
Abstract
Abstract
Objective:
Obturator nerve injury (ONI) is a rare complication during pelvic lymph node dissection (PLND), in extraperitoneal laparoscopic radical prostatectomy (e-LRP), and/or extraperitoneal robotic-assisted laparoscopic radical prostatectomy (e-RALP). It is important to recognize ONI during the initial operation, maximizing the feasibility of simultaneous repair. Here we report our experience with ONI during e-LRP/e-RALP procedures and draw an injury risk map.
Materials and Methods:
Between December 1999 and November 2014, 2531 e-LRPs and 1027 e-RALPs were performed. Five patients (3 during e-LRP, 2 during e-RALP) experienced ONI in the proximal part of the nerve. Obturator nerves were clipped during the 3 e-LRP cases. Clips were immediately removed, and patients received physiotherapy with medical treatments in the postoperative period. During e-RALP, two obturator nerves were transected and subsequently repaired using the robotic Da Vinci® Surgical System (Intuitive Surgical, Inc., Sunnyvale, CA). ONI types were investigated in detail in these patients, and current published studies were analyzed in order to draw a risk map.
Results:
Mean follow-up was 18.8 ± 2.7 months. In total, 3558 cases (2531 e-LRPs, 1027 e-RALPs) were performed. ONI occurred in 3 e-LRP (0.1%) and 2 e-RALP (0.1%) patients. Simultaneous repair was performed successfully in all cases, as clips were removed in e-LRP cases and obturator nerves were repaired using 6/0 polypropylene (Prolene®; Ethicon, Somerville, NJ) suture in e-RALP cases. There was no complication associated with obturator nerve functions such as adductor function and/or neurologic deficiency during long-term follow-up. In view of published studies in the literature, the proximal part of the obturator nerve is at highest risk for injury during PLND, representing 77.8% of reported cases of ONI.
Conclusions:
According to our ONI risk map, the proximal part of the obturator nerve is at higher risk for injury during PLND. Careful dissection and a good knowledge of pelvic anatomy are essential for preventing ONI. Successful ONI management can be performed simultaneously in experienced hands.
Introduction
O
The obturator nerve originates from the second, third, and fourth lumbar nerves. It passes through the pelvis and leaves it by passing through the obturator foramen with the obturator artery and vein. It provides motor innervation to high adductor muscles and gets sensory innervation from skin. 4
ONI can occur by stretching, using severe electrofulguration around the nerve, transection, and entrapment with clips during pelvic lymph node dissection (PLND). According to our best knowledge, there are a handful of cases of ONI during PLND section of extraperitoneal laparoscopic RP (e-LRP) in the published literature. 5 ONI during extraperitoneal robotic-assisted laparoscopic RP (e-RALP) has not been published as yet.
The aim of the present study is to report the incidence and mechanism of ONI during e-LRP and e-RALP. As well, in view of these, we would like to draw a risk map for ONI, considering the location of injury. To our knowledge, this is the first such published report of a risk map for ONI from a pioneer center.
Materials and Methods
This was a retrospective evaluation of prospective recorded data. All patients were informed about the possible complications of the procedures, and signed consent forms were obtained. The certificated prostate cancer (PCa) center of our institute approved the study. All data were recorded on Microsoft (Redmond, WA) Excel™ spreadsheets. Exclusion criteria were irregular follow-up, any metabolic, peripheral, and/or central neurological diseases that can affect peripheral nerves, previous cancer, and previous chemoradiotherapy.
Patients
We collected all data for e-LRP and e-RALP at our institute between December 1999 and November 2014. In total, there were 3558 (2531 e-LRP and 1027 e-RALP) cases. Demographic data of patients, including age, body mass index, prostate-specific antigen, comorbidities, previous operations, preoperative Gleason score, clinical stage, operation time, operation procedure, estimated blood loss, intraoperative complications (i.e., ONI), hospital stay, and postoperative complications, were recorded. Postoperative complications were evaluated according to Clavien–Dindo classifications. 6 Health-related quality of life (HR-QoL) assessment (the 36-item Short Form) was done during follow-up. 7
Operations and techniques
The first step of the e-RALP procedure, including PLND, was started by using traditional e-LRP, until docking the Da Vinci® (Intuitive Surgical, Inc., Sunnyvale, CA) four-arm robotic system, at our department. 8 Additionally, we described our surgical technique for e-RALP and e-LRP elsewhere in detail. 9 In brief, after the patient was positioned for general anesthesia, the extraperitoneal space was created by balloon trocar, and a 12-mm optic trocar was placed according to the Hasson technique through a subumbilical incision. Other trocars were placed as described according to e-LRP or e-RALP. 9 We used 8-mm trocars (Intuitive Surgical, Inc.) instead of 10-mm trocars in e-RALP cases. Indications for PLND were those according to the European Association of Urology Guidelines on PCa. 10
We determined that 5 patients suffered ONI during PLND: 3 cases during e-LRP and 2 cases during e-RALP. The 3 cases during e-LRP experienced inadvertent clip placement on the obturator nerve. The 2 cases during e-RALP experienced ONI as the obturator nerve was transected (Fig. 1). All injuries were in the proximal part of the obturator nerve, where the nerve was running close to the proximal part of the external iliac vein. Clips were removed by endoscopic dissectors during e-LRP. The transected obturator nerve edges were repaired by using 6/0 polypropylene (Prolene®; Ethicon, Somerville, NJ) suture and two needle holders (EndoWrist®) of the Da Vinci robotic system, simultaneously. These were performed by the tension-free reattachment technique. Careful dissection and a good knowledge of pelvic anatomy are essential for both preventing ONI and repairing the obturator nerve.

Transected obturator nerve during robotic-assisted laparoscopic radical prostatectomy. *The obturator nerve was transected from its proximal part (white arrow) where it was passing near the obturator vein. **The distal part of the obturator nerve is close to the arteria iliaca externa. ***The obturator nerve passes through the pelvis to the obturator foramen, with the obturator artery. It was successfully repaired simultaneously by using 6/0 Prolene.
As well, e-LRP cases with ONI received physiotherapy, and 1 of the patients was administered a neurotropic drug. One of the cases of e-RALP with ONI was administered a neurotropic drug, and the other one received both neurotropic drug and physiotherapy. Neurotropic drugs were given under the supervision of the neurology unit of our institute. Physiotherapy sessions were performed at our institute's physiotherapy unit. All patients were given multidisciplinary treatment with the involvement of neurologists and physiotherapists as described above.
Results
Mean follow-up was 18.8 ± 2.7 months. In total, operations were performed on 3558 patients (2531 e-LRPs, 1027 e-RALPs). Five ONI occurred: 3 e-LRP (0.1%) and 2 e-RALP (0.1%) patients. In all patients, ONI was identified and managed successfully during the operation without need for open conversion.
Follow-up of patients
In brief, e-LRP was performed on the first, second, and third patients (Table 1). The chief complaints of the first and second patients were pain in the left leg, which occurred when ONI was caused by placing a clip on the obturator nerve. The first patient described difficulties when he was walking for 3 months. Additionally, both of them received physiotherapy for 10 months. After the treatment period, they considered these problems were affecting their daily life, shown as a 1 point decrease in HR-QoL score. The third patient was also suffering from transient numbness and tingling at his leg, which caused difficulties when he was walking for 2 months. He received physiotherapy for 5 months and medical treatments as neurotropic factors (vitamin B6) for 2 months. 11 He stated that these problems were affecting his daily life, shown as a 2 point decrease in HR-QoL score after the treatment period.
BMI, body mass index; e-LRP, extraperitoneal laparoscopic radical prostatectomy; e-RALP, extraperitoneal robotic-assisted laparoscopic radical prostatectomy; ONI, obturator nerve injury; PSA, prostate-specific antigen; PLND, pelvic lymph node dissection.
The fourth and fifth patients underwent e-RALP (Table 1). The fourth patient was just suffering from difficulties in his left leg while he was walking for 9–12 months. Additionally, he stated that he was feeling abnormal leg movements during walking. Neurologic examinations showed missing reflex of the left adductor muscle, and electromyography of the adductor muscle demonstrated polyphasic action potentials, which was a sign of reinnervation sensitivity. He also received oral vitamin B6 for 2 months. 11 In the light of these, he considered these problems were affecting his daily life, shown as a 1 point decrease in HR-QoL score after treatments. The chief complaints of the fifth patient were pain and hypoesthesia over the medial thigh, on the right side. There were also transient numbness and tingling at his right leg. He had abnormal leg movements during walking. He felt leg weakness at the injury site and had difficulties climbing stairs. The patient received physiotherapy for 5 months and oral vitamin B6 for 2 months. 11 He revealed that these problems were affecting his daily life, shown as a 7 point decrease in HR-QoL score.
Nevertheless, none of the patients had permanent defects in functions of the obturator nerve at long-term follow-up. The patients' characteristics, outcomes, and follow-up periods are presented in Table 1. None of the ONI patients needed additional interventional therapy during follow-up.
Discussion
Early diagnostic tools have been recently used for detection of PCa in developed countries. 10 The incidence of PCa has been decreasing in the United States, and PCa is now the second common cancer among men. 12 Surgical treatment options have been the primary treatment for PCa. Parallel to developed technology in minimally invasive surgery, RP has been performed by laparoscopic and specifically robotic-assisted laparoscopic surgical fashion. The extended PLND is associated with a higher rate of detection of lymph node metastases during e-LRP/e-RALP in patients with clinically localized PCa. However, there are well-known benefits of minimal invasive surgeries, but complications may still be annoying. ONI is a rare complication during RP. It may occur due to stretch (neuropraxia), usage of cautery near the obturator nerve, cutting, and placing a clip on the obturator nerve during PLND section of the e-LRP and/or e-RALP. The reported incidence of ONI in the published literature differs between 0.2% and 5.7% and is summarized, including the present series, in Table 2.
e-LRP, extraperitoneal laparoscopic radical prostatectomy; e-RALP, extraperitoneal robotic-assisted laparoscopic radical prostatectomy; LIHR, laparoscopic inguinal hernia repair; LRP, laparoscopic radical prostatectomy; NA, not assessed; PCa, prostate cancer; PLND, pelvic lymph node dissection; RALP, robotic-assisted laparoscopic radical prostatectomy.
Our series consisted of 2531 e-LRP and 1027 e-RALP patients. In total, 3558 patients were evaluated, and only 5 (0.1%) ONIs occurred. These were successfully managed and repaired simultaneously, as well as detailed information obtained as noted above. However, only 1 patient undergoing e-RALP reported a greater decrease in HR-QoL scores than the others. However, there was no specific feature for this patient. Nonetheless, clinical reflection of ONI was not affecting his daily life in the long term. It was clear that ONI caused some disabilities and decrease in HR-QoL scores in follow-up.
In our opinion, the best way to prevent ONI is having a comprehensive knowledge of the male pelvic anatomy in order to perform an adequate and safe PLND. Additionally, surgeons should be aware of these kinds of injuries, especially during internal PLND in close to the proximal part of the obturator nerve. Of the key importance is that careful dissection and knowledge of pelvic anatomy are the main cornerstones for preventing ONI. Thus, it is also essential not to lose the overview and landmarks such as the external iliac vein or obturator channel during the mentioned surgical procedures. Nezhat et al. 13 reported that this could be a problem specifically in robotic procedures because of the × 10 magnification. The obturator nerve has to be clearly demonstrated in its course before starting with placing clips and/or using cautery around the nerve. Bipolar cautery should be preferred for preventing electrofulguration effects. 14 Monopolar scissors are widely used in robotic surgery. Thus, surgeons should be aware of cautery effects near the obturator nerve. Another issue is to prefer titanium clips instead of Hem-o-lok® (Weck Surgical Instruments, Teleflex Medical, Research Triangle Park, NC) clips, which are wider and difficult to remove and can cause more injury, in case of the nerve becoming entrapped.
The preferred and most effective therapy option in transected case is an immediate repair of ONI by using microsurgical anastomosis techniques.13–24 Nezhat et al. 13 reported a primary suture on the transected left obturator nerve during RALP. Spaliviero et al. 16 recorded full motor function at 21 months after repair for ONI during LRP. However, Rothmund et al. 18 published that there was missing reflex in a patient with ONI at 12 months after nerve repair during PLND. Göçmen and Şanlıkan 23 reported repair for incomplete transection of the obturator nerve during PLND; they also noted successful recovery at 6 months after ONI repair.
We completely agree that immediate repair can help to recover functions of the obturator nerve. Early diagnosis and the patient being awake are the cornerstones of diagnosing ONI. Additionally, surgeons should know how to manage perioperative complications such as ONI. 25 Thus, 2 patients underwent primary repair by using 6/0 Prolene due to transection of the obturator nerve during e-RALP in the present series; these procedures took 9 and 11 minutes, respectively. Improved high-definition vision with × 10 magnification and dexterity in suturing with precise EndoWrist needle holders could facilitate the suturing. These could also optimize the quality of suturing, which is very important in epineural reapproximation of the nerve. There were some disabilities in these patients in the short term, but no permanent disability was recorded in long-term follow-up. The impact of early repair should not be underestimated for ONI.
Physiotherapy and medical treatment options are the other additive treatments of choice after ONI. Stolzenburg et al. 15 reported conservative treatments after ONI. Fishman et al. 14 noted that muscle weakness was still continuing after ONI that was managed by physiotherapy. There were 4 patients who received physiotherapy and 3 patients who received medical treatment with vitamin B6. In light of the data in Table 2, conservative treatment options seemed like the first-line treatment for ONI. Moreover, physiotherapy may help to recover to motor and/or sensory functions. 26 Besides, medical treatments with vitamin B6 can help the reinnervation period for injured nerves. 27 Therefore, electromyography can show improvement in innervation rates of the obturator nerve during follow-up. Multidisciplinary work involving neurologists and physiotherapists should be considered. As a result, conservative treatment options are more suitable for cases without nerve transections than for cases with transected obturator nerve.
Haninec et al. 17 and Rothmund et al. 18 reported ONI on the proximal part of the nerve with 1 case in each series. On the other hand, Nezhat et al. 13 and Rafii and Querleu 20 noted injury on the distal part of the obturator nerve. Finally, there were 5 cases with injury on the proximal part of the obturator nerve in the present series. These are summarized in Table 3.
ONI, obturator nerve injury.
The obturator nerve may be fixed to lymph nodes or surrounded by them. In such cases, a careful nerve mobilization should be performed. Additionally, surgeons should be patient during PLND. Fixed lymph nodes should not be mobilized roughly. Specifically, the proximal part of the obturator nerve is passing close to the external iliac vein and the internal iliac artery where the internal iliac lymph nodes are localized. According to our clinical opinion, retraction of the peritoneum to medial can provide surgeons a better view for operation space in this risky area.
In the published literature, 77.8% of reported injuries occurred in the proximal part, and 22.2% occurred in the distal part, according to our risk map (Fig. 2). No injury has been reported for the middle area.17–20 If we would draw a risk map for ONI, the proximal part of the obturator nerve is at high risk, as can be seen from Table 3.
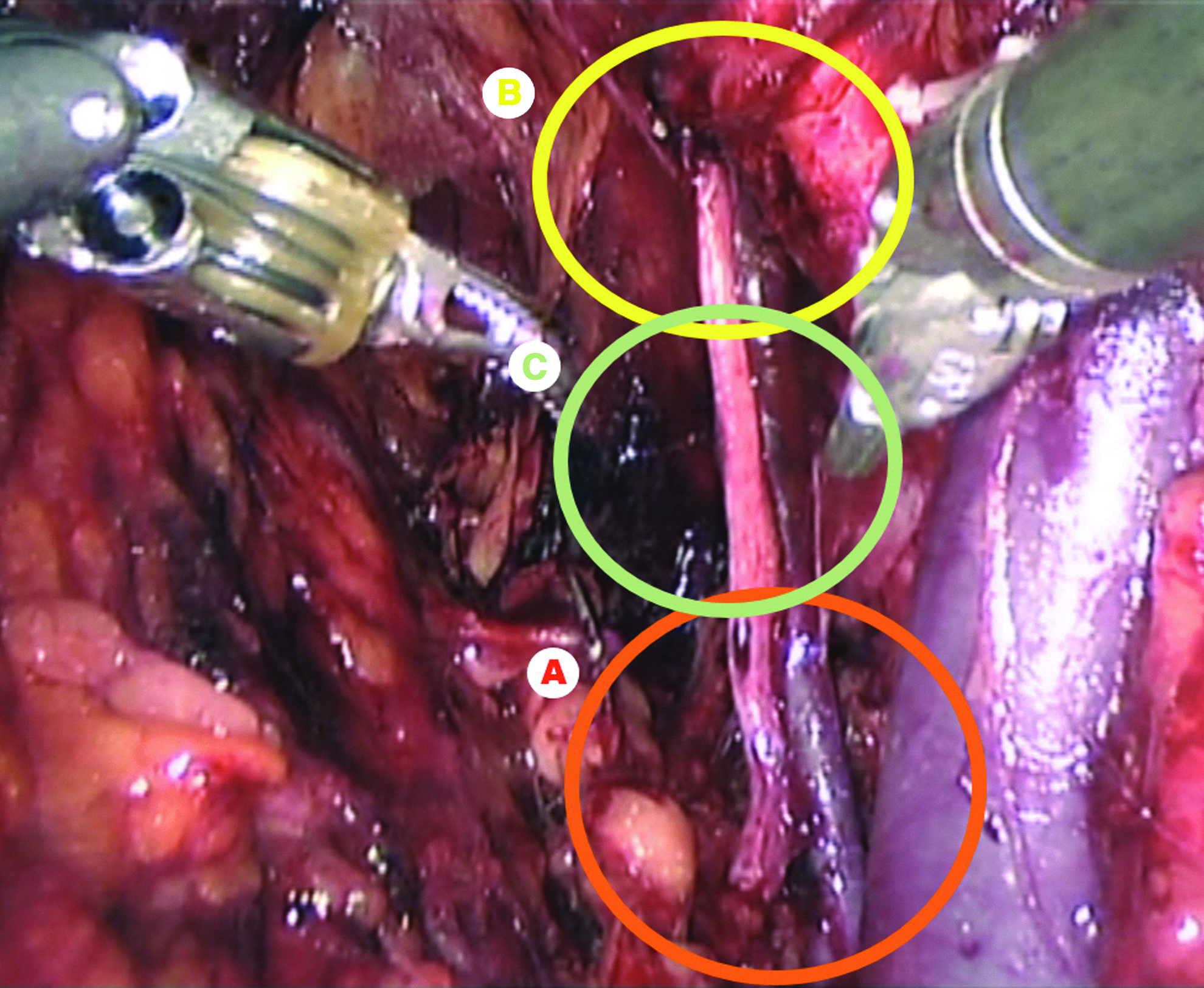
Risky areas (circled) for obturator nerve injury: (A) the proximal part, (B) the distal part, and (C) the middle part of the obturator nerve.
Primarily, it is very important to identify anatomical landmarks to avoid nerve injuries during surgery. The minimally invasive fashion of robotic surgery can help us in terms of magnified vision and a superior high-definition view. Thus, all of these can provide us precise identification and dissection of lymph nodes, the obturator nerve, and vessels in the retroperitoneal pelvic space. 25
Besides, the surgeon's experience and abilities come into question. The prevention of most iatrogenic injuries depends on training in the technique, and the incidence of complications correlates directly with the surgeon's experience. At our training center, surgeons perform various steps of e-LRP under the supervision of an experienced mentor according to their experience level. The third through fifth cases were performed by surgeons who were at the beginning of their learning curve. If an obturator injury occurs during e-LRP, the surgical team should be sufficiently experienced, and the advantages of laparoscopic surgery should not be forfeited by conversion to open surgery. In our series, all complications were managed by the mentor (J.R.) of the center, and there was no clinical reflection of permanent damage in the obturator nerve in long-term follow-up.
We know the limitations of the present series. The retrospective pattern is one of them. On the other hand, the goals of the study included presentation of the greatest numbers of ONI during the laparoscopic PLND section of e-LRP and e-RALP in the published literature. In addition, a risk map was drawn for ONI during PLND. According to these, we strongly believe that the best way to spare the obturator nerve is related to careful dissection specifically on the proximal part of the nerve during PLND.
Conclusions
ONI is a rare complication of PLND section during e-LRP and e-RALP. Careful dissection and a good knowledge of pelvic anatomy are essential for preventing ONI. Surgeons should be particularly careful near the proximal part of the obturator nerve during PLND. It is important to recognize ONI in the course of the surgical procedure. Immediate surgical repair can help the obturator nerve to recover, and conservative treatment options can support treatments after operation. More structured studies on this topic are needed for preventing ONI.
Footnotes
Disclosure Statement
No competing financial interests exist.