
Abstract
Abstract
Background:
Laparoscopic caudate hepatectomy, which is a challenging procedure, has been reported sporadically. However, there is no standardized surgical technique, and the safety and feasibility of this procedure remain controversial.
Materials and Methods:
A left-sided, purely laparoscopic approach for anatomic caudate hepatectomy was used for 11 selected patients in our institution. The procedure and technique of laparoscopic caudate hepatectomy were described. Perioperative data of these patients were retrospectively reviewed.
Results:
The 11 cases included two subgroups: laparoscopic isolated caudate hepatectomy (n = 4) and laparoscopic combined caudate and left hemihepatectomy (n = 7). There were three major steps for anatomic caudate hepatectomy. Two conversions were required (18.2%). Two complications (Clavien Grades I and II) occurred but no deaths.
Conclusions:
The left-sided, purely laparoscopic approach for anatomic caudate hepatectomy is safe and feasible in selected patients. This procedure can be performed by hepatobiliary surgeons with abundant experience in laparoscopic liver surgery.
Introduction
I
The caudate lobe, because of its unique anatomy, has often been considered the forbidden zone of laparoscopic hepatectomy. Even so, with the encouraging outcomes of laparoscopic liver resection and the accumulation of surgical experience, there have been sporadic attempts to apply the laparoscopic approach to the caudate lobe. There is still not a standard surgical technique for laparoscopic caudate hepatectomy (LCH). In this study we introduce our experience and evaluate the feasibility and safety of a left-sided, purely laparoscopic anatomic caudate resection in selected patients.
Materials and Methods
Patients
Laparoscopic liver resection has been performed since 1998 in our center. With accumulation of experience, we performed the first LCH in 2007. We applied strict inclusion and exclusion criteria for laparoscopic caudate lobe resection. Inclusion criteria for the laparoscopic procedure were as follows: indications for caudate hepatectomy, Child–Pugh Class A, and lesion size less than 5 cm in patients with tumors. Exclusion criteria were as follows: hilar cholangiocarcinoma, severe extrahepatic bile duct stricture, suppurative cholangitis in patients with hepatolithiasis, vascular invasion, previous major open surgery in the epigastrium, and an American Society of Anesthesiologists score of 4 or more.
A total of 11 patients underwent laparoscopic anatomic caudate lobectomy between January 2007 and December 2013 in our institution. Caudate lobe wedge resection and biopsy were excluded from the analysis. Caudate resection could be performed as a combined procedure with other types of hepatectomy. In our series the 11 cases were divided into two subgroups: laparoscopic isolated caudate hepatectomy (LICH) (n = 4) and laparoscopic combined caudate and left hemihepatectomy (LCLH) (n = 7). All cases were performed by our minimally invasive team. All senior surgeons had more than 10 years' surgical experience.
This study was approved by the ethics committee of Sir Run Run Shaw Hospital, Zhejiang University, Hangzhou, China. Patient information was anonymized and de-identified prior to analysis.
Anatomy and surgical procedure
The caudate lobe of the liver is located between the hepatic hilum and the inferior vena cava (IVC). It can be divided into three parts: Spiegel's lobe (Couinaud's segment 1), the paracaval portion (Couinaud's segment 9), and the caudate process.10,11 The caudate lobe is supplied by arterial branches and portal vein branches from both the left and right portal triads. For the purpose of surgical anatomy, there are usually two to five large trunks emanating from the portal triads to the caudate lobe, called the caudate portal triad. 12 The caudate lobe drains directly into the IVC through a series of short hepatic veins and not usually into the left, middle, or right hepatic veins (Fig. 1). The transection line can become problematic during complete isolated caudate lobectomy. Theoretically it can be defined using the counterstaining identification technique described by Takayama et al. 13 in 1991. In practice, we transect the liver parenchyma from the caudate process to the tip of the caudate lobe along the oblique plane slanting from the right portal vein to the left hepatic vein.
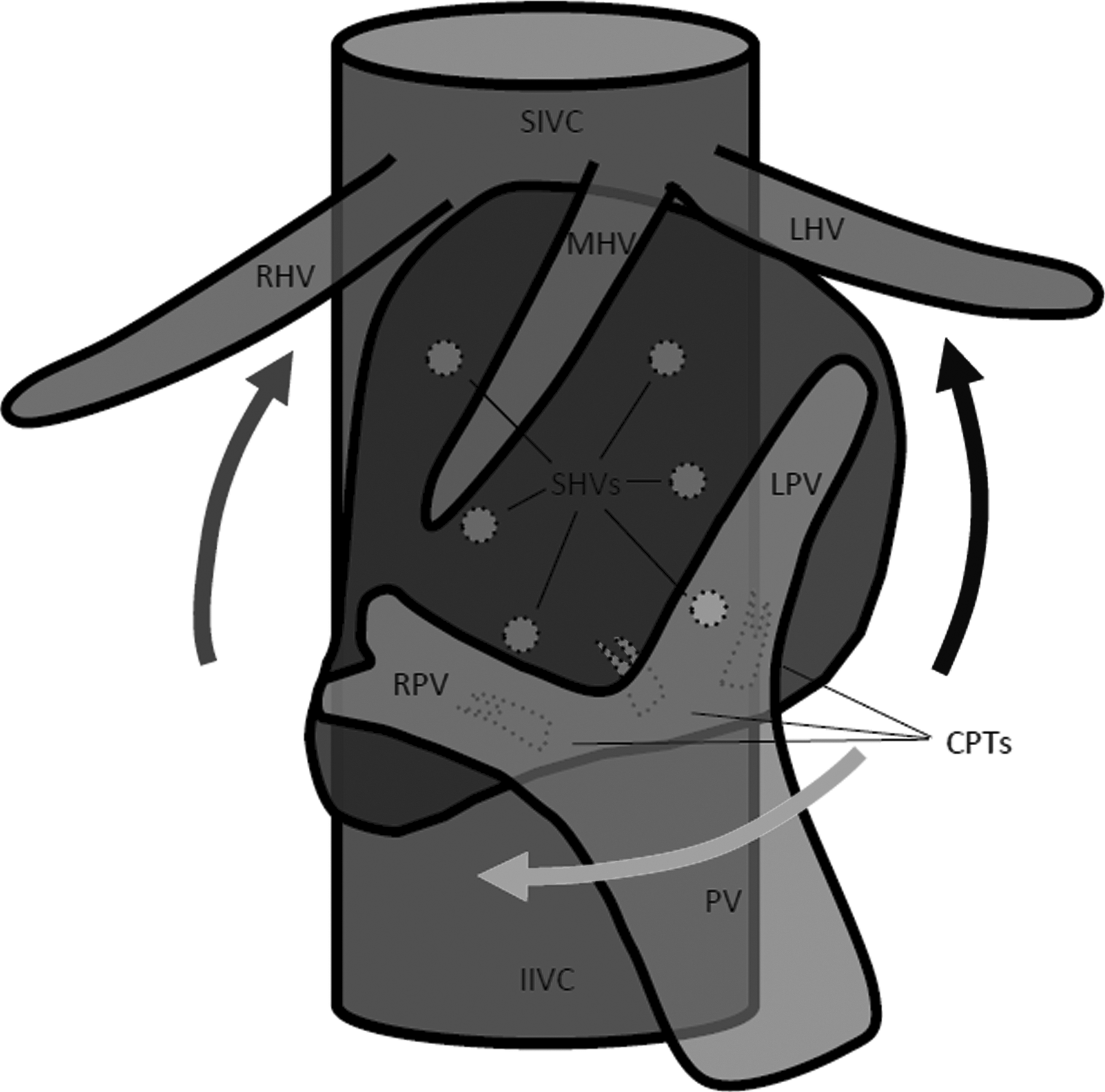
Anatomy of the caudate lobe and the major surgical processes of caudate hepatectomy. The black arrow indicates a left approach to divide the short hepatic veins (SHVs) and raise the caudate lobe. The light gray arrow indicates the caudate portal triads (CPTs) are dissected and divided. The dark gray arrow indicates the caudate lobe is transected from the caudate process to the tip of the caudate lobe (from the right portal vein [RPV] to the left portal vein [LPV]). IIVC, inferior inferior vena cava; LHV, left hepatic vein; MHV, middle hepatic vein; PV, portal vein; RHV, right hepatic vein; SIVC, superior inferior vena cava.
LCH was performed by a left-sided, purely laparoscopic approach. Patients were positioned supine under general anesthesia. Maintenance of a low central venous pressure (less than 5 mm Hg) was used. Three surgeons performed the operation. The senior surgeon stood on the left side of the patient with a junior surgeon on his right near the head of the patient; the assistant was on the right side of the patient. Four trocar sites were used. Pneumoperitoneum (12 mm Hg) was established, and a supraumbilical 10-mm trocar was inserted as the camera port. A 12-mm trocar below the left costal margin was placed for the main manipulation port, and two 5-mm assisting ports were inserted in the right flank area under direct vision (Fig. 2).

Placement of trocars and surgeons' position when performing LCH: point A, observation port; point B, main manipulation port; and point C, two assistant ports and the incision for removing the specimen.
The patient was turned to a 30° anti-Trendelenburg position. The peritoneal cavity was explored for extrahepatic disease. After division of the falciform, left coronary, and triangular ligaments, the left lobe of the liver was lifted anteriorly. The lesser omentum was incised, and if present the accessory left hepatic artery was preserved. After the Spiegel process was exposed, routine intraoperative ultrasonography was performed to identify the tumor's location, to evaluate its relationship to the vessels, and to determine if unexpected tumors were present.
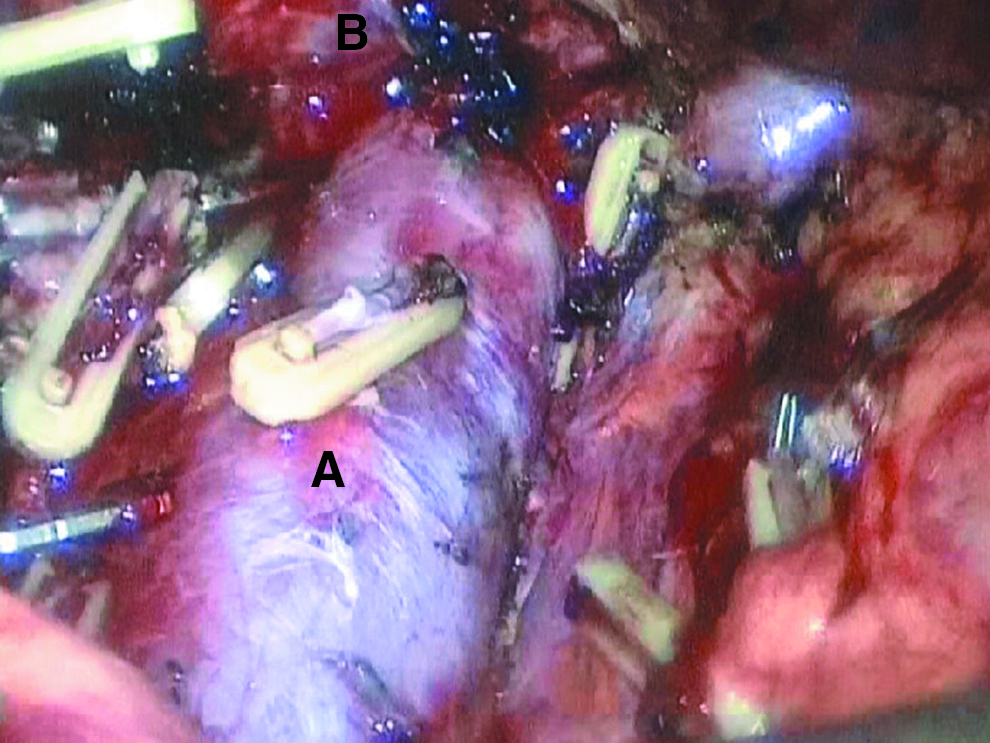
The three major steps for caudate hepatectomy are shown in Figure 1. In the first step, the peritoneum and fibrous attachments between the caudate lobe and the IVC were divided. The short hepatic veins were clamped and divided with a titanium ligating clip (Ethicon Endo-Surgery Inc., Cincinnati, OH) or an absorbable clip (12-mm Lopro-Clip; Tyco Healthcare UK Ltd., Gosport, United Kingdom) (Fig. 3). In the second step, the assistant lifted the caudate lobe and pulled it to the left. The branches to the caudate lobe, the caudate portal triads, were dissected and divided one at a time, close to the base of the umbilical fissure (Fig. 4). In the third step, after the caudate lobe was released from the IVC and hepatic hilum, we transected the liver parenchyma from the caudate process to the tip of the caudate lobe. Parenchymal transection was performed by a laparoscopic Peng's multifunction operative dissector (Hangzhou Shuyou Electronic Science and Technology Co. Ltd., Hangzhou) using the curettage and aspiration technique (Fig. 5). We have previously reported our experience of laparoscopic liver resection using the laparoscopic Peng's multifunctional operative dissector. 14
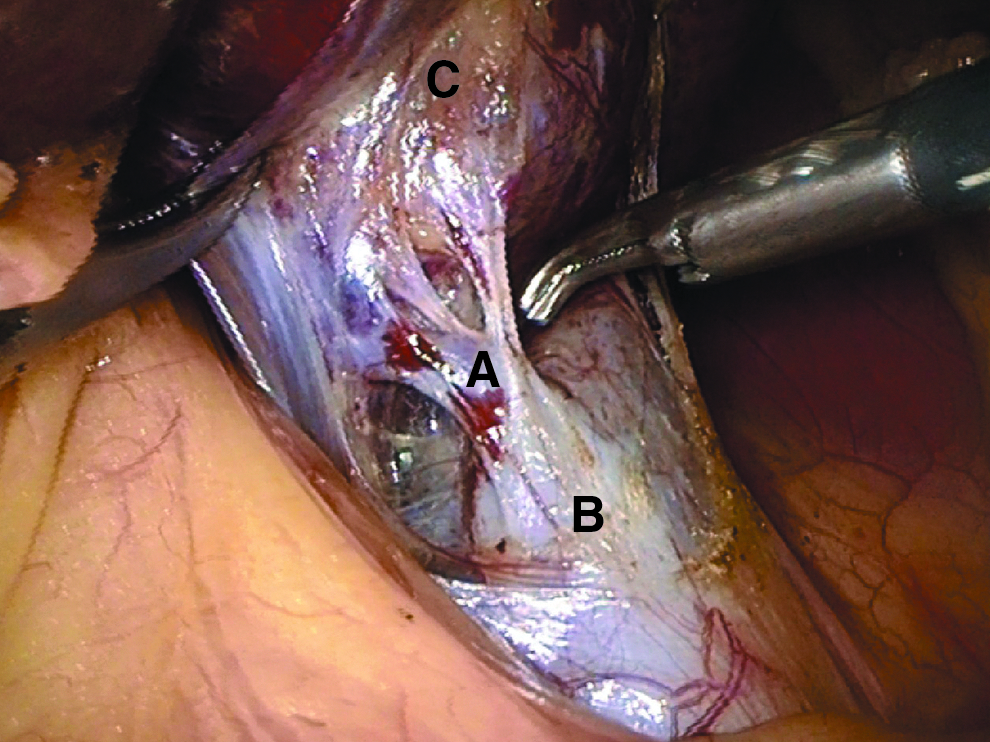
A short hepatic vein was isolated. A, a large short hepatic vein; B, inferior vena cava; C, the caudate lobe.
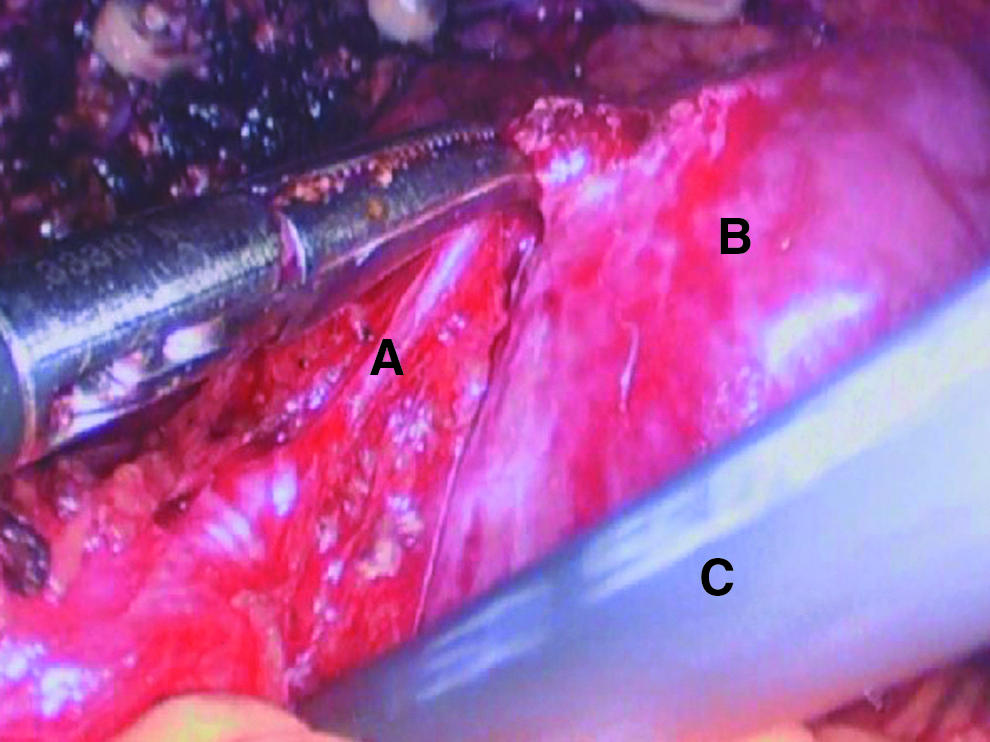
A caudate portal triad is dissected. A, a caudate portal triad; B, the caudate lobe; C, laparoscopic Peng's multifunction operative dissector.
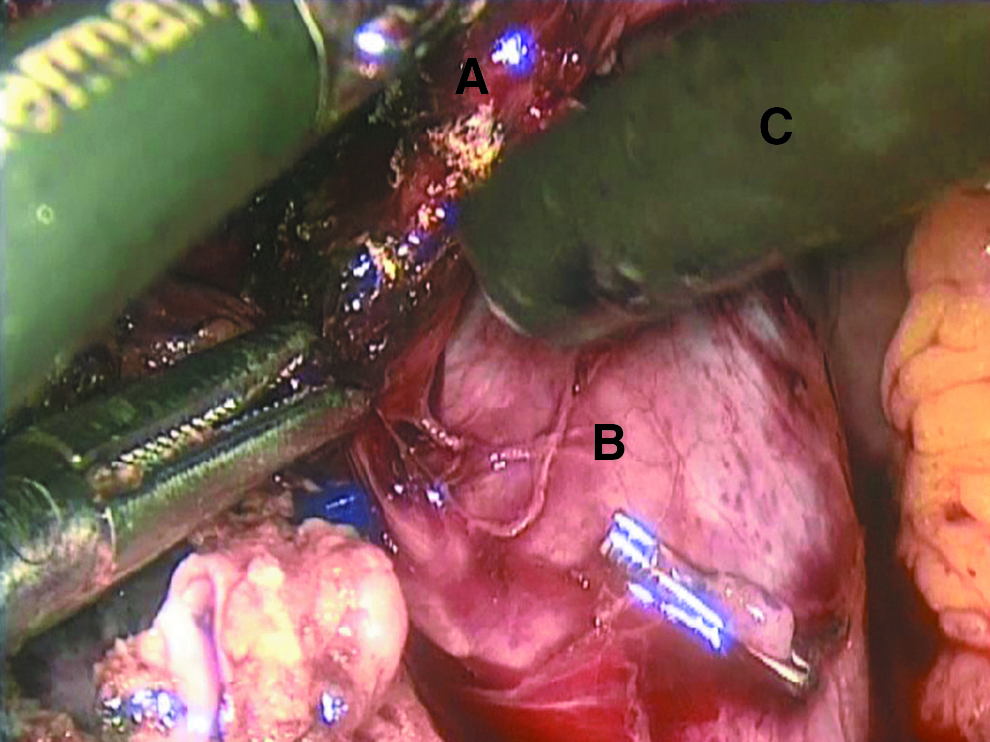
Parenchymal transection was performed by the laparoscopic Peng's multifunction operative dissector. A, the caudate lobe; B, inferior vena cava; C, laparoscopic Peng's multifunction operative dissector.
After the caudate lobe was removed, the retrohepatic IVC was exposed (Fig. 6). The specimen was retrieved in a bag and extracted via an extended assisting trocar site. We did not use Pringle's maneuver in the laparoscopic process. In the LCLH group, left hemihepatectomy was performed first to obtain better exposure for LCH. Laparoscopic left hemihepatectomy by curettage and aspiration was performed as described previously. 9 A drain was placed near the resection site in each case.
The retrohepatic inferior vena cava was exposed after the caudate lobe resection. A, inferior vena cava; B, left hepatic vein.
Statistical analysis
Patient characteristics, surgical features, and postoperative course were analyzed according to type of resection. Complications were graded according to the Clavien–Dindo classification. 15 Posthepatectomy liver failure was defined and graded according to the International Study Group of Liver Surgery. 16 Results were expressed as median (range) values.
Results
Demographics
In our series 11 patients (four males, seven females; 34–60 years of age) underwent laparoscopic caudate lobectomy (four LICH, seven LCLH). Diagnoses of patients undergoing LICH included hepatocellular carcinoma (n = 1), colorectal metastases (n = 1), and symptomatic hemangioma (n = 2). Diagnoses in the LCLH group included hepatolithiasis (n = 5), hepatocellular carcinoma (n = 1), and symptomatic hemangioma (n = 1).
Surgical features
Conversion to open surgery was required for 2 patients (one hemangioma in the LICH group and one hepatolithiasis in the LCLH group). Only 1 patient in the LCLH group who required conversion required blood transfusion (9.1%). Operation time was 185 (range, 155–350) minutes in the LICH group and 275 (range, 190–295) minutes in the LCLH group. The blood loss was 250 (range, 200–600) mL in the LICH group and 500 (range, 300–900) mL in the LCLH group, respectively.
Resection margin is an important factor associated with clinical outcome. Surgical margins were negative in all cases with tumors. In the LICH group, the tumor size was 11.8 (range, 1.2–20) cm3, and the resection margin was 1.4 (range, 0.4–2) cm.
Postoperative course
The length of postoperative hospital stay was 7 (range, 4–11) days in the LICH group and 6 (range, 5–9) days in the LCLH group. Three of 11 patients (27.3%) required postoperative analgesia, including 2 patients who underwent conversion.
No mortality occurred in the perioperative period. Two patients experienced two complications. The patient who underwent conversion in the LICH group experienced temporary respiratory distress and a pleural effusion and recovered without intervention (Clavien Grade I). One patient with hepatolithiasis in the LCLH group was treated with antibiotics for an intraabdominal infection (Clavien Grade II). No cases of postoperative bleeding, biliary leakage, or liver failure occurred. Intraoperative cholangiography was routinely performed in patients with hepatolithiasis. No residual stone was found in any of 5 cases.
Discussion
Among laparoscopic hepatectomy surgeries, LCH is the most difficult procedure for which limited reports have been published.17–26 As far as we know, we present the largest series of laparoscopic caudate lobe resection using a left-sided, purely laparoscopic approach. Our experience shows that LCH can be applied in selected patients with hepatocellular carcinoma, colorectal metastasis, hemangioma, or hepatolithiasis.
For caudate hepatectomy, the laparoscopic approach is a double-edged sword. On the one hand, minimally invasive liver resection can improve patient outcomes by reducing blood loss, postoperative pain, and hospital length of stay.8,27,28 On the other hand, this difficult procedure may bring danger to the patient during surgery. Strict inclusion criteria and exclusion criteria, abundant experience in laparoscopic liver resection, and appropriate surgical technique dictate the success of this procedure.
In our opinion, caudate lobe tumors larger than 5 cm or with vascular invasion cannot be managed safely under laparoscopy. Hilar cholangiocarcinoma is also not appropriate for LCH, as we cannot guarantee safe surgical margins and effective lymphadenectomy. One cirrhotic patient and 1 patient with hepatic fibrosis underwent successful laparoscopic resection and recovered well. This supports previous data that cirrhosis and fibrosis are not contraindications for laparoscopic liver resection.8,29,30 Even with the success of laparoscopic resection for benign disease demonstrated in this study, we do not believe that indications for resection can be liberalized. We do not perform operations for asymptomatic benign tumors.
As is known, surgeons experience a learning curve before mastering laparoscopic liver resection.14,31 Since the first case was performed in August 1998, we have completed more than 100 cases of laparoscopic liver resection before performing the challenging laparoscopic hepatic caudate lobectomy. We suggest that the technique of laparoscopic hepatectomy should develop step by step in an institution, from simple to complex cases. In our hospital we use the laparoscopic approach while following patient safety and oncologic principles.
Certain techniques are used during laparoscopic caudate lobectomy, including different approaches, low central venous pressure, different instruments, and intermittent pedicle clamping. Three approaches have been described: left, right, and transparenchymal.32,33 In our experience the left-sided approach is a rational procedure, especially for patients whose lesions arise from Spiegel's lobe or spread into the left part of the caudate lobe. Low central venous pressure (less than 5 mm Hg) was used, which can reduce intraoperative bleeding.34,35 We used the laparoscopic Peng's multifunctional operative dissector as the main surgical instrument. This instrument can be used for blunt dissection, aspiration, cutting, and electric coagulation without replacing instruments. It maintains a clear line of vision and saves time. The intrahepatic ducts and vessels can be bluntly dissected using the curettage and aspiration technique. Parenchymal transection can be completed in experienced hands. After the inflow and outflow of the caudate lobe were controlled, we did not find Pringle's maneuver or preventative hepatic vein isolation to be necessary in our patients. The most dangerous maneuver is parenchymal transection, where the main hepatic veins are near to the dissection plane. We do not emphasize the exposure of hepatic veins, which may cause unmanageable bleeding. Air embolism is another potential problem. We prevented gas embolism by controlling the pneumoperitoneum pressure below 12 mm Hg and ligating short hepatic veins before liver resection.
In our series there were 2 patients who required conversion to open surgery (18.2%). One hemangioma patient in the LICH group was converted to open surgery due to bleeding from an short hepatic vein. In another patient with hepatolithiasis in the LCLH group, bleeding was encountered during dissection of the caudate portal triads. The most common reason for conversion to open surgery is bleeding, both here and in other studies. 24 Conversion from laparoscopic to open surgery should not be considered a failure. Conversion to open surgery should be expedited if bleeding cannot be controlled laparoscopically. We have an experienced team composed of surgeons, anesthesiologists, and nurses to ensure patient safety. We use the sponge press method under laparoscopy to temporarily control bleeding. Blind suturing may cause massive, fatal hemorrhage with tearing of veins.
There were no serious complications (such as bleeding, biliary leakage, and liver failure) in our series. This may be due to clearer visualization and meticulous dissection of liver parenchyma under laparoscopy. Biliary leakage is the most common and disturbing postoperative complication in liver resection and can cause sepsis, liver failure, and death.24,36 Further studies should be performed to evaluate the value of the laparoscopic technique for reducing biliary leakage.
A safe resection margin needs to be emphasized in patients undergoing laparoscopic caudate lobe resection. Some studies showed that wedge resection had a higher positive margin rate than anatomic resection.37,38 In our series all patients underwent anatomic liver resection, instead of enucleation, even for benign tumors. Our experience showed that a safe resection margin can be attained in selected patients undergoing anatomic LCH.
For patients with hepatolithiasis, residual stone rate is an important indicator of treatment outcome. In our study the initial clearance rate was 100% in 5 cases with hepatolithiasis. This result is comparable to previous reports and indicates that LCH can be used to treat cholelithiasis of the caudate lobe.39–42
Our experience has provided a strategy for selecting appropriate patients, a systematic technical method, and a preliminary safety and feasibility evaluation of LCH. However, our patient population is small, and it consists of heterogeneous subgroups. In consideration of those limitations, further studies should be performed to validate the safety and benefits of LCH. In the meantime, the technologies and methods will continue to advance.
Conclusions
Laparoscopic caudate resection is technically challenging due to the special location of this lobe. According to our experience, a left-sided, purely laparoscopic approach for anatomic caudate hepatectomy can be performed safely by experienced laparoscopic hepatobiliary surgeons in selected patients.
Footnotes
Disclosure Statement
No competing financial interests exist.