
Abstract
Abstract
Pelvic exenteration is used in the treatment of several pelvic cancers, including those of the rectum, uterus, and bladder. We report the first case of robotic pelvic exenteration for the treatment of symptomatic prostate cancer involving the rectum and bladder. A six-port transperitoneal robotic approach was used. Bilateral extended lymphadenectomy up to the inferior mesenteric artery was performed. The rectum and bladder were removed en bloc, and a double-barrel anastomosis was then performed with both ureters being connected to the lower opening of the colostomy. Operative time was 249 minutes, and estimated blood loss was 600 mL. No intraoperative or postoperative complications were recorded. Biopsy of the rectum and bladder showed prostatic adenocarcinoma with a Gleason score of 9 (5+4), and 1 of 17 nodes was positive for cancer. Postoperative prostate-specific antigen level was 1.24 ng/mL. The patient is already 19 months after surgery with optimal quality of life. Thus pelvic exenteration is a feasible alternative for highly symptomatic prostate cancer involving adjacent pelvic organs.
Introduction
S
Prostate cancer is the most frequently diagnosed cancer and the second leading cause of death from cancer in men in the United States. It was estimated that around 242,000 men were diagnosed and more than 28,000 eventually succumbed to prostate cancer in 2012. 2 Despite this high incidence, macroscopic involvement of pelvic organs is rare before end-stage disease. When it occurs it usually presents with disabling symptoms such as perineal pain, rectal bleeding, hematuria, and fecal and urinary obstruction. Estimated survival at this stage is usually around 12–24 months. 3 The role of total pelvic exenteration in symptomatic locally advanced prostate cancer is not well established but could aid in palliation of these highly disabling symptoms.
Robotic pelvic exenteration has been initially reported for colorectal cancer. 4 However, there are no reports yet on complete robotic exenteration for urological cancer. Hence, we present what we believe is the first report on robot-assisted total pelvic exenteration in a highly symptomatic patient with prostate cancer having rectal and bladder involvement.
Case Report
We present the case of a 71-year-old man who underwent a radical prostatectomy in 1995 for prostate cancer at 53 years of age. Two years later he had salvage radiotherapy due to biochemical recurrence. The patient came into our care in March 2005 with a prostate-specific antigen (PSA) level of 0.94 ng/mL. He was subsequently placed in intermittent androgen ablation due to a rising PSA level and eventually became castration resistant in July 2012. Several months later he complained of rectal bleeding and severe tenesmus. His PSA level at the time was 25.47 ng/mL. A digital rectal examination was performed and showed a mass in the rectal canal, with a subsequent colonoscopy showing a friable mass in the anterior rectal wall 3 cm from the anal margin with signs of mucosal infiltration up to 10 cm from the anal margin (Fig. 1). Complementary bone scan, computed tomography scan, and [18F]fluorodeoxyglucose positron emission tomography/computed tomography scan were performed and showed a 3.7-×1.7-cm contrast-enhancing bladder nodule involving the left ureteral meatus and causing ipsilateral hydronephrosis, a 3.9-cm mass in the prostatic bed with infiltration of the anterior rectal wall (Fig. 2), and enlarged regional lymph nodes up to 13 mm. No bone metastases were identified. Rectal biopsy demonstrated prostatic adenocarcinoma with extensive necrosis and ulceration.
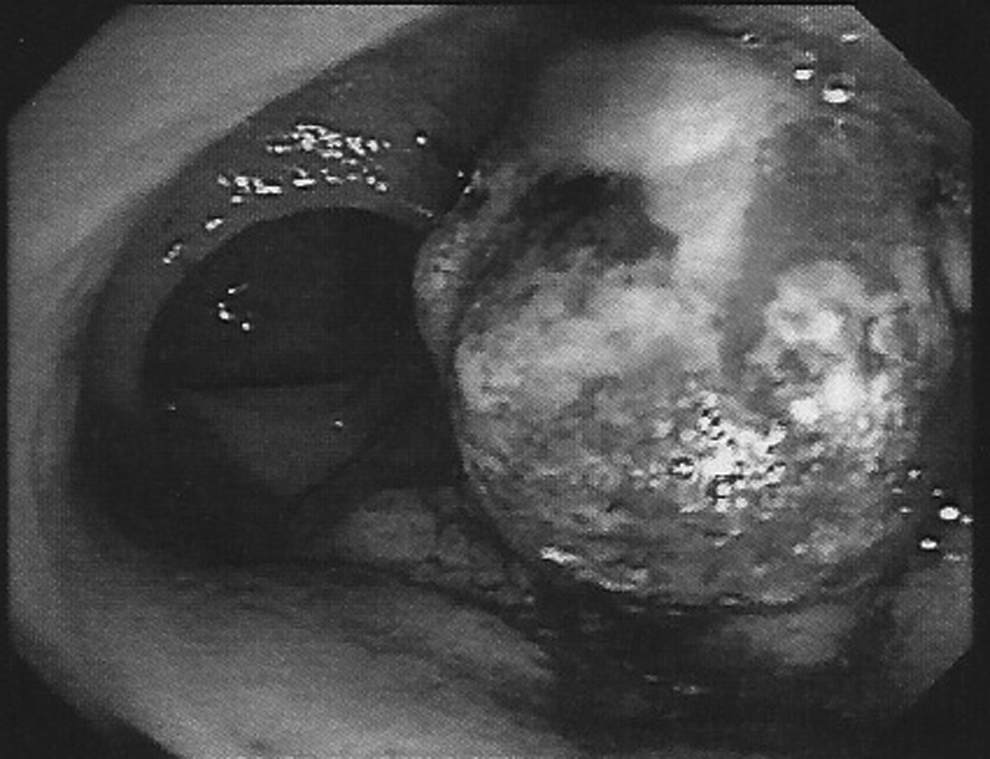
Colonoscopy shows prostate cancer involvement of the anterior rectal wall and lumen.
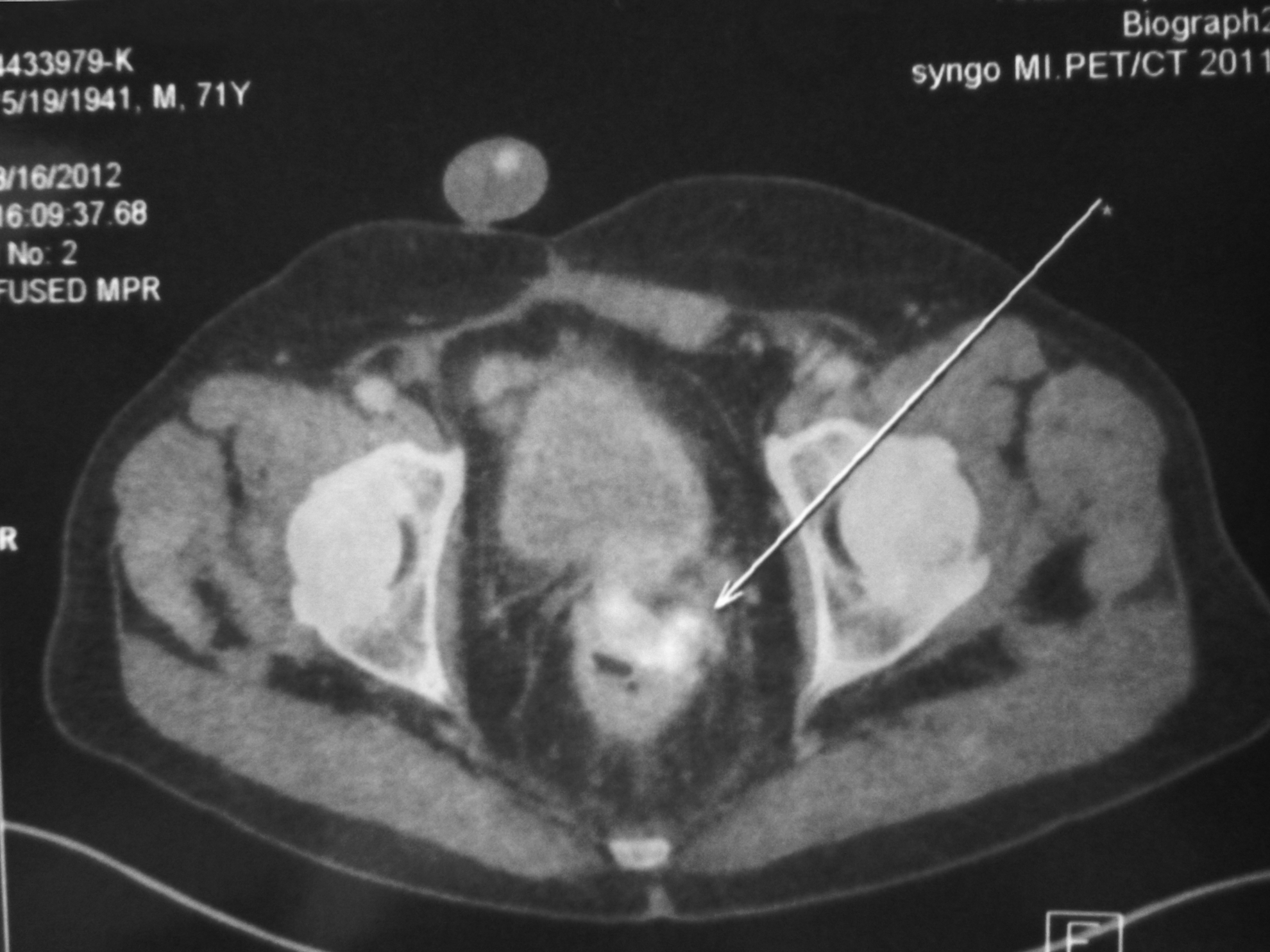
[11C]Choline positron emission tomography/computed tomography showing the tracer marking posteriorly through the rectal wall (arrow).
A robotic pelvic exenteration was performed using a six-port transperitoneal approach as for a radical cystectomy. Both ureters were dissected and cut close to the bladder. A bilateral extended pelvic lymphadenectomy with the upper limit at the inferior mesenteric artery was subsequently performed. The sigmoid colon was then freed and cut at the rectosigmoid union with a laparoscopic stapler. The rectum and the bladder were then en bloc excised after controlling the respective vascular pedicles. The surgery was completed from the perineal approach where the surgical specimen was extracted. Urinary and fecal diversion was achieved through a double-barreled wet colostomy. A loop colostomy was created 10–15 cm proximal to the previously sectioned rectosigmoid junction and exteriorized at the left lower quadrant. The ureters were then individually anastomosed robotically to the end of the distal stump. The pelvic dead space was then filled with an absorbable polypropylene mesh, and two percutaneous drains were left (Fig. 3).

Postoperative cosmetic results. The previous scar is from radical prostatectomy, robotic ports, and stoma on the left lower quadrant.
Operating time was 249 minutes, divided as follows: 13 minutes for ports and docking, 110 minutes for lymphadenectomy, 66 minutes for exanteration, and 60 minutes for ureteral anastomosis and colostomy. Estimated blood loss was 600 mL. Postoperative course was uneventful, with the patient being discharged on postoperative Day 7.
Histopathology informed extensive rectal and vesical infiltration from prostatic acinar adenocarcinoma with a Gleason score of 9 (5+4). Lymph node yield was 17, with one right external iliac node positive for cancer.
Six weeks after surgery his PSA level was 1.39 ng/mL. The patient is currently in androgen deprivation therapy and was also treated with chemotherapy with docetaxel. He is now 24 months postoperative with a PSA level of 2.37 ng/mL and a good quality of life.
Discussion
Total pelvic exenteration has been widely used to remove or palliate a variety of pelvic cancers, including those of the cervix, rectum, vagina, uterus, and bladder.5,6 Since the first report by Brunschwig 1 in 1948, surgical technique and knowledge have dramatically changed, and now this procedure results in good quality of life for most patients.7,8 Notwithstanding, the morbidity is still high, with around 13%–64% of the patients reporting some kind of procedure-related complication. 9
The Bricker ileal conduit is the most common type of urinary diversion. However, it might be less suitable in cases of pelvic exanteration as these patients need an additional stoma for concurrent fecal diversion, complicating daily handling and decreasing their quality of life. Double-barrel wet colostomy was first described by Carter et al. 10 in 1989. The procedure was done in a patient with severe actinic pelvic disease and consisted of simultaneous fecal and urinary diversion using a single stoma. A reservoir distal to the stoma is used for urinary diversion with free urine drainage and no contact with feces. Its main advantage is the prevention of fecal reflux to the ureteral anastomosis by total separation of the fecal content, thus achieving a significantly decreased risk of ascending pyelonephritis.
Kecmanovic et al. 7 reported on 38 patients who underwent double-barreled wet colostomy for urinary and fecal diversion. Postoperative morbidity was 15.7% with no treatment-related mortality.
Kamat et al. 8 published a report on 14 patients with locally advanced prostate cancer with untractable perineal pain and rectal symptoms who underwent total pelvic exanteration during a 7-year period. Eleven (79%) had complete relief of pain symptoms, and all the rest had significant relief. The average symptom-free period was 14.1 months (range, 3–36 months). Seven patients eventually died from prostate cancer at a median of 24 months.
Locally advanced pelvic cancers can cause severely disabling symptoms, including perineal pain, hematuria, hematochezia, and urinary and fecal obstruction. Macroscopic involvement of pelvic organs, especially the rectum, is uncommon in prostate cancer. It is believed that Denonvillier's fascia could act as a natural barrier to the extension of prostate cancer posteriorly. However, when it happens it can lead to disabling symptoms such as intractable perineal pain and rectal dysfunction. Radical surgery in these cases is in many cases the only possibility of achieving a satisfactory palliation.
Amid very limited data, the role of robotic surgery in pelvic exenteration is far from being elucidated, yet it demonstrated feasibility and could potentially transfer the benefits of minimally invasive surgery to this highly morbid procedure.
Footnotes
Disclosure Statement
O.A.C. has been a Proctor of the da Vinci Surgical System (Intuitive Surgical Inc.) for Latin America. I.V.-M., A.R.-C., A.S., and O.S. declare no competing financial interests exist.