
Abstract
Abstract
Background:
Distal obstruction of ventriculoperitoneal (VP) shunts is a major problem in the treatment of hydrocephalus. To avoid this complication, we describe a simple method using the falciform ligament to place and hold the distal catheter in the right subdiaphragmatic space, preventing catheter migration and distal obstruction.
Materials and Methods:
We retrospectively collected data of all VP shunt insertion and revision for adults with idiopathic normal-pressure hydrocephalus between November 2011 and September 2013. All of these were done using the “falciform technique,” with the distal catheter portion performed laparoscopically. No exclusion criteria were applied. A neurosurgeon and a laparoscopic surgeon were involved in each case. The falciform ligament was used to tether the distal catheter above the liver, with the distal tip of the catheter reaching the hepatic flexure to allow for drainage directly into the right paracolic gutter. Baseline, operative, and postoperative data were collected and analyzed.
Results:
In total, 58 patients underwent a shunt procedure during the period of study. The majority (74%) underwent new VP shunt placement, and 26% underwent revision and replacement for catheter obstruction. The female to male ratio was 1.14:1. Mean age was 67.3±17.5 years. Revisions due to distal catheter obstruction were subsequent to previous surgery placement. Median follow-up was 329 days. Three patients (5%) had proximal catheter obstruction requiring shunt revision. None of the patients (0%) was found to have distal obstruction at the end of the study period at the most recent follow-up.
Conclusions:
The faparoscopic falciform technique significantly reduces the rate of distal VP shunt obstruction in adults with idiopathic normal-pressure hydrocephalus. Continued follow-up is needed to confirm long-term patency of the catheter.
Introduction
H
Neurosurgeons traditionally use a mini-laparotomy and blind manual direction for distal catheter placement into the abdominal cavity. 6 Distal catheter failure rates are reported as being between 5% and 35%, with higher rates due to abdominal adhesions, obesity, or scoliosis.6,7 Blind placement of the catheter also carries the risk of postoperative ileus, injury to intraabdominal organs or blood vessels, and inability to confirm the patency of the catheter or its location within the abdominal cavity at the end of the case. Preperitoneal malposition occurs in a significant number of patients. 6 Advances in laparoscopic insertion techniques have not decreased overall shunt failure rates. 8 Laparoscopy allows for confirmation of patency, visualization of placement, lysis of adhesions, removal of foreign bodies, sampling of peritoneal fluid for culture, and minimization of abdominal trauma.9,10 Some neurosurgeons rely on the expertise of a general surgeon for laparoscopic placement of the distal shunt. 11
A technique using the falciform ligament that involved clipping the catheter in place, with drainage onto the liver in the subdiaphragmatic space, was associated with complications of adhesions and distal catheter obstruction, as well as unwanted side effects of hiccups and referred shoulder discomfort. 12
With the goal of preventing distal catheter obstruction in adults with VP shunts, we used a modification to the previously described falciform ligament technique, achieving catheter fixation without the use of clips and placement of the distal catheter tip in an area of the peritoneal cavity with potential space for cerebrospinal fluid drainage and absorption.
Materials and Methods
After obtaining institutional review board approval, we performed a retrospective analysis of the electronic medical records of a consecutive series of adults with hydrocephalus who underwent VP shunt insertion or revision with laparoscopic assistance at Sinai Hospital of Baltimore (Baltimore, MD) by a single general surgeon from November 2011 to September 2013. All adults with hydrocephalus who required VP shunt insertion or revision were eligible for the falciform technique. Data collected included sex, comorbidities including prior abdominal surgery and indication of procedure, operative date, intraoperative complications, and postoperative complications including catheter patency and wound infection during the follow-up period.
Our institution's standard practice is to follow hydrocephalus patients at 3–6-month intervals to determine whether the patient's INPH symptoms are improved, and if not, to arrange for evaluation of shunt obstruction by nuclear medicine shunt patency studies. 5
Operative technique
A neurosurgeon and laparoscopic surgeon were involved in every case. A cranial incision was made, and the proximal shunt catheter was inserted by the neurosurgeon (or tested for revision). At the same time the laparoscopic surgeon accessed the abdominal cavity by using a 5-mm incision just above the umbilicus. A diagnostic laparoscopy was then performed, with lysis of adhesions if necessary. Another 5-mm trocar was placed in the left upper quadrant.
For shunt revision surgery, the previously inserted distal catheter was located and assessed. It was disconnected from the shunt valve and tested for patency using sterile saline and laparoscopic visualization of saline flow. All existing catheters were replaced with new distal catheters regardless of patency due to specific length requirements.
The distal catheter was trimmed to a length of no more than 30 cm within the abdominal cavity and tested for patency under direct vision before insertion into the abdominal cavity.
The neurosurgeon tunneled the new distal catheter to an abdominal incision placed to the left of the falciform ligament in the epigastric area. A 5-mm trocar was used at the epigastric incision to create an entry point into the abdomen, and an introducer sheath was peeled apart after introducing the catheter into the track (Fig. 1). A small defect (about 0.5 cm) was created in the falciform ligament using electrocautery (Fig. 2). The distal catheter was placed through the falciform defect and draped over the dome of the liver in the subdiaphragmatic space so that the distal end of the catheter would reach the hepatic flexure to drain cerebrospinal fluid directly into the right paracolic gutter (Figs. 3–5). The abdomen was then desufflated, and the port sites were closed with subcuticular sutures.
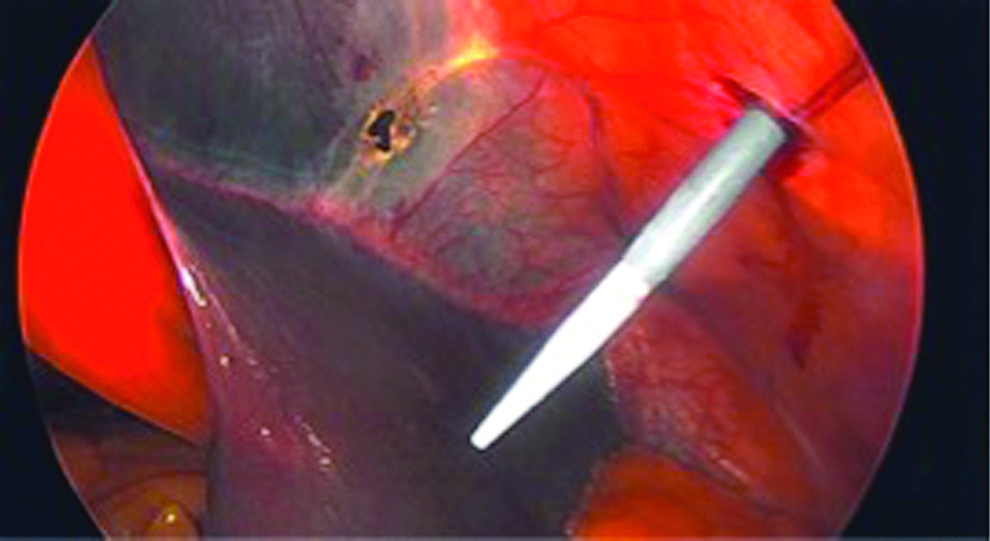
The falciform defect is created, and the distal catheter is inserted through the abdominal wall.
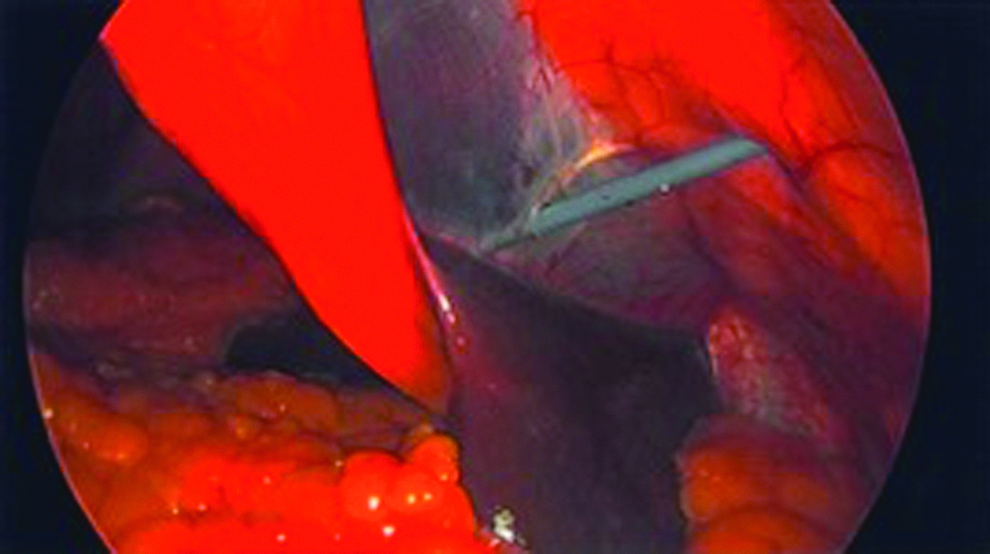
The catheter sheath is directed and inserted through the falciform defect.
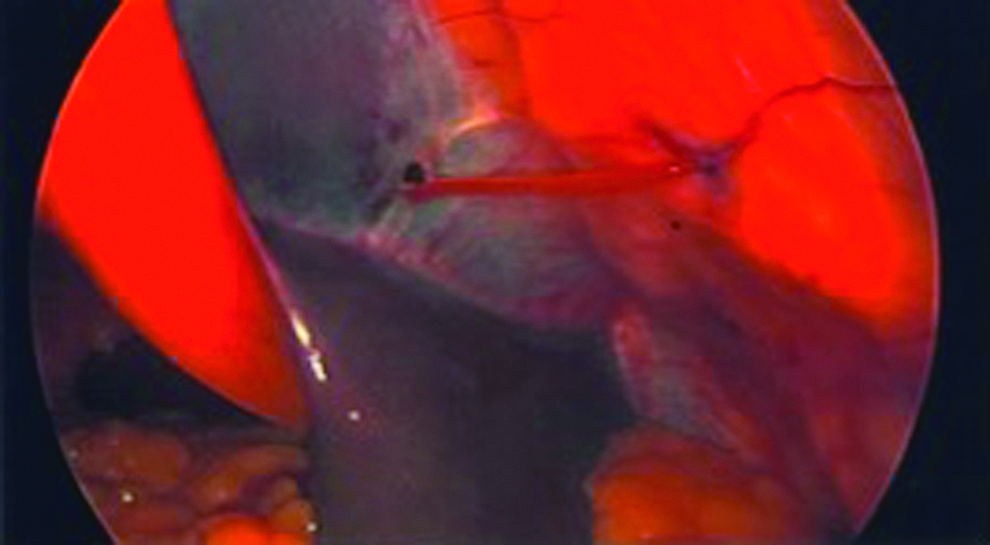
The catheter is inserted through the falciform ligament defect, and the sheath is removed.

The distal catheter is directed toward the right subdiaphragmatic space.
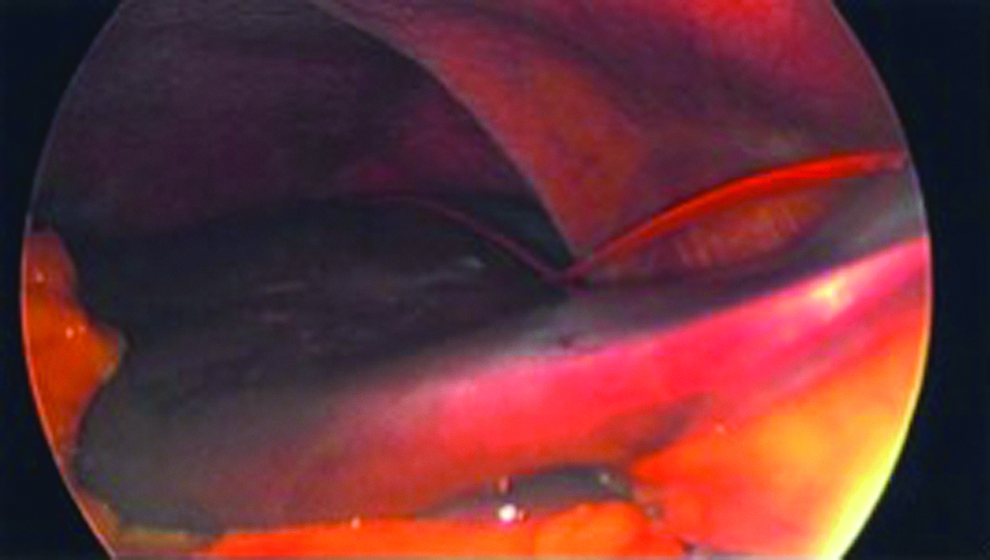
The distal catheter is confirmed to be positioned above the liver with the distal end directed toward the right paracolic gutter.
Postoperative procedure
Postoperative abdominal x-rays were taken for verification of the catheter location initially, but this practice was stopped after the first 28 cases because it did not alter patient care.
Results
Fifty-eight patients underwent either placement or revision of VP shunt using the laparoscopic falciform technique. Forty-three (74%) underwent new VP shunt placement, and 15 (26%) had revision and replacement. The female to male ratio was 1.14:1. Average age was 67.3±17.5 years. Average body mass index was 29.2±7.3 kg/m2 (Table 1). All shunt revisions for distal catheter obstruction were for catheters that had been originally inserted using the mini-laparotomy or laparoscopic technique, but not the falciform ligament technique. There were no intraoperative complications of bowel injury, conversion to open laparotomy, estimated blood loss of >100 mL, or intolerance to pneumoperitoneum.
Median follow-up was 329 days (range, 19–707 days). None of the patients (0%) was found to have distal obstruction during our study period.
Three shunts (5%) were revised for proximal catheter obstruction. One was suspected to be a proximal obstruction based on the shunt patency study that showed no entry of radionuclide into the ventricles. Another was initially thought to be a distal catheter obstruction based on the shunt patency study; however, distal obstruction was discovered at the time of shunt revision surgery. The etiology of the last was uncertain until the time of surgery, as technical difficulties prevented a shunt patency study from being performed.
The first 28 patients (46.7%) underwent routine abdominal x-rays for confirmation of VP shunt placement. Of those, 24 of 28 catheters (85.7%) were in the right upper quadrant as intended, 2 (7.1%) could not be visualized due to the patient's body habitus, 1 (3.6%) was visualized in the left upper quadrant, and 1 (3.6%) was visualized in the right lower quadrant suggesting postoperative displacement.
Discussion
We have demonstrated a remarkably low distal catheter obstruction rate by use of the falciform ligament technique. We paid specific attention to the distal catheter insertion technique, as the majority of obstructions seen in adults with INPH at our institution have been distal, consistent with previous studies. 5 Our cohort of 58 patients is a relatively large patient group who all underwent either initial or revision of VP shunt with a neurosurgeon performing the proximal shunt insertion or revision and a laparoscopic surgeon inserting the distal catheter using the falciform technique for fixation and guidance to the right upper quadrant above the liver. This technique prevents the catheter from being covered or coiling in the omentum or small bowel and allows cerebrospinal fluid drainage into the paracolic gutter potential space below the liver. We attained the benefit of natural fixation of the peritoneal catheter by passing it through a fenestration of the falciform ligament and did not encounter the morbidities associated with the technique of clipping the catheter in place. 12 Further imaging studies would need to be performed to validate long-term stability of catheter location.
Our series had no distal obstruction (0%) during the follow-up period, which is an improvement from published data. One patient was found to have a distal obstruction diagnosed with a shunt patency study 25 months after initial VP shunt placement using the falciform technique that fell outside of our study period. The European INPH study, with a 1-year follow-up, showed a distal catheter failure rate of 4%, proximal failure rate of 4% and overall need for revision of 15%. 13 A study of adult hydrocephalus from Johns Hopkins in Baltimore with a 24-month follow-up showed that 33% needed revision, of which 47% were due to distal obstruction. 4 There were no wound-associated infections, misplaced catheters, or intraabdominal injuries.
Reducing the rate of shunt obstruction should lead to reduced morbidity for patients, as well as reduced hospital admissions and costs, as the average cost of admission for possible shunt malfunction is $35,816. 3 The effect of a shunt procedure on 5-year Medicare expenditures in the elderly is a cost difference of $25,477 less per patient. 14
Using laparoscopy allows direct visualization of the distal catheter within the abdomen to assess obstruction and test catheter patency. Our technique requires trimming the intraabdominal portion of the distal catheter to a length of 30 cm so that the tip of the catheter will be at the right paracolic gutter. Shortening the catheter decreases the resistance to flow through the shunt system, which may be a factor influencing maintained patency. These modifications overcome many of the complications associated with earlier attempts at a falciform technique, including shunt obstruction from clips or sutures used to secure the distal catheter and involving intractable hiccups and right upper quadrant pain, 12 both presumably from irritation from cerebrospinal fluid collecting above the liver. 14 Although patients were not asked about hiccups, review of postoperative clinical notes revealed no patient complaints of hiccups or right upper quadrant pain.
Conclusions
The laparoscopic falciform technique significantly reduces the rate of distal VP shunt obstruction in adults with INPH. Continued follow-up is needed to confirm long-term patency of the catheter. A prospective trial comparing open laparotomy, standard laparoscopic technique, and the falciform ligament technique is warranted to confirm the results of our experience.
Footnotes
Disclosure Statement
No competing financial interests exist.