
Abstract
Abstract
Background:
A small percentage of patients fitted with a gastric band still experience “failure.” Here, the authors demonstrate the safety and feasibility of band preserving–laparoscopic gastric plication (BP-LGP), which was designed to improve weight loss and decrease gastric band adjustment frequency and thereby improve patient quality of life.
Materials and Methods:
All 6 patients involved in this study had a gastric band in place for more than 1 year; the median interval from gastric banding to BP-LGP was 31.7 months (range, 19.7–49.9 months). Five (83.3%) patients were female. Preoperative median body mass index (BMI) at gastric banding was 35.4 kg/m2 (range, 31.9–43.9 kg/m2), median nadir BMI with the gastric band was 25.7 kg/m2 (range, 20.9–31.0 kg/m2), and percentage excess BMI loss (%EBMIL) ranged from 24.3% to 123.6%. Indications for BP-LGP were as follows: chronic gastric prolapse in 2 patients (33.3%), pouch-esophageal dilatation in 3 (50.0%), and insufficient weight loss in 4 (66.6%), which included 2 patients with weight loss failure (%EBMIL of <30%).
Results:
The 6 patients consecutively underwent surgery from May 2014 to January 2015. No conversion to open surgery was necessary, and no perioperative complication or mortality occurred. Mean operative time was 190 minutes. All patients showed weight loss after revision and showed resolution of troublesome signs and symptoms. Median follow-up after revision was 7.3 months (range, 5.7–10.1 months), median BMI at last follow-up was 27.6 kg/m2 (range, 22.7–34.0 kg/m2), and median %EBMIL was 75.7% (range, 21.0%–103.6%). Median fill volume before revision was 6.1 mL (range, 2.7–11.0 mL), and median fill volume after revision was 0.3 mL (range, 0.0–5.3 mL). Three patients (50%) had an empty band at last follow-up.
Conclusions:
This novel method of bariatric revision (modified BP-LGP) might have a role as a salvage procedure in patients with impending gastric band failure.
Introduction
S
Herein, we propose a new revision technique for those with impending gastric band failure involving the addition of gastric plication with the band in situ, which we refer to as “band preserving–laparoscopic gastric plication” (BP-LGP), as originally stated by Huang et al. 3 in 2012. BP-LGP was designed to augment the weight loss and reduce gastric band adjustment frequency, thereby improving patient quality of life.
Materials and Methods
This clinical study was performed by retrospectively reviewing prospectively collected data of patients who underwent BP-LGP at Gil Medical Center (Gachon University College of Medicine, Incheon, Republic of Korea). The guidelines issued by the 2008 Asian Consensus Meeting on Metabolic Surgery in Trivandrum, India, for body mass index (BMI) restriction using bariatric surgery (see www.acmoms.com/acmom_2008.html) were followed throughout. In addition, we include those patients with a BMI of ≥25 and <30 kg/m2 and who were refractory to nonsurgical treatment for obesity (a BMI in this range poses moderate risk to Asians 4 ) for initial gastric banding surgery. BP-LGP was offered to patients as an alternative to “simple band-to-band revision” or “band removal with/without conversion to other surgery” and was performed according to patient preference, unless there was an absolute medical contraindication. Conservative management had been performed for at least 1 year before revision. Informed consent was obtained from all individual participants, and all were specifically informed that BP-LGP included an experimental procedure. All surgical procedures were performed with the patient under general endotracheal anesthesia.
In brief, a 36 French bougie was inserted transorally to the midesophagus level by an anesthesiologist before the patient was placed in the reverse 30° Trendelenburg position. A five-trocar port technique was used at the upper abdomen: one 12-mm trocar was placed at the umbilicus, two 5-mm trocars were placed on both anterior axillary lines 3–4 cm subcostally, and two 12-mm trocars were placed at both midclavicular lines, 5 cm subcostally. The BP-LGP procedure consisted of (1) disconnecting the band and port system, (2) laparoscopic nondestructive removal of the existing band, (3) repair of the hiatal widening if necessary, (4) gastric plication (plication first methods), (5) reinsertion of the band in its proper position, (6) band fixation with phrenogastric sutures, and (7) reconnection of the band and port system (Fig. 1).
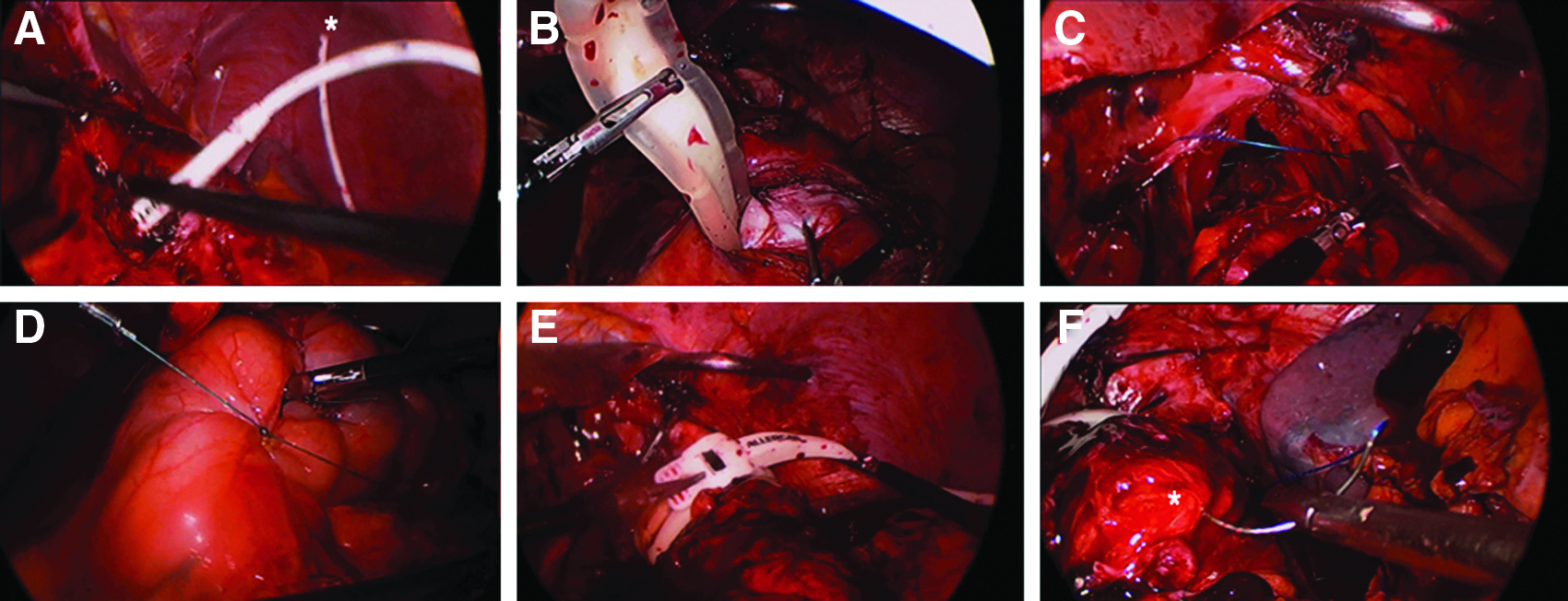
The band preserving–laparoscopic gastric plication technique.
Gastric infolding was performed using two layers of nonabsorbable sutures [inner interrupted sutures of 2-0 poly(ethylene terephthalate) (Ethibond®; Ethicon, Somerville, NJ) and outer continuous sutures of 2-0 polypropylene (Prolene®; Ethicon) or the V-Loc™ wound closure device (Covidien, Mansfield, MA)] under the guidance of a 36 French bougie, which had been advanced into the gastric lumen from midesophagus level just before infolding. The first row of sutures was started 2 cm below the gastroesophageal junction and proceeded until 3–4 cm proximal to the pylorus (usually 8–10 full-thickness nonabsorbable interrupted stitches were needed to complete the first row). This was intended to produce a suture to the lesser curvature distance of approximately 2 cm (36 French + gastric wall thickness × 2) as described in the series by Talebpour and Amoli. 5 Distances between sutures varied from 2 to 3 cm. The second row of sutures was started from the same point as the first row. Extramucosal running 2-0 Prolene sutures or V-Loc wound closure was used along the first row of sutures down to 3–4 cm proximal to the pylorus.
After BP-LGP, nil per os was maintained until nausea and sialorrhea subsided. Fowler's position was recommended on the day of surgery. Generous hydration was maintained along with intravenous esomeprazole (Nexium®; AstraZeneca, London, United Kingdom) (40 mg/day), metoclopramide (Macperan®; Donghwa Pharmaceutical Co., Ltd., Seoul, Korea) (30 mg/day), and granisetron (Kytril®; Roche Pharmaceuticals, Nutley, NJ) (1–2 mg/day). Discharge was considered when a patient tolerated sips of water, and on discharge patients were advised to progress to a soft diet in 15 days and to solid food in 30 days. Oral omeprazole (Losec®; AstraZeneca) (40 mg four times a day or 20 mg twice a day) was prescribed regularly for 3 months. The band was left empty for future band adjustment if necessary at least 6 months after BP-LGP. All procedures performed in this study were in accordance with the ethical standards of the institutional committee at our institution.
Results
Six patients consecutively underwent surgery from May 2014 to January 2015. During that period, 209 patients with a gastric band were followed up in our clinic.
The 6 patients had a gastric band in place for more than 1 year, and median time from gastric banding to BP-LGP was 31.7 months (range, 19.7–49.9 months). Five patients (83.3%) were female. Median preoperative BMI at gastric banding was 35.4 kg/m2 (range, 31.9–43.9 kg/m2), and median nadir BMI with a gastric band was 25.7 kg/m2 (range, 20.9–31.0 kg/m2) with percentage excess BMI losses (%EBMILs) ranging from 24.3% to 123.6%. In all patients, conservative management had failed to address their problems. Indications for BP-LGP were chronic gastric prolapse in 2 patients (33.3%), pouch-esophageal dilatation in 3 patients (50.0%), and insufficient weight loss in 4 patients (66.6%) (including 2 patients with a %EBMIL of <30% with a gastric band at BP-LGP) (Table 1).
%EBMIL, percentage excess body mass index loss; BI, band intolerance; BMI, body mass index; BP-LGP, band preserving–laparoscopic gastric plication; CGP, chronic gastric prolapse; F, female; FWL, failed weight loss; IWL, insufficient weight loss; LAGB, laparoscopic adjustable gastric band; PED, pouch-esophageal dilatation.
No conversion to open surgery was necessary, and no perioperative complication or mortality occurred. Median operative time was 190 minutes (range, 90–230 minutes). All patients showed weight loss after revision. Median follow-up after revision was 7.3 months (range, 5.7–10.1 months), and median BMI at last follow-up was 27.6 kg/m2 (range, 22.7–34.0 kg/m2) with a median %EBMIL of 75.7% (range, 21.0%–103.6%). Troublesome symptoms resolved in all patients. Median fill volumes before and after revision were 6.1 mL (range, 2.7–11.0 mL) and 0.3 mL (range, 0.0–5.3 cmL), respectively. Three patients (50%) had an empty band at last follow-up (Table 2).
Time between gastric banding (primary operation) and band preserving–laparoscopic gastric plication (BP-LGP) (revision).
BMI, body mass index; FU, follow-up.
Discussion
This study demonstrates BP-LGP is feasible and effective as a revisional procedure for those with impending gastric band failure. Aside from the acute or subacute complications of an adjustable gastric band, which include band erosion and acute band slippage/prolapse, chronic complications, such as pouch-esophageal dilatation, chronic gastric prolapse, and band intolerance (in the long term), result in insufficient or failed weight loss because it is not possible to adjust the band properly in these patients.
At a median 7.3 months of follow-up after BP-LGP, all 6 of our patients showed additional weight loss with a median percentage excess weight loss increase of approximately 30%. Furthermore, median fill volume before revision was 6.1 mL (range, 2.7–11.0 mL), and median fill volume after revision was 0.3 mL (range, 0.0–5.3 mL); 3 patients (50%) had an empty band at a median follow-up of 6 months.
We developed interest in BP-LGP as a means of band revision because, occasionally, patients with a gastric band require conversion to sleeve gastrectomy or gastric bypass due to insufficient weight loss (or resolution of comorbidities) or specific gastric band–associated alimentary intolerances (frequent clogging of food or reflux). These situations are more common in those who have experienced insufficient weight loss for several years after gastric banding or symptoms that might be attributable to chronic band slippage/prolapse. However, body weight can remain constant or even increase after conversion, possibly due to a relatively “normal” food intake without the patients' gastric band. In fact, the weights of such patients at re-operation are falsely low due to chronic reflux, regurgitation, dysphagia, and food intolerance, which are typical symptoms of a dysfunctional band. 6 On the other hand, band-to-band revision (band repositioning or replacement) often results in secondary failure caused by the recurrence or exacerbation of gastric band–associated problems.7,8 All of our cohort of patients except 1 (Patient 6) had shown initial meaningful weight loss with the band only. Their median nadir BMI with the band was 24.8 kg/m2 (range, 20.9–27.2 kg/m2) with a median nadir %EBMIL of 101.2% (range, 80.4%–123.6%), and they did not want more complex surgery, such as sleeve gastrectomy or gastric bypass. It has been suggested that the course after primary banding before failure is the main indicator of future success, 8 which was our rationale for preserving the band in our cohort of patients.
We would like to focus on the reason for band failure in our patients, as well as how BP-LGP corrected the problems. In Patients 1 and 4, initial weight loss after LAGB was excellent (nadir %EBMIL was 123.6% and 101.2%, respectively), but with time, they presented moderate to severe nighttime reflux and weight regain due to a large pouch above the band. Conservative management, including band adjustment (unfilling/refilling) and dietary education, was not effective. After BP-LGP, both the patients showed additional weight loss with smaller filling volume, and their reflux symptoms were completely resolved, which is probably the result of the looser band that is associated with the lesser amount of filling volume after BP-LGP and the resulting normalization of the pouch above the band (Fig. 2). In both patients, hiatal defects were closed during BP-LGP.
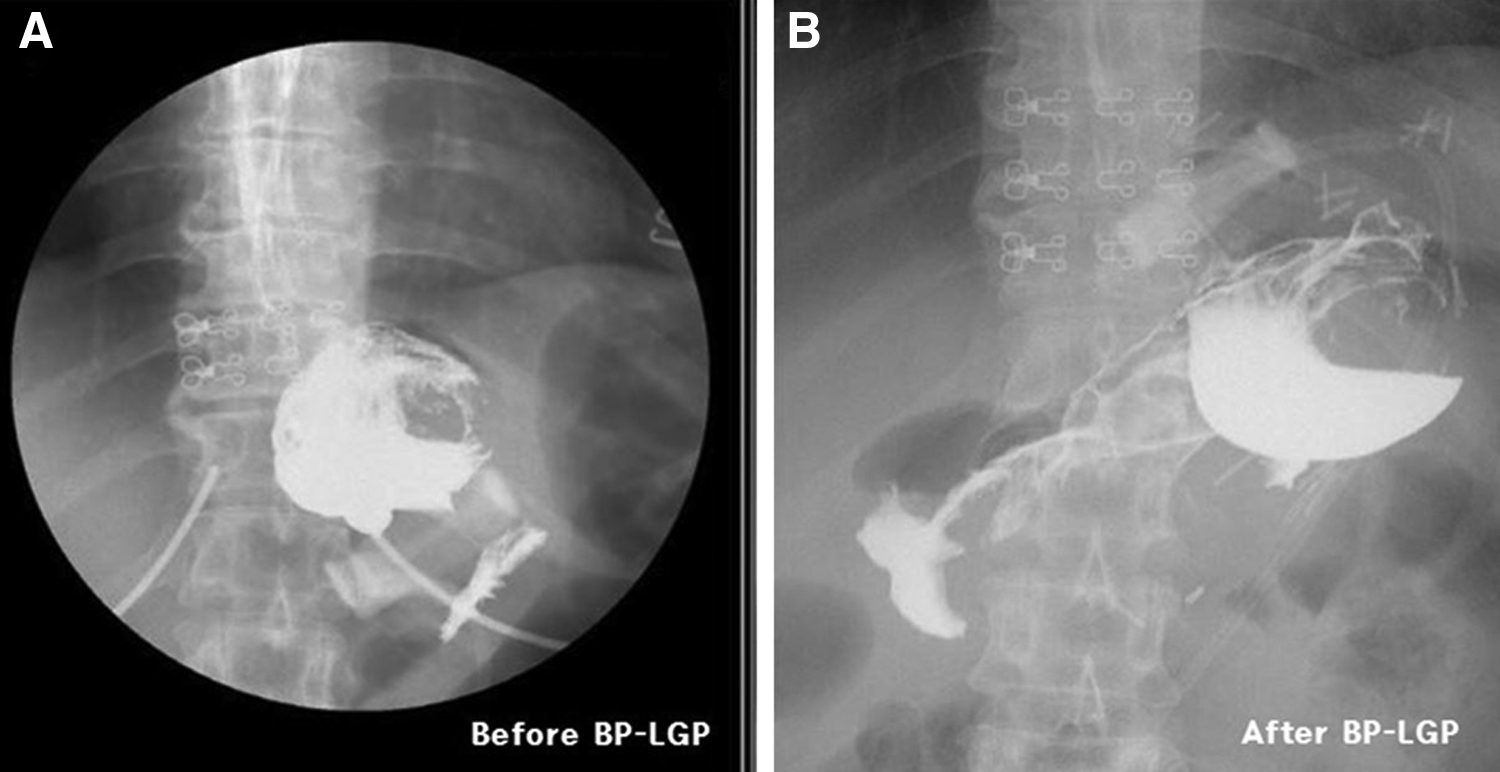
The fluoroscopic images of Patient 4.
Patient 2 was referred from another hospital for severe esophageal dilatation and solid dysphagia. However, band adjustment (total unfilling and gradual refilling) with dietary education was not effective because weight loss was not possible every time we deflated the band, whereas esophageal widening and motility disturbances worsened every time we inflated the band. Band removal was seriously considered, which was refused by the patient. After BP-LGP, additional weight loss occurred with a lesser amount of filling volume. The patient commented that “I'm happy to eat real food.” Although esophageal dilatation has been corrected radiologically at 7.8 months after BP-LGP, we carefully follow up and educate the patient for modifying eating habits because there is concern that esophageal dilatation would recur, depending on the amount of filling volume.
In Patients 3 and 5, chronic gastric prolapse was diagnosed. Both had a history of emergency total unfilling due to “gastrospasm.” After that, they occasionally showed gross food intolerance with a relatively small increment in filling volume and relief when the increment was removed; therefore maintenance of weight was not possible. Under the safe fill volume, weight loss never happened, and eventually the patients underwent revision. During BP-LGP, the band was placed correctly, and the fundus was plicated and anchored to the left crural fascia.
Patient 3 showed suboptimal weight loss with a % EBMIL of 21% at 8.6 months even after BP-LGP. Actually, this patient hesitated to have an adjustment for fear of food intolerance as experienced before BP-LGP. However, we expect that the patient would reach her relevant weight goal with serial band adjustments without such discomfort. Currently, the patient is losing weight slowly with an empty band but has no discomfort.
Finally, 1 patient (Patient 6) was, in fact, a follow-up-loss patient after gastric banding. She showed up again for poor weight loss and intolerance of band (frequent vomiting, solid dysphagia). Therefore we added plication to augment her weight loss and quality of life. The patient achieved remarkable %EBMIL (76.3%) after 6 months after BP-LGP. The patient is very satisfied with the result of BP-LGP.
Unexpectedly, we observed that filling volume decreased after BP-LGP. Median fill volumes before and after revision were 6.1 mL (range, 2.7–11.0 mL) and 0.3 mL (range, 0.0–5.3 mL), respectively. Three patients (50%) had an empty band at last follow-up. For the 3 patients who had band filling after BP-LGP, adequate restriction was achieved by a smaller amount of saline, the effect of which can be explained by Boyle's law: PV = C (constant), where in this case P = intragastric pressure and V = intragastric volume. It has been suggested that pressurization of the cardia above the LAGB, probably activating gastric mechanoreceptors that relay via the vagus nerve, or direct pressure or contact of the LAGB against the gastric wall induces satiety of LAGB patients. 9 Therefore, it is our understanding that in BP-LGP, intragastric pressure increases due to gastric volume reduction by plication below the band, and this increased intragastric pressure might help satiety at smaller band filling volumes. We have witnessed that patients could not tolerate it if the filling volume reached the pre–BP-LGP level. Therefore, we speculate that BP-LGP has more effect than the additive effect of a band and plication because reductions in the numbers and amounts of band adjustment are clear benefits of BP-LGP as compared with band-to-band revision, when one considers the costs of hospital visits and of various port complications, such as infections and port-reservoir damage.
However, BP-LGP is not a panacea or an ideal revisional procedure for adjustable gastic banding, as it has several inherent problems. Average operation time in the present study was rather long at 190 minutes (range, 70–230 minutes) because two operations were combined. Long operation time and general anesthesia are clearly demerits of this procedure when cost and postoperative recovery are considered. Actually, gastric plication accounted for most of the operative time during BP-LGP. However, operating time would undoubtedly be decreased by familiarization of the plication technique. Other studies have shown the gastric band plus plication procedure has greater risk than the gastric band procedure alone or sleeve gastrectomy,10,11 which was attributed to rare but serious complications specific to gastric plication, such as fold prolapse, gastric obstruction, and perforation. Another concern is the possibility of gastric inlet obstruction caused by invagination of the first plicated fold through the band stoma orifice, and thus the first fold should be located cautiously to prevent this complication. Multiple-stitch plication or intraoperative endoscopic surveillance of the first fold could prevent gastric inlet obstruction.
The obvious limitations of this study are its small cohort and short-term follow-up. It is possible that the plication effect would disappear with time due to physiologic dilatation of stomach caused by smooth muscle relaxation. Furthermore, in some poorly motivated patients, chronic problems associated with gastric band before BP-LGP might recur, although all kinds of band revision present this risk. Summarizing, we believe this novel method of bariatric revision (BP-LGP) might have a role as a salvage procedure in patients with impending gastric band failure.
Footnotes
Disclosure Statement
No competing financial interests exist.