
Abstract
Abstract
Background:
Omohyoid muscle syndrome (OMS) (not omohyoid syndrome) is a rare clinical condition that has a characteristic feature of a protruding lateral neck mass during swallowing. The use of endoscopic surgery on the neck is now pretty well established for thyroid and parathyroid glands. Patients with OMS usually undergo simple surgical transection of the omohyoid muscle. The procedure leaves operative scars on the neck, and most patients worry about the cosmetic problems. We report here the first use of an endoscopic procedure instead of traditional surgery for treatment of OMS.
Materials and Methods:
We present a rare case of a 26-year-old Chinese man who noted a protruding mass involving the right side of his neck during the past 10 years. OMS was diagnosed. Laparoscopic simple transection of the omohyoid muscle by an ultrasonically activated scalpel was performed.
Results:
After laparoscopic transection of the omohyoid muscle, the neck mass completely disappeared during swallowing, and there were no operative scars on the neck.
Conclusions:
To our knowledge, this is the first report of laparoscopy for treatment of OMS. We believe that the laparoscopic procedure is made acceptable for this unusual disease because of the cosmetic result.
Introduction
O
Case Report
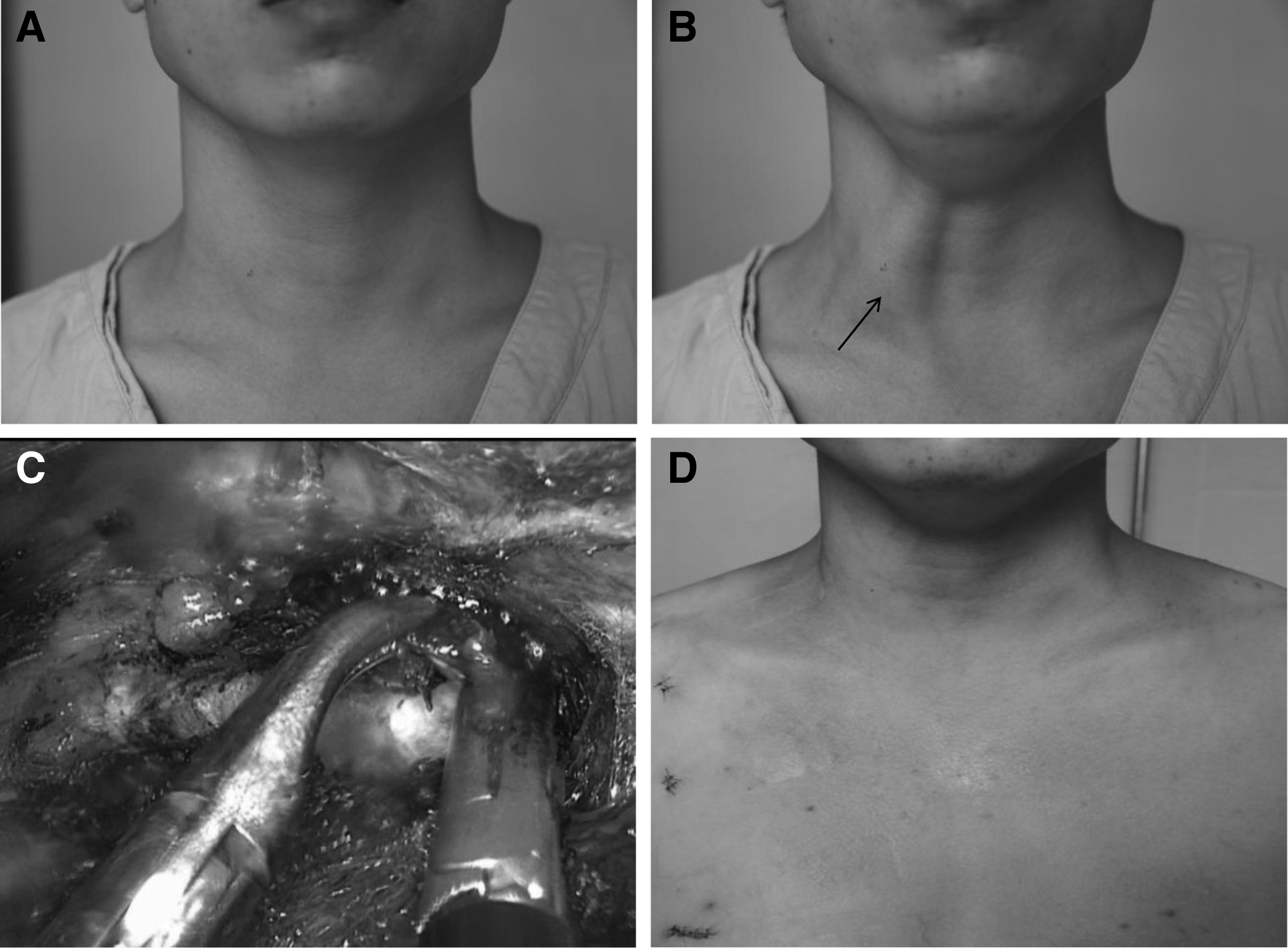
A 26-year-old Chinese man noted a protruding mass involving the right neck during the past 10 years. The mass was present during swallowing and disappeared right after swallowing (Fig. 1A and B, arrow). The mass caused him to be uncomfortable with the disconfiguration. No special symptom was noticed. The routine ultrasound and computed tomography scan of the neck revealed no morphological abnormality. OMS was diagnosed according to the clinical symptoms and signs.
The patient in the
Endoscopic simple transection of the omohyoid muscle was performed with the patient under general anesthesia and with endotracheal intubation similar to the transaxillary approach for endoscopic neck surgery. The patient was placed in the supine position with the neck extended with a shoulder pillow. Diluted (1:500) epinephrine solution was injected into the subcutaneous space in the breast and subplatysmal space in the neck to reduce bleeding during the dissection.
The first incision was made in the upper right areolar areas. Through the opening, subcutaneous and subplatysmal dissections were done bluntly with use of a dissector. After the dissections were done to the desired extent, the 10-mm port was put on the side of the mass, and the laparoscope was introduced through this port. The working space was established with CO2 insufflation at a pressure up to 6 mm Hg. Two 5-mm ports used for the operational instruments were inserted through incisions below the clavicle near axillary areas on the side of the mass. The remaining dissection was completed with the visual guidance of the laparoscope. After the interior border of the sternocleidomastoid muscle was dissected, good exposure of the omohyoid muscle and carotid sheath was achieved. The omohyoid muscle was transected by an ultrasonically activated scalpel (Fig. 1C). Complete hemostasis was attained, and no suction drain was left in place. The skin was reapproximated cosmetically. The operation lasted 0.5 hours.
After endoscopic transection of the omohyoid muscle, the neck mass completely disappeared during swallowing. No complication occurred. The patient's postoperative stay was 1 day. The cosmetic result was considered very good by the patient at 1 day (Fig. 1D) and 6 months after the procedure.
Discussion
OMS, also called omohyoid sling syndrome, is a rare disease. The first description of a patient with OMS was reported in Chinese in the Chinese Journal of Surgery in 1978 by Ye, who also reported in the English literature in 1980. 4 Historically, a similar terminology, omohyoid syndrome, was used in a report published in The Lancet in 1969 to describe a case with characteristic symptoms, including pain and tenderness in the neck, voice changes, and swallowing difficulties most likely due to acute spasm or cramping of the omohyoid muscle. 5 However, the patient did not show any neck mass or anatomical disconfiguration during swallowing. Thus, this case is not compatible with the current concept of OMS.
The key clinical finding of OMS is the pathognomonic feature of the appearance of a transient lower lateral neck mass during swallowing due to dysfunction of the omohyoid muscle. Physical examination characteristically showed no positive finding when the patient was not swallowing. Most patients with OMS were treated by omohyoid muscle surgical transection. The procedure leaves operative scars on the neck. Botulinum toxin injection under ultrasonography guidance for OMS could offer a way to simulate the effect of omohyoid muscle transection without operative scars on the neck, but it does not predict whether OMS will completely recur or if another injection is required. 1
The use of endoscopic surgery on the neck is now pretty well established for thyroid and parathyroid glands. We report here the first use of an endoscopic procedure instead of traditional surgery for treatment of OMS. After the procedure, the neck mass completely disappeared during swallowing, and there were no operative scars on the neck. The cosmetic result is perfect.
In conclusion, we performed endoscopic simple transection of the omohyoid muscle. To our knowledge, this is the first report of an endoscopic procedure for treatment of OMS. We believe that the endoscopic procedure is made acceptable for this unusual disease because of the cosmetic result.
Footnotes
Disclosure Statement
No competing financial interests exist.
All authors had access to the data and a role in writing the manuscript.