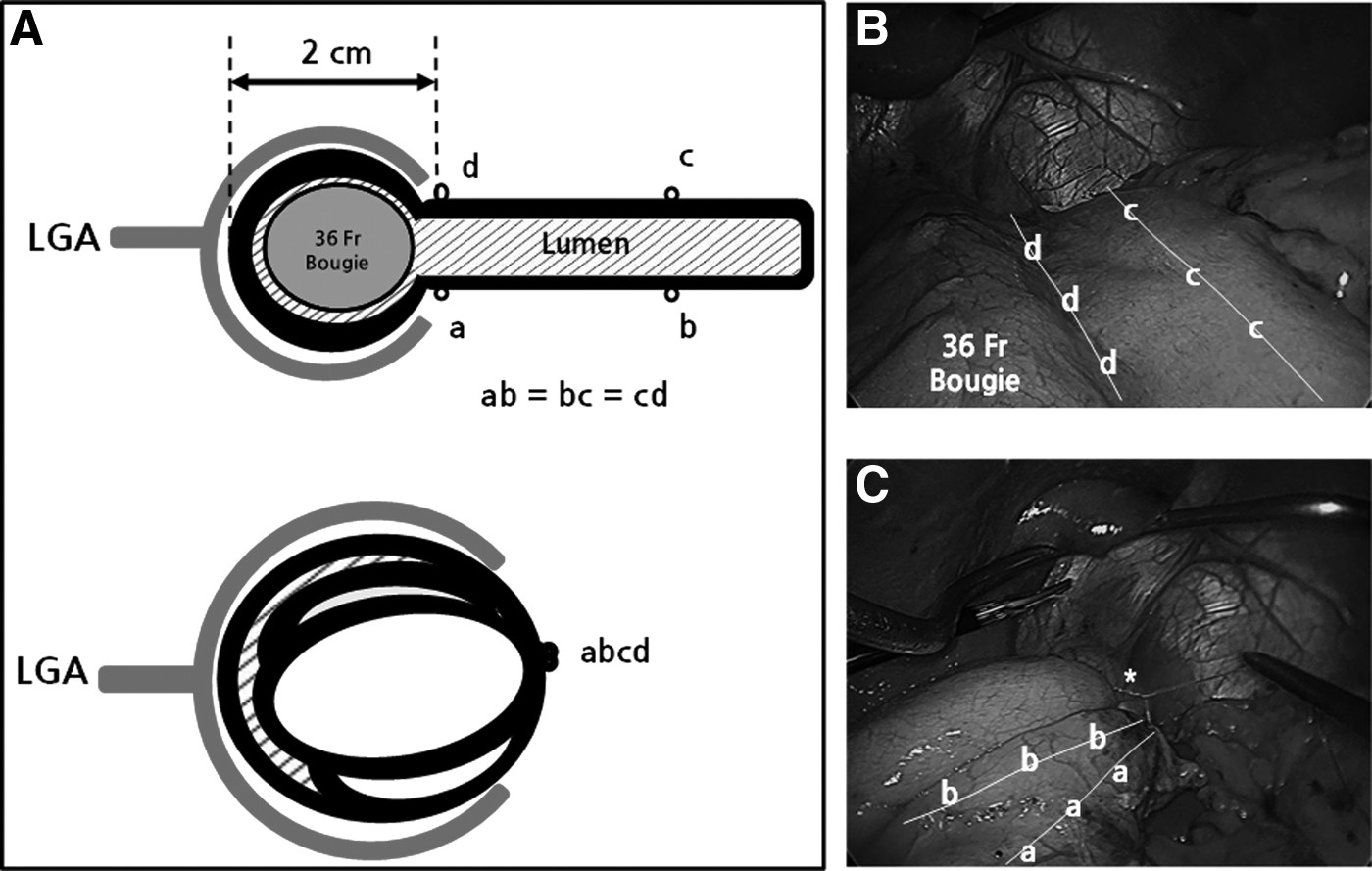
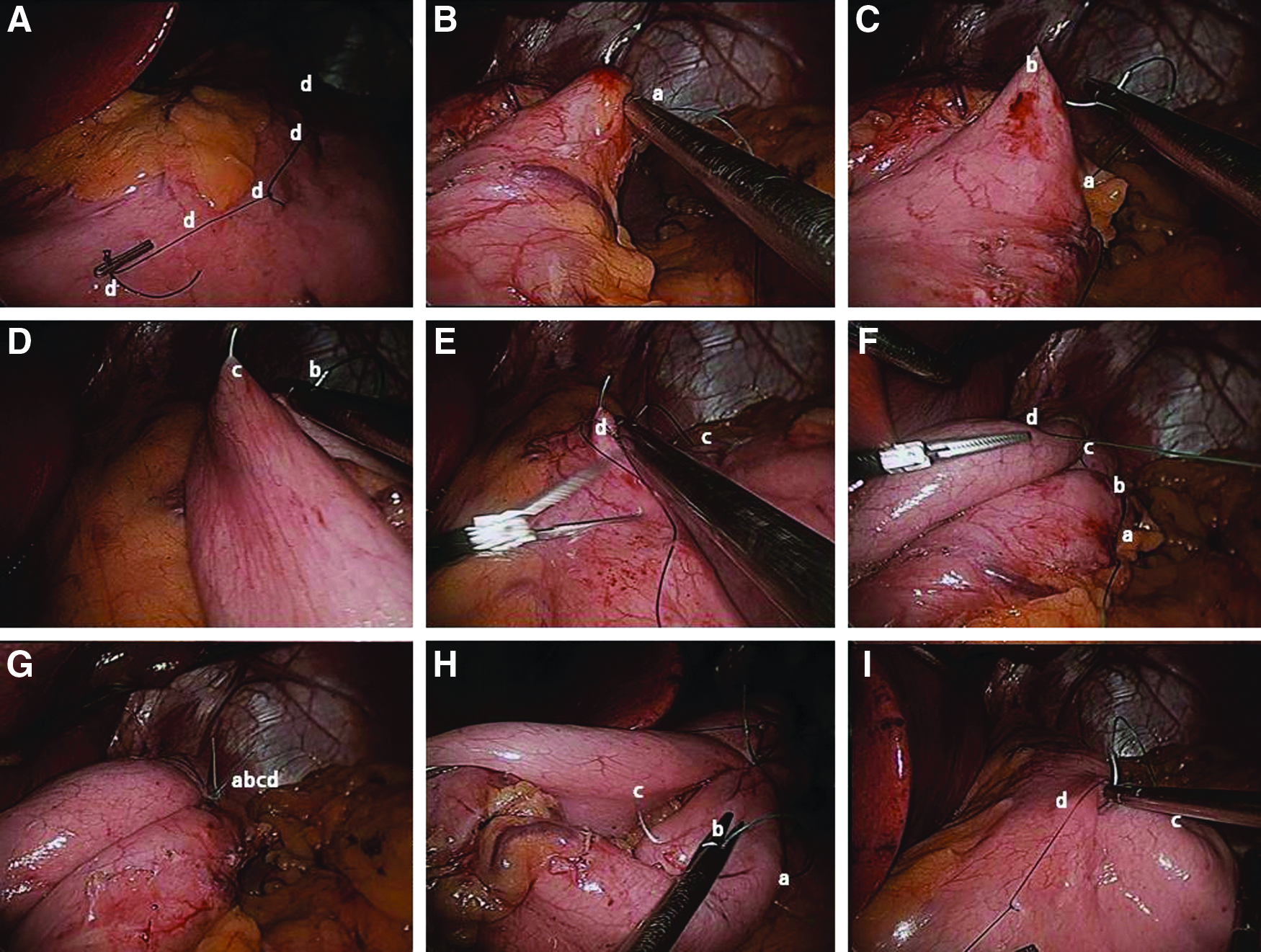
In this technique, our intention was to produce a suture to lesser curvature distance of approximately 2 cm (36 French + gastric wall thickness × 2) as described in the series by Talebpour and Amoli. 3 Distances between the sutures varied from 2 to 3 cm. The second row of sutures was started from the same point as the first row. Extramucosal running 2-0 Prolene or V-Loc was used along the first row of sutures down to 3–4 cm proximal to the pylorus. When the infolded stomach looked insufficiently invaginated after placing the first row, more gastric wall was apposed for the second row (Fig. 3).
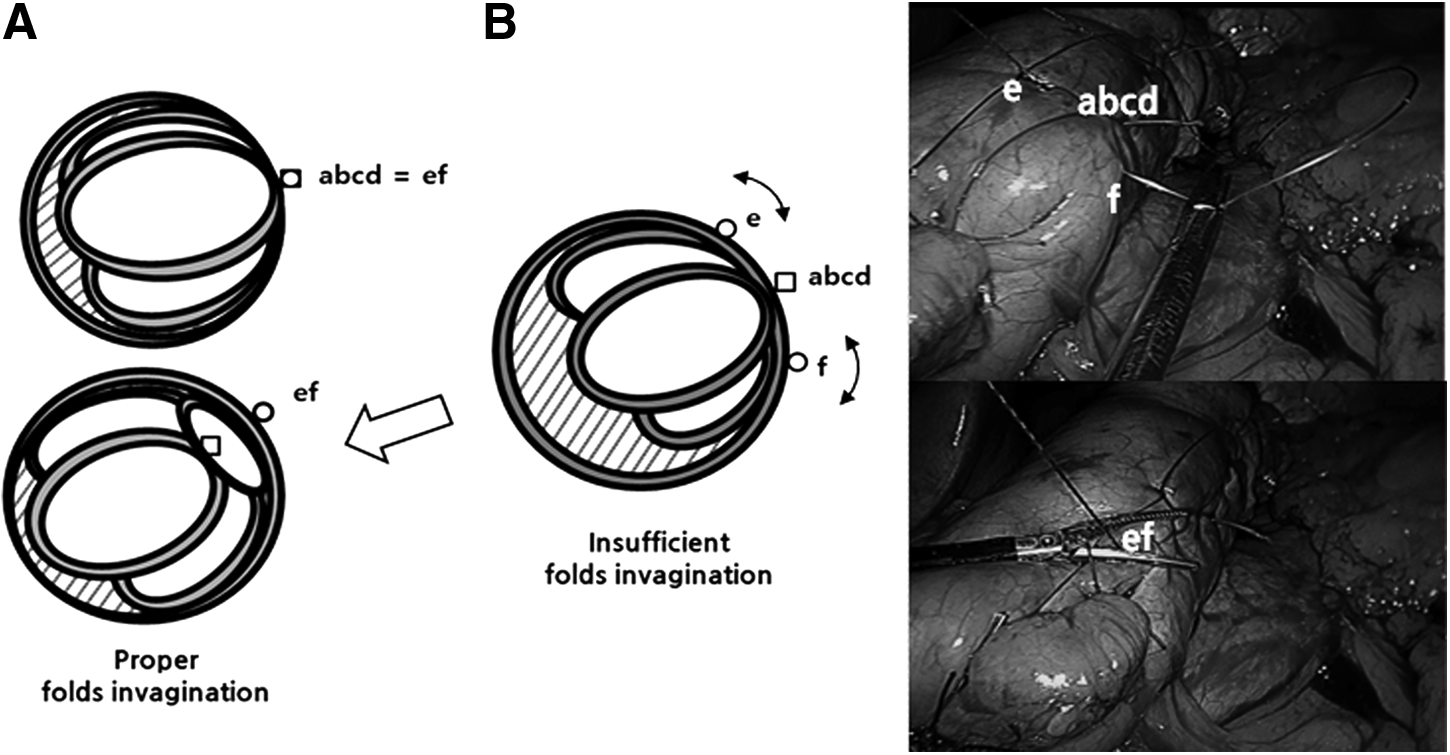
Schematic drawing of reinforcement of the outer layer after the first row of sutures.
After surgery, nil per os was maintained until nausea and sialorrhea subsided. Fowler's position was recommended on the day of surgery. Generous hydration was maintained along with intravenous esomeprazole (Nexium®; AstraZeneca, London, United Kingdom) (40 mg/day), metoclopramide (Macperan®; Donghwa Pharmaceutical Co., Ltd., Seoul, Republic of Korea) (30 mg/day), and granisetron (Kytril®; Roche Pharmaceuticals, Nutley, NJ) (1–2 mg/day). Discharge was considered when a patient tolerated sips of water, and on discharge patients were advised to progress to a soft diet in 15 days and to solid food in 30 days. Oral omeprazole (Losec®; AstraZeneca) (40 mg four times a day or 20 mg twice a day) was prescribed regularly for 3 months. Patients were recommended to visit at 1, 3, 6, 12, 18, and 24 months postoperatively and then annually. Ideal body weight was calculated as the weight corresponding to a BMI of 23 kg/m2 (upper limit of normal BMI for an Asian population). A food tolerance score (FTS) questionnaire was send to patients at least 3 months after LGGCP, and endoscopy was performed regularly at 1 year postoperatively. The FTS is a self-administered, 1-page questionnaire that is used to evaluate degree of food tolerance following bariatric surgery. 4 Endoscopic findings of GER were classified using the modified Los Angeles classification system. 5
Information on patient numbers, operative procedures, genders, ages, perioperative BMIs, percentage excess BMI losses (%EBMILs), and complications were collected during follow-up outpatient visits or by e-mail or telephone. The primary study end point was the effectiveness of LGGCP on percentage excess weight loss, and the secondary end points were early and late complications, FTS, and endoscopic findings.
Results
All operations were performed by a single laparoscopic surgeon (S.M.K.). Sixty-four patients were eligible, and these constituted the study cohort. In these 64 patients, LGGCP was the primary operation, and the operative technique used was as described above. Fifty-nine of the 64 patients (92.2%) were female. Overall mean (range) patient age was 34 (21–49) years, and mean ± standard deviation (SD) preoperative BMI was 31.4 ± 4.3 kg/m2 (range, 25.2–48.0 kg/m2). Comorbidities included type 2 diabetes in 2 (3.1%), hypertension in 6 (9.4%), dyslipidemia in 9 (14.1%), fatty liver in 12 (18.8%), sleep apnea in 3 (4.7%), polycystic ovary syndrome/dysmenorrhea in 3 (4.7%), osteoarthritis in 2 (3.1%), and well-controlled depressive disorder in 12 (18.8%).
All operations were performed laparoscopically, and there were no open conversions. A hiatal defect (<2 cm) was closed concurrently in 6 cases (9.4%). Mean operative time was 136 minutes (range, 75–300 minutes). No morbidity or mortality occurred. Immediate postoperative nausea and vomiting occurred in 58 patients (90.6%). Mean postoperative hospital stay was 2.3 days (range, 1–7 days). One patient (1.6%) required re-admission due to dehydration on postoperative Day 7 and was discharged on postoperative Day 11 after conservative management No major complication requiring re-operation, such as bleeding, gastric obstruction, or gastric perforation/leakage, occurred. All patients showed meaningful weight loss except 1 patient (1.6%); in this patient %EBMIL was less than 30% at 6 months postoperatively. The mean %EBMILs of the patients at 1, 3, 6, 12, and 18 months were 34.7% (n = 64), 50.8% (n = 60), 61.1% (n = 40), 82.1% (n = 19), and 82.9% (n = 12), respectively (Fig. 4).
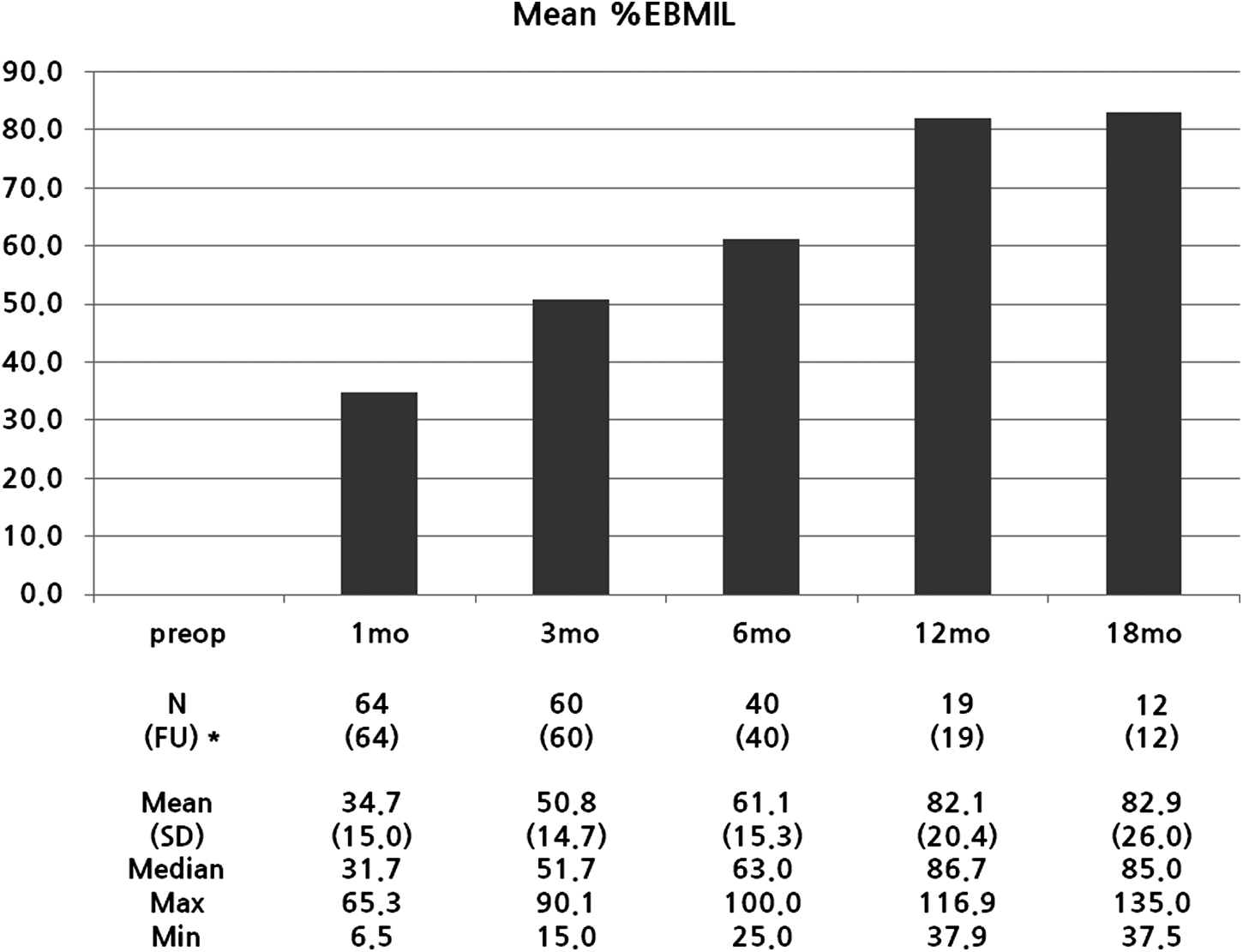
Mean percentage excess body mass index loss (%EBMIL) values at different times after laparoscopic gastric greater curvature plication. *Numbers in parentheses represent number of patients who were followed up (FU) at each time point. Max, maximum; Min, minimum; mo, month; SD, standard deviation.
One-year follow-up endoscopy was performed in 19 patients with reflux esophagitis of LA-M (minimal) in 16 patients (84.2%), LA-A in 2 patients (10.5%), and LA-B in 1 patient (5.3%). All 19 patients showed intact plicated fold without mucosal change on endoscopy (Fig. 5).
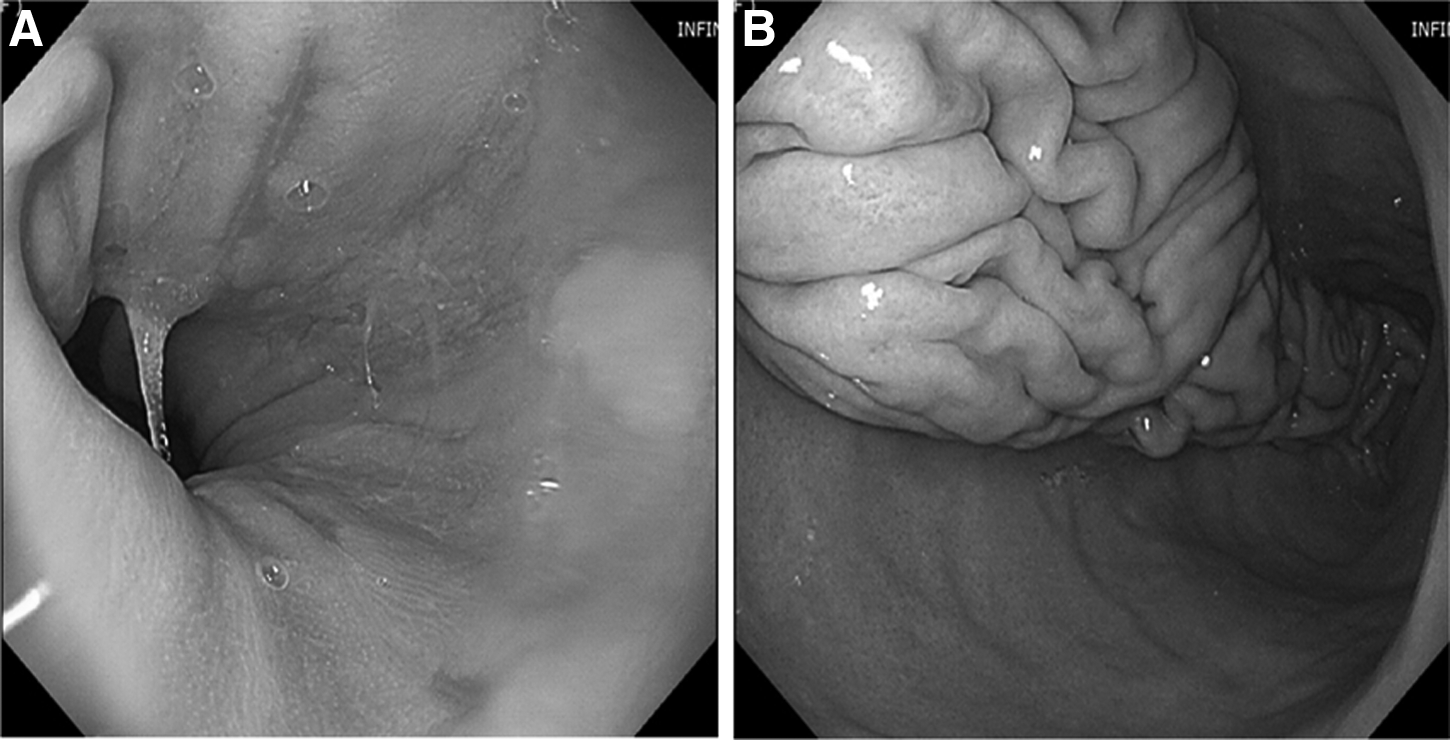
Endoscopic photographs obtained at 12 months after laparoscopic gastric greater curvature plication.
FTS questionnaires were correctly completed and returned by 22 of the 60 patients followed up for 3 months (Fig. 6). Mean satisfaction score with current eating (1–5 points) was 4.27 ± 0.55, and mean specific food tolerance (0–16 points) was 12.95 ± 3.48. Food tolerances for specific food types are summarized in Figure 6. Mean vomiting/regurgitation score (0–6 points) was 3.73 ± 1.12, and mean total FTS (1–27 points) was 20.95 ± 4.30.
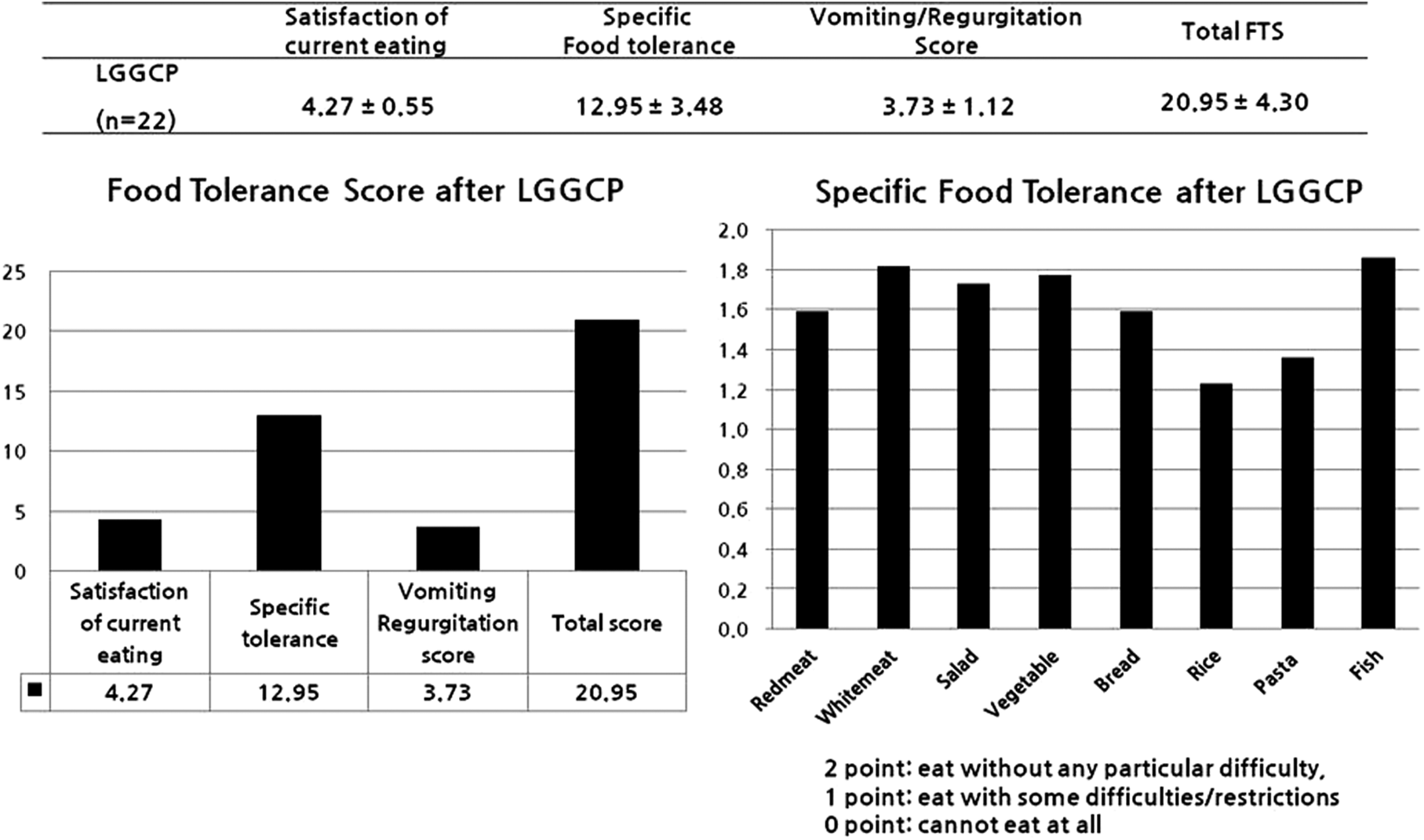
Mean total and specific food tolerance score (FTS) values of the patients (n = 22) after laparoscopic gastric greater curvature plication (LGGCP). Patient satisfaction with current eating was scored between 1 (very poor) and 5 (excellent) points. Food tolerance was awarded between 0 and 16 points (minimum to maximum possible) for eight types of food (2 points if the patient could eat the type without any particular difficulty, 1 point if he or she could eat it with some difficulties/restriction, and 0 points if he or she could not eat it at all). Vomiting and/or regurgitation were given between 0 and 6 points (daily vomiting or regurgitation, 0 points; three or more times a week, 2 points; up to twice a week, 4 points; and never, 6 points). The total FTS therefore varied between 1 and 27 (with 27 being the maximum for excellent food tolerance). Data are mean ± standard deviation values.
Discussion
This study shows that LGGCP is both safe and effective in terms of weight loss and food tolerance. Furthermore, we did not encounter any major LGGCP-specific complication during the clinical observation period up to 18 months. Although several recent studies have reported acceptable short- or mid-term treatment outcomes for LGGCP,3,6–11 almost all patients experience nausea, vomiting, and sialorrhea during the immediate postoperative period. It is suggested that this is due to edema of the apposed gastric wall, 3 which is not only uncomfortable but also increases the incidences of adverse reactions specific to LGGCP, such as focal ischemic perforation,3,9,12 gastric obstruction,3,7,9,11,13 gastrogastric hernia (stitch burst or loosening), 11 and intragastric compartment syndrome. 12 Complications specific to LGGCP probably result from overtightening the gastric lumen, especially at the cardia (displacing the distal esophagus), which often results in “early gastric obstruction” requiring re-operation.
Systemic reviews of LGGCP show that the number of gastric obstruction requiring re-operation has been very similar among different studies and that gastric obstruction is the most common reason for re-operation.14,15 We have found the use of a 36 French bougie, use of the multiple stitch technique (especially at the fundus), and strict diet education (a high protein liquid diet) during the immediate postoperative period are critical for minimizing gastric obstruction. Theoretically, the multiple stitch technique in the inner row of plication decreases the size of pockets created in between the gastric folds that might collect seroma and lead to gastric obstruction.9,16 In our experience, undoing the plication was not necessary in patients with gastric obstruction. Instead, we recommend conservative management because gastric obstruction after LGGCP usually improves as edema subsides. Specifically, Atlas et al. 17 reported 3 of 44 patients required re-operation due to obstruction at the incisura angularis. The gastroscope in those patients passed easily into the duodenum. As is the case during LSG, excessively tight plication should be avoided in this area because the presence of a relative narrowing distal to fundus after tight plication impairs the emptying from the fundus of the stomach, which actually causes development of severe reflux caused by functional obstruction rather than true gastric obstruction. 18 In one report about gastric obstruction after LGGCP, inappropriate oversewing the outer layer of plication actually produced twisting and distortion of the gastric tube. 13 Skrekas et al. 9 reported 3 cases of re-operation for late gastric obstruction. In our surgical technique however, late gastric obstructions were not observed.
Other than too tight plication, gastrogastric herniation between sutures is the cause of gastric obstruction by tensioning the nearby threads. Verdi et al. 19 showed that gastric prolapse was the major cause of revision after LGGCP with one revision (2.2%) for acute prolapse and 15 revisions (33.3%) for later gastric prolapse among 45 patients, although detailed surgical techniques were not described in their series. In our surgical technique, fixation of the entire fundus by multiple plication sutures in the inner row of sutures was critical. In addition, nonabsorbable knotless unidirectional barbed suture material (V-Loc) was best suited for the outer row of sutures because it is not easily loosened during continuous suture reinforcement.
In the present study, the amount of weight loss achieved, as measured by mean %EBMIL, was excellent (>80%) at 12 months postoperatively and was maintained until 18 months postoperatively. However, it is unclear whether these favorable %EBMIL results are attributable to the surgical techniques adopted or to the relatively lower mean BMI of our patients (the average preoperative BMI in this series was 31.4 kg/m2). Nevertheless, these patients are typical of those treated by bariatric surgery for severe obesity in Asia and are classified by the World Health Organization as obese and at high risk. 2 In a similar study on restrictive bariatric surgery, LAGB, performed in patients with BMIs of less than 35 kg/m2, produced mean percentage excess weight loss values at 1 year postoperatively from 52.5 to 78.6 kg/m2. 20 Accordingly, LGGCP presumably is a more relevant restrictive procedure, at least in terms of weight loss. Furthermore, LGGCP offers the added benefits of ease of follow-up, the absence of a silicone foreign body, and freedom from associated long-term complications.
There have been a few studies comparing LGGCP with LSG in the short term showing that LGGCP is inferior as a restrictive procedure for weight loss.19,21,22 It is unclear whether this difference results from the technical variation because LGGCP still lacks standardization of the technique among different surgeons. However, aside from weight loss, LGGCP has the same benefit of treatment of comorbiditites.21,22 The major disadvantages of LSG are the formations of leaks. The other disadvantage of LSG is that altering the anatomy of the cardia results in gastroesophageal reflux in up to 20% of patients. 23 In some patients, initial postoperative edema, luminal narrowing, and acid reflux persist after LGGCP for several months. In such patients, we have witnessed by endoscopy that gastroesophageal reflux is caused by high intraluminal pressure and resulting “transient low esophageal sphincter insufficiency” rather than a damaged antireflux mechanism that has been proposed as a mechanism of gastroesophageal reflux disease after LSG. 24
Actual food tolerance and eating quality after LGGCP have not been described in the literature. In the only study found on the topic, 8 the Impact of Weight on Quality of Life-Lite questionnaire showed a significant improvement at 12 months after LGGCP with a suitable number of patients. The present study is unique in that we investigated eating quality after LGGCP to determine whether LGGCP is a clinically relevant form of restrictive surgery. The mean total FTS score (1–27 points) of LGGCP patients in our study was 20.95 ± 4.30, which is comparable to the published scores of other forms of restrictive surgery.25,26
In conclusion, our initial results of LGGCP are promising, which shows LGGCP is an intervention that may be comparable to other restrictive surgeries in terms of weight reduction and complication. The results were satisfactory, and major complications specific to LGGCP did not happen during the clinical observation period up to 18 months. In addition, quality of eating as measured by FTS was better than that with LAGB. A prospective randomized study with a larger number of patients, as well as longer follow-up to compare other restrictive surgeries, is definitely warranted for LGGCP to be a stand-alone bariatric restrictive procedure. Along with patient education and support, reproducible surgical techniques minimizing both gastric obstruction and too early gastric dilatation should be developed in the near future.
Footnotes
Disclosure Statement
No competing financial interests exist.