
Abstract
Abstract
Objective:
To evaluate the clinical effectiveness and safety of percutaneous transhepatic papillary balloon dilatation (PPBD) combined with laparoscopic cholecystectomy (LC) for the treatment of gallstones with common bile duct stones.
Materials and Methods:
From February 2012 to January 2013, 65 patients (31 males and 34 females) who had gallstones with common bile duct stones were divided into two groups: endoscopic papillary balloon dilatation (EPBD)+LC (n = 40 cases) and PPBD+LC (n = 25 cases). The maximum transverse diameter of common bile duct stoned was 15 mm. White blood cell count and serum amylase level were measured at 12 hours and 72 hours after the operation, and operation time, time of gastrointestinal function recovery, and hospitalization time were analyzed.
Results:
No case in either group was converted to open surgery. The stones were successfully pushed out into the duodenum in all patients of both groups. One case of postoperative pancreatitis (2.5%) and 5 cases of hyperamylasemia (12.5%) occurred among the 40 patients in the EPBD+LC group. In contrast, no case of postoperative pancreatitis and 2 cases of hyperamylasemia (8%) occurred among the 25 patients in the PPBD+LC group. The serum amylase level at 12 hours postoperatively was statistically significantly different (307 ± 39.94 IU/L in the EPBD+LC group and 193 ± 30.78 IU/L in the PPBD+LC group; P < .05). There were no significant differences between the two groups in operative time, postoperative gastrointestinal function recovery time, or hospital stay time (P > .05). During follow-up of 2 years, 1 case of recurrence for common bile duct stones was discovered and was treated successfully with EPBD repeatedly.
Conclusions:
PPBD combined with LC simultaneously is an alternative effective and safe procedure for the treatment of gallstones and bile duct stones, especially for those patients who are unsuitable for endoscopic treatment.
Introduction
L
Percutaneous transhepatic papillary balloon dilatation (PPBD) has been used successfully to manage removal of bile duct stones; PPBD reduces the mechanical damage to the duodenal papilla during the removal of stones and decreases the incidence of postoperative pancreatitis.1,2 For cases of endoscopic treatment failure, PPBD combined with LC could be a useful alternative option for the treatment of gallstones and bile duct stones.
Materials and Methods
Patients
A retrospective study was carried out from February 2012 to January 2013 involving 65 patients (31 males and 34 females) who were diagnosed by computed tomography or magnetic resonance imaging scan to have gallbladder stones combined with common bile duct stones. Subjects were divided into two groups according to treatment: EPBD+LC (n = 40 cases) and PPBD+LC (n = 25 cases) (18 cases of postgastrectomy Billroth II restriction and 7 cases of failed cannulation to the bile duct). Patient age ranged from 42 to 75 years (median age, 61 years). The maximum transverse diameter of a common bile duct stone was 15 mm. No significant difference was found between the two groups for age, sex, stone size, or preoperative total bilirubin level (Table 1).
EPBD, endoscopic papillary balloon dilatation; LC, laparoscopic cholecystectomy; PPBD, percutaneous transhepatic papillary balloon dilatation.
We performed the operation after patients had recovered from acute cholangitis, jaundice, liver dysfunction, and acute pancreatitis (white blood cell count, ≤10 × 109/L; total bilirubin, ≤34 μmol/L; alanine aminotransferase, ≤60 U/L; C-reactive protein, ≤10 mg/L). Written informed consent was obtained from each patient. Exclusion criteria included concurrent hepatolithiasis, acute pancreatitis, pancreatic or biliary malignancy tumor, and severe coagulation dysfunction.
Procedures
PPBD
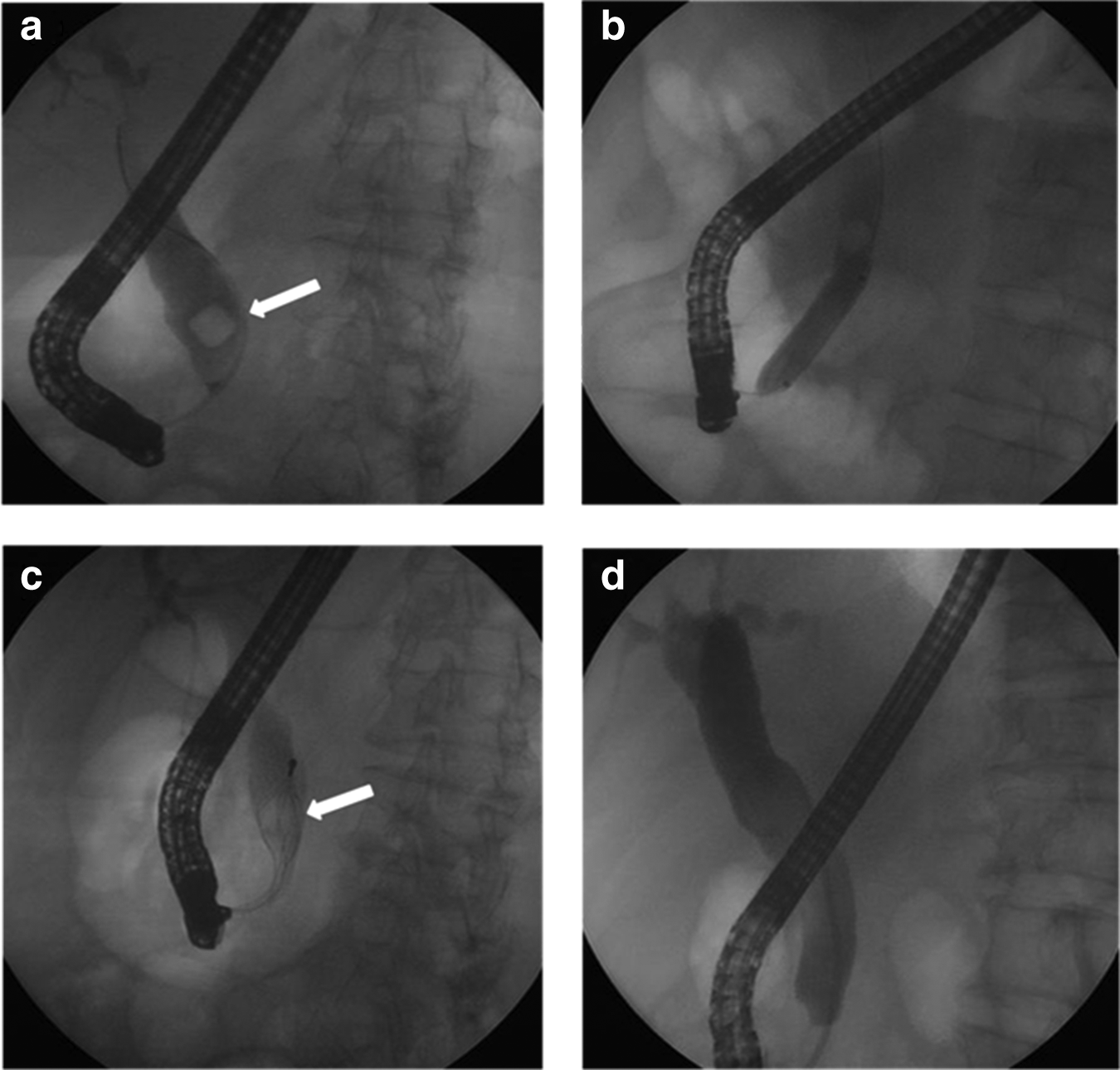
Surgery was performed under fluoroscopic monitoring. The puncture site was located in the right axillary line at intercostal space 8–9. The right hepatic duct was punctured with a 21-gauge Chiba needle (Cook Medical, Bloomington, IN). The route of the biliary system was observed by angiography. A short 0.035-inch-diameter guide wire (Terumo, Tokyo, Japan) was used to insert a 6-French introducer sheath (Terumo) into the target bile duct. A 260-cm-long 0.035-inch-diameter guide wire was advanced through the papilla and into the duodenum, the balloon catheter was passed over the guide wire to the duodenum under fluoroscopic guidance, and the middle portion of the balloon was located at the biliary sphincter. The balloon was slowly filled with contrast medium by using an inflation device for which the maximum pressure was 6–8 atmospheres and maintained for 1–2 minutes, until the balloon waist had disappeared under fluoroscopic guidance. The balloon ranged in diameter from 8 to 15 mm, based on the diameter of the stone. The common bile stone was pushed out into the duodenum with the inflation balloon (Fig. 1). A 8.5 French external drain pigtail catheter (Cook Medical) was placed with its distal end in the common bile duct, which was removed after 5–7 days if postoperative cholangiography was normal.

Percutaneous transhepatic papillary balloon dilatation for the removal of common bile duct stones.
EPBD
The procedure was performed with a duodenoscope (model JF 260; Olympus Co., Ltd., Tokyo, Japan) for endoscopic retrograde cholangiopancreatography (ERCP), and biliary cannulation was achieved using a transpapillary approach with an ERCP catheter. A triple-sized dilator balloon (CRE™ wire-guided balloon dilation catheter; Boston Scientific, Galway, Ireland) was inserted into the bile duct, and the balloon catheter was passed over a guide wire retrogradely. When it was positioned at the biliary orifice, the balloon was then gradually inflated with contrast medium until the waist of the balloon had disappeared under endoscopic and fluoroscopic guidance. The balloon diameter was 10–15 mm, depending on the sizes of the stones and bile duct. The balloon was maintained in position for 60 seconds and then deflated. The bile duct stones were removed into the duodenum with a basket (Fig. 2). A nasobiliary catheter was placed in the bile duct and was removed after 3 days if postoperative cholangiography was normal.
Endoscopic papillary balloon dilatation for the removal of common bile duct stones.
LC
The procedure was performed in the usual way.
Clinical data
White blood cell count and serum amylase level were measured at 12 hours and 72 hours after the operation. The operation time, time of gastrointestinal function recovery, and hospitalization time were analyzed. Postoperative pancreatitis was defined as a serum amylase level of ≥500 IU/L, combined with persistent epigastric pain. Hyperamylasemia was defined as a serum amylase level of ≥500 IU/L, but without abdominal symptoms.
Statistical analysis
Statistical analysis was performed with SPSS version 17.0 software (SPSS, Inc., Chicago, IL). Continuous variables were expressed as mean ± standard deviation values. Categorical and binary variables were tested using the chi-squared test. Student's t test was used for statistical comparisons between the two groups. A value of P < .05 was considered to indicate statistical significance.
Results
No case in either group was converted to open surgery, and no deaths or other major complications occurred. The stones were successfully pushed out into the duodenum in all patients of both groups. One case of postoperative pancreatitis (2.5%) and 4 cases of hyperamylasemia (12.5%) occurred among the 40 patients in the EPBD+LC group. In contrast, no case of postoperative pancreatitis and 2 cases of hyperamylasemia (8%) occurred among the 25 patients in the PPBD+LC group. The serum amylase level at 12 hours postoperatively was statistically significantly different (307 ± 39.94 IU/L in the EPBD+LC group and 193 ± 30.78 IU/L in the PPBD+LC group; P < .05). Both groups had no bleeding or perforation cases. There were no significant differences between the two groups in serum amylase level 72 hours postoperatively, operative time, postoperative gastrointestinal function recovery time, or hospital stay time (P > .05) (Table 2). During follow-up of 2 years, 1 case of recurrence for common bile duct stones was discovered and was treated successfully with EPBD repeatedly.
EPBD, endoscopic papillary balloon dilatation; LC, laparoscopic cholecystectomy; NS, not significant; PPBD, percutaneous transhepatic papillary balloon dilatation.
Discussion
LC is the optimum treatment of choice for gallstones owing to minor trauma and faster recovery. For the treatment of common bile duct stones, an approach involving both laparoscopic and endoscopic has been implemented extensively. However, a debate still exists regarding how to treat the two diseases simultaneously.
The laparoscopic transcystic approach is more limited by retrieval of only small stones and inconvenient access to the bile duct. LCBDE has been demonstrated to be an effective treatment for common bile duct stones, with a stone clearance rate ranging from 84% to 97%, a postoperative morbidity rate of 4%–16.4%, and a mortality rate of approximately 0%–0.8%.3–5
T-tubes were traditionally inserted in the open bile duct after removal of stones, and morbidity rates related to T-tube use have been reported to be 4%–16.4% in the laparoscopic era. 6 The T-tube–related complications include bile leakage, bile infection, and bleeding, as well as cholangitis from exogenous sources through the T-tube. Furthermore, the patients have to keep the bile drainage tube in place for several weeks, which caused great discomfort.
An increasing tendency option for choledochotomy is primary closure without the use of a T-tube. Gurusamy et al. 7 in a meta-analysis found that there was no significant difference in the serious morbidity rates (17/147 in the T-tube group versus 9/148 in the primary closure group). Compared with the T-tube group, the operating time and hospital stay of the primary closure group were significantly shorter. But after primary closure, the cholangiography and clearance of residual stones are unreliable. Additionally, biliary stricture cannot be avoided completely as a long-term complication after common bile duct exploration, which is very difficult to deal with. Therefore, as with any surgical intervention, an assessment of operative risk needs to be made.
Bansal et al. 8 compared LCBDE+LC with ERCP+LC for patients with gallstones and common bile duct stones; the surgical success rates were similar (91.7% versus 88.1%) in the two groups, but the mean operative time was significantly longer in the LCBDE+LC group. A meta-analysis 9 indicated the incidence of bile leakage in the ERCP+LC group was lower than that in the LCBDE+LC group. There was no statistically difference between the two approaches in terms of other major complications. However, mortality rates associated with choledochotomy exploration are around 4% in high-risk elderly patients, especially those who are subjected to urgent biliary drainage procedures. 10
Endoscopic sphincterotomy (EST) has been established as the main treatment for bile duct stones since 1974. Although the success rate of EST is high, this procedure may cause pancreatitis, bleeding, perforation, and other acute complications. Furthermore, it can damage the function of the papilla sphincter, which causes chronic complications such as enteric-biliary reflux, bacterial infection, and inflammation of the biliary system. 11 EPBD was described by Staritz et al. 12 for the management of common bile duct stones. Ersoz et al. 13 in 2003 reported EST combined with large-diameter (12–20 mm) EPBD to remove large bile duct stones, with a success rate of 83% in the first session and an overall complication rate of 15.5%. Two meta-analyses, by Baron et al. 14 (8 studies analyzed) and Weinberg et al. 15 (15 studies analyzed), showed that there were no statistically significant differences in the success rate for stone removal between EST and EPBD (94.3% versus 96.5%), and overall complication rates were similar in the EPBD and EST groups (10.5% versus 10.3%). Compared with EST, EPBD had a lower stone recurrence rate. However, a higher incidence of pancreatitis after EPBD was reported in some studies. 16 In a multicenter study Disario et al. 17 reported 2 patients with fatal pancreatitis. Tsujino et al. 18 show that the post-EPBD pancreatitis rate was 4.8% of their 1000 patients, but all of them recovered later. EPBD preserved the function of the sphincter of Oddi and reduced risk of bleeding and perforation.19,20
Some patients with common bile duct stones are unsuitable for endoscopic therapy because of an altered gastrointestinal anatomy after Billroth II gastrectomy, a strictured upper gastrointestinal tract, or failed cannulation of the bile duct. PPBD as an interventional radiologic method may provide an effective and safe procedure without choledochotomy and preserve the function of the sphincter of Oddi. In 1981, Centola et al. 21 described PPBD for the successful treatment of common bile duct stones. Seo et al. 22 indicated that the rate of successful stone removal was 97.1% in EPBD cases and 98.2% in PPBD cases, postoperative pancreatitis occurred in 14 (6.7%) of 208 cases in the EPBD group and none (0%) of 56 cases in the PPBD group (P = .046), and the incidence of hyperamylasemia was 29.8% in the EPBD group but 7.1% in the PPBD group (P = .0005). Fumio et al. 23 described that gallstones and bile duct stones can be treated by percutaneous transhepatic papillary ballon (PTBD)+LC simultaneously with the patient under general anesthesia; there were no deaths and major complications and no case converted to open surgery, serum amylase levels in 10 cases among 21 patients were transiently elevated (serum amylase levels >200 IU/L) and recovered within 7 days, and no severe pancreatitis occurred.
In our study 1 case of postoperative pancreatitis (2.5%) and 4 cases of hyperamylasemia (12.5%) occurred in the EPBD+ LC group. In contrast, there were no cases of postoperative pancreatitis and 2 cases of hyperamylasemia (8%) in the PPBD+LC group. The serum amylase level at 12 hours postoperatively was 307 ± 39.94 IU/L in the EPBD+LC group and 193 ± 30.78 IU/L in the PPBD+LC group. EPBD may traumatize the orifice of the pancreatic duct associated with repeated cannulation. The numerous contrast medium injected into the pancreatic duct was considered to be a significant risk factor of pancreatitis. However, in PPBD, because the procedure applied antegrade balloon dilation, selective cannulation was unnecessary, and no contrast medium was injected into the pancreas duct. In both EPBD and PPBD, indwelling biliary drainage contributed to reduce the postoperative incidence of severe pancreatitis and cholangitis.
In this study LC was implemented instantly for the patients after removal of the common bile duct stones, although the triangle of Calot surrounding the tissue was mildly edematous, but not enough to contraindicate the operation. There were no cases converted to open surgery. Some research indicated that a one-stage approach combining ERCP and cholecystectomy was a safe and effective method with a low risk of postoperative pancreatitis, as well as being more comfortable for the patients and also reducing the mean hospital stay.24,25 Undoubtedly, our study had certain limitations. Retrospective analyses have inherent selection and information biases, especially with the limited number of cases that were enrolled. A multicenter prospective randomized control trial would be helpful to demonstrate the feasibility of this technique.
In conclusion, for the treatment of gallstones and bile duct stones, PPBD combined with LC simultaneously is an alternative effective and safe procedure, especially for those in whom the endoscopic procedure was a failure.
Footnotes
Disclosure Statement
No competing financial interests exist.