
Abstract
Abstract
Background and Aims:
Although the minimally invasive endoscopic Stretta procedure is being increasingly used as an alternative strategy to manage gastroesophageal reflux disease (GERD), the benefits of this procedure have to be further evaluated in clinical settings. This prospective observational study assessed the short-term and midterm outcomes associated with laparoscopic Toupet fundoplication (LTF) and the Stretta procedure.
Patients and Methods:
From January 2011 to January 2012, we allocated 80 patients to LTF and 85 to the Stretta procedure. Primary outcome measures, including symptom scores of heartburn, regurgitation, chest pain, belching, hiccup, cough, and asthma, as well as proton pump inhibitor (PPI) use, were analyzed at midterm follow-up (1–3 years).
Results:
Of the 165 patients, 125 patients following LTF (n=65) or the Stretta procedure (n=60) completed the designated 3-year follow-up and were included in the final analysis. At the end of the 3-year follow-up, the symptom scores were all significantly decreased compared with the corresponding values before the two procedures in both groups (P<.05). After LTF and the Stretta procedure, 47/65 (72.3%) and 41/60 (68.3%) patients, respectively, achieved complete PPI therapy independence (72.3% versus 68.3%, P=.627). Comparing with LTF, however, the Stretta procedure had less effect on improving typical symptoms of heartburn, regurgitation, and chest pain and reducing the rate of re-operation (11.8% versus 0%, P=.006).
Conclusions:
LTF and the Stretta procedure were equally effective in controlling GERD symptoms and reducing PPI use. However, LTF can achieve more improvement on typical symptoms and has a lower rate of re-operation.
Introduction
I
This prospective observational study was therefore conducted to evaluate the short-term and midterm outcomes associated with LTF and the Stretta procedure in selected adult patients with PPI-refractory GERD.
Patients and Methods
Ethical statement
This prospective observational study was approved by the Institutional Review Board and conducted in compliance with the ethical principles for medical research involving human subjects stated in the World Medical Association Declaration of Helsinki. Informed consent was obtained from all subjects.
Subjects
In total, 165 patients with PPI-refractory GERD seeking care in our department were recruited between January 2011 and January 2012. LTF was performed for 80 patients, and 85 patients received the endoscopic Stretta procedure. All participating patients underwent 24-hour ambulatory impedance monitoring, esophageal manometry, upper gastrointestinal contrast radiography, and esophagogastroduodenoscopy preoperatively. The inclusion criteria were as follows: (1) GERD diagnosed by endoscopically evidenced esophagitis, abnormal esophageal pH, DeMeester score of ≥14.7 with symptom correlation of ≥50%, and/or reflux episodes of >73 during a 24-hour ambulatory impedance monitoring; (2) lower than normal esophageal sphincter pressure detected by esophageal manometry; (3) endoscopically confirmed Los Angeles grade A or B esophagitis; (4) nonhiatal hernia or small (<2 cm) hiatal hernia; (5) persistent symptoms despite daily use of PPI; and (6) ≥18 years of age. Patients with central nervous system diseases, connective tissue diseases, previous esophageal or gastric surgery, esophageal stricture, shortened esophagus, impaired distal esophageal peristalsis, Barrett's esophagus, autoimmune diseases, collagen vascular disease, and/or coagulation disorders were excluded.
Treatment
Five-port LTF was performed with the patient under general anesthesia. After the gastrohepatic ligament was dissected with a Harmonic® scalpel (Ethicon Endo-Surgery, Cincinnati, OH), a window was created behind the lower esophagus. Then, the diaphragmatic crura were dissected carefully, and the distal esophagus was mobilized about 5 cm, while the mediastinal structures, including pleura, pericardium, vagus nerves, and aorta, were identified and preserved. In all cases, the gastric fundus was dissected by dividing short gastric vessels. The diaphragmatic crura were sewed behind the esophagus with one or two nonabsorbable sutures, and a posterior 270° 2-cm-long fundoplication was constructed with five or six interrupted nonabsorbable stitches.
Endoscopic Stretta radiofrequency delivery procedure was performed on all patients as previously described. 6 In brief, the patient was sedated, and the distance to the gastroesophageal junction was measured under a gastroscope. Then the endoscope was withdrawn, and a radiofrequency-delivering catheter, consisting of a flexible balloon-basket with four electrode needle sheaths, was introduced orally using a guide wire. The balloon was inflated 2 cm proximal to the squamocolumnar junction, the electrode needles were deployed, and radiofrequency energy was delivered for 1 min. The needles were then withdrawn, the balloon was deflated, and the catheter was rotated 45°. These steps were serially repeated every 0.5 cm inwards, covering an area 2 cm above and 0.5 cm below the squamocolumnar junction.
Outcome assessment
The primary outcome measures of this study were frequency and severity of the major GERD symptoms, including heartburn, regurgitation, chest pain, belching, hiccup, cough, and asthma. Data on these outcome measures were collected through a standardized questionnaire as previously described.4,6,7 More specifically, the frequency was graded as 0 (none), 1 (less than once per week), 2 (once or twice per week), 3 (three or four times per week), 4 (five or six times per week), and 5 (more than six times per week); the severity was graded as 0 (none), 1 (slight), 2 (mild), 3 (moderate), 4 (severe), and 5 (extremely severe). The total of the frequency score and the severity score for each of these measures was designated as the symptom score. Other outcome measures were medication independence and related complications.
The questionnaires were prepared in simplified Chinese and administered to the subjects before LTF or the Stretta procedure and at 1 year and 3 years posttreatment, respectively.
Statistical analysis
Data were expressed as mean±standard deviation values unless specified otherwise. They were analyzed by Student's t tests or nonparametric tests based on their nature. The statistical analysis software SPSS version 17.0 (SPSS Inc., Chicago, IL) was used for all analyses. Differences were considered significant when P<.05.
Results
Initially, 165 patients entered the study. During the designed 3-year follow-up, 31 patients dropped out of the study. In patients with the Stretta procedure, 9 patients were excluded in the final symptom score analysis because of revised therapy during the 3-year period. As a result, 125 (75.8%) patients had complete follow-up. Of these patients, 65/80 (81.3%) patients with LTF and 60/85 (70.6%) with the Stretta procedure were included in the final analysis. There was no significant difference either in the average age (48.6±12.2 versus 47.4±10.7 years, P=.561) or in the male to female ratio (35/65 versus 25/60, P=.173) between patients in the LTF and Stretta groups. The baseline of each symptom score is shown in Table 1. With regard to the baseline, symptoms significantly improved after treatment in patients either following LTF or the Stretta procedure (Figs. 1 and 2).
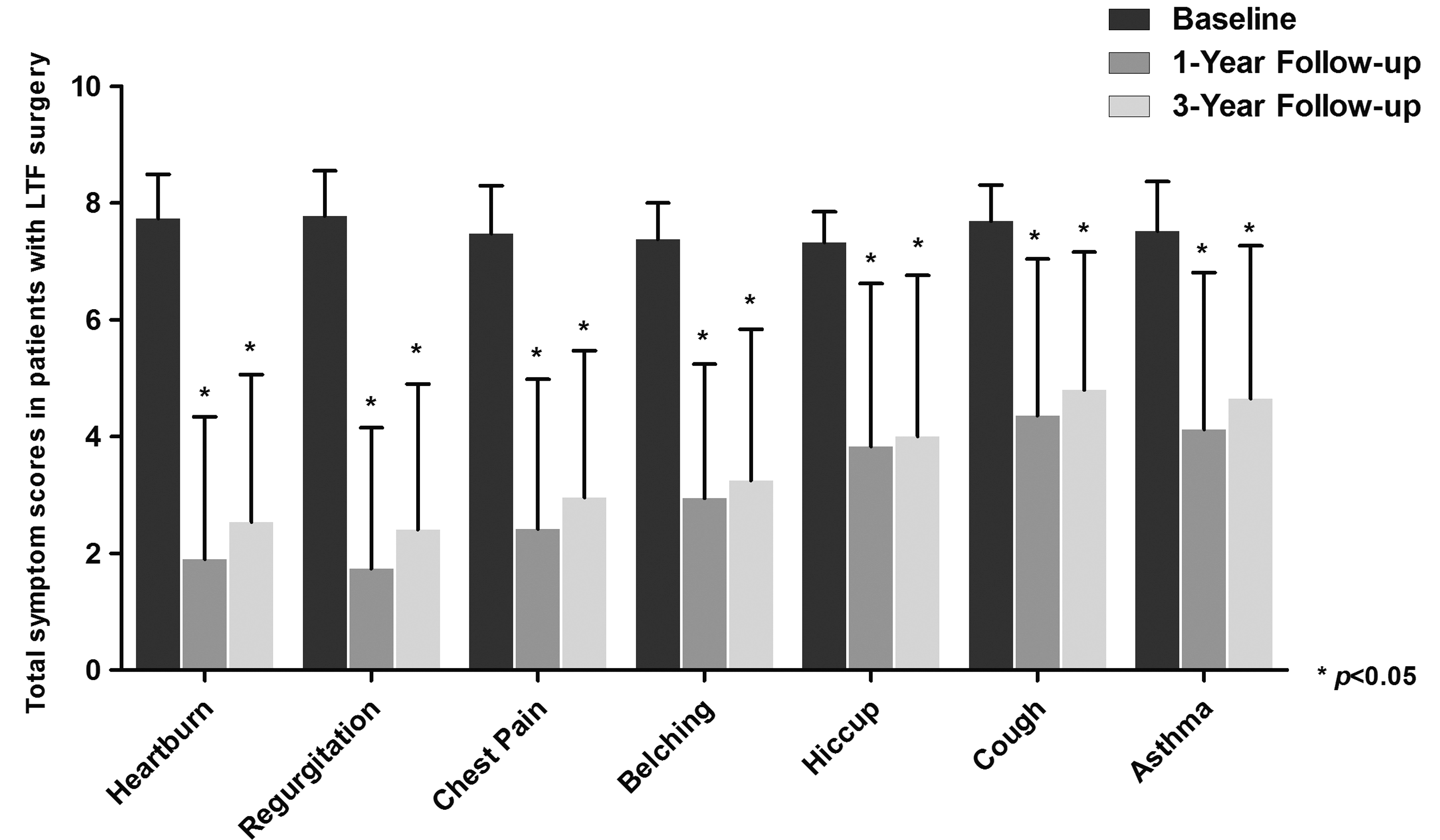
Total symptom scores (frequency score+severity score) in patients before laparoscopic Toupet fundoplication (LTF) and at the 1-year and 3-year follow-up visits.
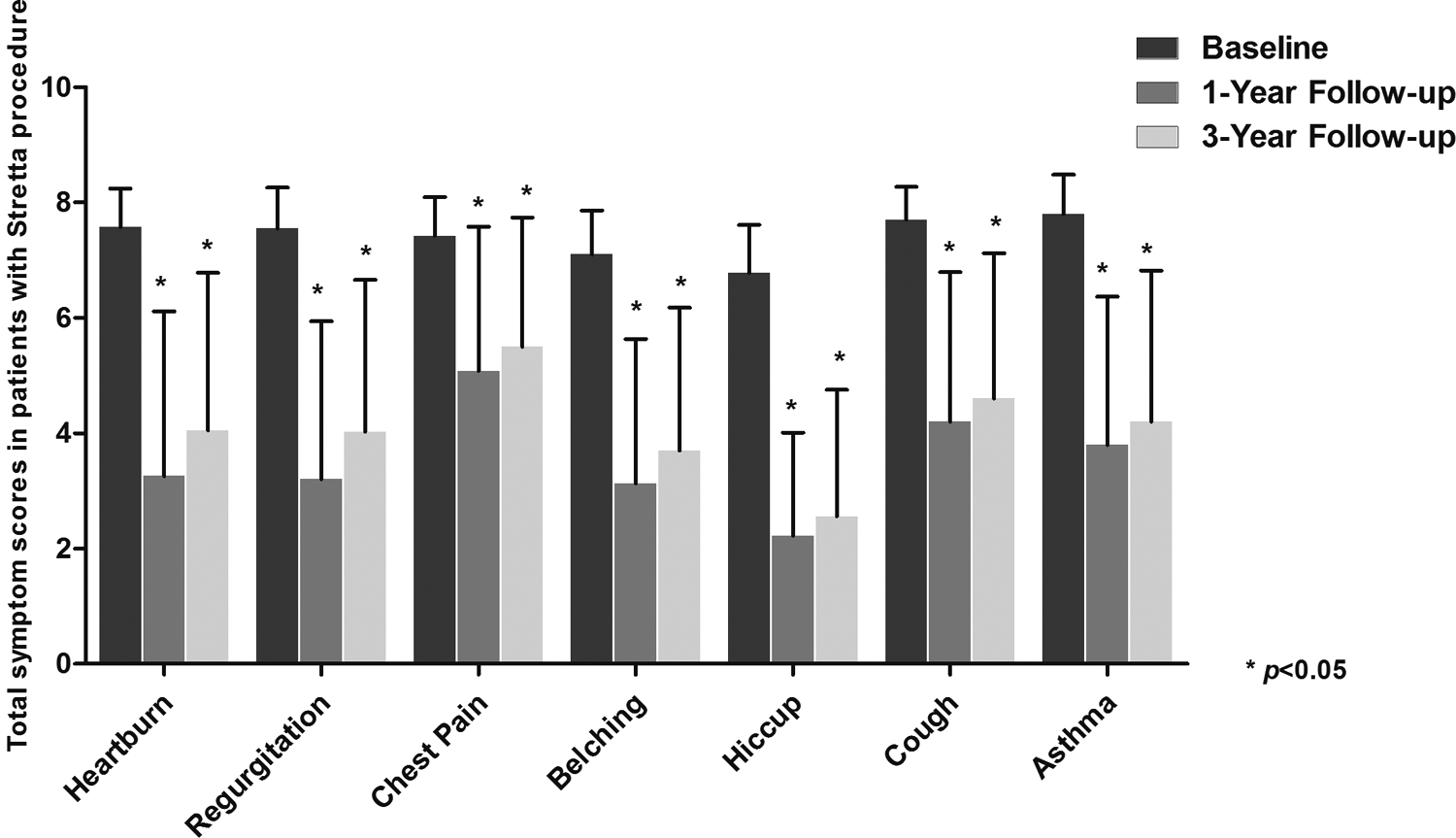
Total symptom scores (frequency score+severity score) in patients before the Stretta procedure and at the 1-year and 3-year follow-up visits.
Data are mean±standard deviation values or n (%) as indicated.
The total of the frequency score and the severity score for each symptom was designated as the symptom score.
LTF, laparoscopic Toupet fundoplication.
Early outcomes
Although the pretreatment symptom scores did not show any difference between patients in the LTF and Stretta groups, LTF showed a clear benefit for improving typical symptoms, including heartburn, regurgitation, and chest pain. In the results of 1-year follow-up, the atypical symptoms, including belching, hiccup, cough, and asthma, significantly improved in both groups, but the improvement was not significantly different between patients in the LTF and Stretta groups (Table 2).
Data are mean±standard deviation values or n (%) as indicated.
The total of the frequency score and the severity score for each symptom was designated as the symptom score.
Significant difference.
LTF, laparoscopic Toupet fundoplication; PPI, proton pump inhibitor.
In addition, patients who had LTF surgery did not have significant benefits on the PPI independence and related complications. Even if the excluded 9 patients were included and considering the rate of re-operation, the LTF surgery would not have any clear benefits at the end of the 1-year follow-up (Table 2).
Midterm outcomes
During the follow-up period, the total symptom scores were significantly reduced, and the reduction was sustained for 3 years in both groups, although each of the symptom scores increased gradually over time. Regarding symptomatic improvements, however, the clear benefits of LTF surgery limited on typical symptoms were sustained (Table 2).
With regard to the PPI independence, 88 (70.4%) of the 125 patients were completely off PPI at 3 years after treatment. Of these patients, 47 (72.3%) of the 65 patients following LTF and 41 (68.3%) of the 60 patients who underwent the Stretta procedure were completely off PPI. However, there was no significant difference in PPI independence between patients in the LTF and Stretta groups at the end of the 3-year follow-up. Although there were no adverse clinical consequences of bleeding episodes, perforations, conversions to open procedure, or deaths in either group, 6.2% of patients complained of surgery-related abdominal distension following LTF. Furthermore, 8 patients who were excluded from the final symptom score analysis needed revision surgery in the Stretta group, and this rate was obviously higher than that in the LTF group at the end of the 3-year follow-up (Table 2).
Discussion
Affecting one-third of the world's population, GERD is the most common chronic digestive disorder. 7 LTF, with the benefit of reducing postoperative dysphagia, has become widely used in the surgical treatment for GERD. 8 Laparoscopic fundoplication has a high rate of patient satisfaction, with a short hospital stay and rapid recovery, but it fails to fall into the “ideal” treatment category because of the high risk of postoperative complications.2,9 Recently, the minimally invasive Stretta procedure has become an acceptable option for patients who are PPI-refractory and poor surgical candidates but still require intensive treatment to adequately manage their GERD.4,6 Nevertheless, the short-term and midterm benefits associated with LTF and this minimally invasive procedure need to be further evaluated.
In this prospective study, we followed up 125 adult patients for 3 years after either LTF or the Stretta procedure. Our results clearly demonstrate that both procedures were effective for reducing the frequency and severity of GERD-associated symptoms, including typical and atypical symptoms. Moreover, the medication elimination rate increased to 72.3% and 68.3%, respectively. In this study, however, the results were different from those of our previous studies.2,4,6,7 It has been demonstrated that the Stretta procedure was less effective in eliminating PPI usage in patients with respiratory symptoms than in patients without respiratory symptoms. 4 Furthermore, the fact that there were fewer patients with respiratory symptoms in this study could be one of the reasons for the higher rate of medication elimination after the Stretta procedure.
This is the first study to compare the outcomes of LTF and the Stretta procedure, although the comparison of laparoscopic Nissen fundoplication and the Stretta procedure had been studied by our team. 7 The midterm results from this study showed that LTF was superior to the Stretta procedure in improving the typical symptoms as opposed to the atypical symptoms. This may be associated with technical differences in laparoscopic fundoplication and the Stretta procedure.3,4 A previous study showed that Toupet fundoplication could achieve the sufficient long-term control of reflux and with a success rate of 85%, 10 but it might have a smaller effect on GERD-related respiratory symptoms. 11 Although numerous studies have evaluated the efficacy of the Stretta procedure in the management of medication-refractory GERD,3,12–16 no studies have demonstrated that the Stretta procedure could be superior to laparoscopic fundoplication. Despite the lack of significant differences regarding atypical symptomatic improvements and medication elimination, more randomized trials are needed to assess the long-term outcomes associated with LTF and the Stretta procedure.
Although the patients who received revision surgeries after the Stretta procedure were excluded from the final analysis, the rate of re-operation should be taken into consideration. In this study, the rate of re-operation after the Stretta procedure was 1.4% during the 1-year follow-up, but this increased to 11.8% at the end of the 3-year follow-up. In these re-operated patients, most would rather have undergone LTF than the Stretta procedure again. Despite the other benefits, the wider application of the Stretta procedure would be limited by its higher rate of re-operation.
Conclusions
In summary, through a 3-year prospective observation, we demonstrated that LTF and the Stretta procedure were equally effective in controlling GERD symptoms and reducing PPI use. However, LTF can achieve more improvements in typical symptoms and has a lower rate of re-operation.
Footnotes
Disclosure Statement
No competing financial interests exist.