
Abstract
Abstract
Introduction:
Thoracoscopic surgical procedures in small infants and children require a growing demand for lung isolation in pediatric anesthesia practice.
Materials and Methods:
Between January 2006 and September 2014, 16 children underwent thoracoscopic procedures that needed one-lung ventilation using a bronchial blocker.
Results:
The thoracoscopic procedure was performed at a mean age of 99 months (range, 6–186 months) and a mean weight of 33 kg (range, 7–68 kg) without any conversion to open surgery in any case. We were able to achieve one-lung ventilation in all patients. The quality of lung deflation was excellent in all patients except in 1 due to malposition of the bronchial blocker, whereas dislodgement of this device occurred in 2 cases.
Conclusions:
The use of a bronchial blocker provided a highly effective means of one-lung ventilation for children undergoing the thoracoscopic approach.
Introduction
I
The pulmonary ventilation might jeopardize the success of VATS with an insufficient surgical exposure increasing the rate of conversion to open surgery. Historically, VATS was considered to be an absolute indication for OLV to provide surgical exposure in adult patients, 3 but its application in infants and children has not been universally determined yet. OLV has been postulated to be absolutely indicated when the nondiseased lung must be protected from ipsilateral lung pathology, such as hemorrhage, infection, or spillage of tumor cells. Many other indications for lung isolation in children exist, including tumor resection, lobectomy, repair of coarctation of the aorta, and spinal access in pediatric scoliosis. Even if the former procedures were not technically difficult, they had several shortcomings, such as the incomplete collapse of the operating lung, contamination from the affected lung to the healthy lung, difficulties in suctioning the lung during surgery, and the possibility of obstruction of the upper lobe bronchus (especially the right upper lobe bronchus). 4
Currently, many techniques for OLV exist, including the use of a single-lumen endotracheal tube, double-lumen tubes, Univent® (Fuji Systems, Tokyo, Japan) tubes, and bronchial blockers (BBs) such as the Fogarty embolectomy catheter or the Arndt® endobronchial blocker (Cook Critical Care, Bloomington, IN). These options have their individual limitations, and none is entirely satisfactory because available equipment may be too large and poorly adaptable in small children or in patients with abnormal upper or lower airways. 5 The choice of OLV techniques depends on multiple factors, including the age, the size, and the anatomy of the patient, the training of the anesthesiologist, the availability of equipment, and the type of surgery.
The new BBs have advantageous properties such as a high-volume, low-pressure balloon and a multiport airway adapter. These features allow them a broad pediatric application. 6 In the recent literature, there are a very few isolated cases about the use of these devices during pediatric thoracoscopy. We report here our experience of single-lung ventilation by BBs in a large series of children affected by different thoracic pathologies.
Materials and Methods
Between January 2006 and September 2014, 16 children (7 females and 9 males) underwent thoracoscopic procedures that required OLV (Table 1). The indication for a BB in order to optimize the exposure or to avoid contamination of the nondiseased lung during surgery was judged after an accurate radiological study that provided in some cases the three-dimensional thoracic reconstruction of the bronchial tree. All patients received general anesthesia and were subjected to insertion of a standard tracheal tube ranging in diameter from 4.5 to 7.0 mm into the trachea. In all cases fiber optic bronchoscopy was performed, allowing the visualization of any anatomical abnormalities of the bronchial tree and the placement of the endobronchial blocker.
BB, bronchial blocker; CCAM, congenital cystic adenomatoid malformation; ELS, extralobar sequetration; F, female; ILS, intralobar sequestration; M, male; PAIR, puncture, aspiration, injection of a scolecidal agent, re-aspiration; TT, tracheal tube.
The pediatric BB was inserted into either the right or the left main bronchus to block ventilation to either the right or the left lung, depending on the site of surgery. In each case, the blocker and the fiber optic scope were placed through their respective ports of a Y-shaped adapter and driven under videoscopic guidance into the desired main bronchus. Then the balloon was inflated. Lung isolation and proper positioning were confirmed by auscultation and direct visualization of the blocker. All patients were subjected to a thoracoscopic procedure with a CO2 insufflation pressure of 4–6 mm Hg and a flux of 1.5–2 L/minute.
We also identified two subgroups according their age less than (Group A) or greater than (Group B) 2 years in order to look for differences that might affect the use of endobronchial blockers in our pediatric population. Mean values were compared using the unpaired Mann–Whitney test, and qualitative parameters were analyzed by Fisher's test. A P value < .05 was considered statistically significant.
Results
The thoracoscopic procedure was performed on the patients at a mean age of 99 months (range, 6–186 months) and a mean weight of 33 kg (range, 7–68 kg) without any conversion to open surgery in any case. The indications for thoracoscopic surgery and lung isolation were resection of bronchopulmonary lesions in 10 patients (63%) and scoliosis or hyperkyphosis in the others (Table 1). Seven (44%) BBs were placed in the left main bronchus, and nine (56%) were placed in the right. Placement of a BB required a mean time of 18.8 minutes (range, 10–25 minutes) with an operating time of 69 minutes (range, 15–145 minutes). We were able to achieve OLV in all patients. Group A included 7 patients with a median age of 13.3 months (range, 6–24 months) and a median weight of 9.2 kg (range, 7–12.5 kg), whereas Group B included 9 patients with a median age of 165 months (range, 84–106 months) and a median weight of 51.7 kg (range, 26–68 kg). Even if the weight difference between the two groups was statistically significant at P > .0002, allowing coverage of the entire spectrum of pediatric population, the difference in the application time of endobronchial blockers was not statistically significant between the two groups (P = .2105) (Fig. 1).
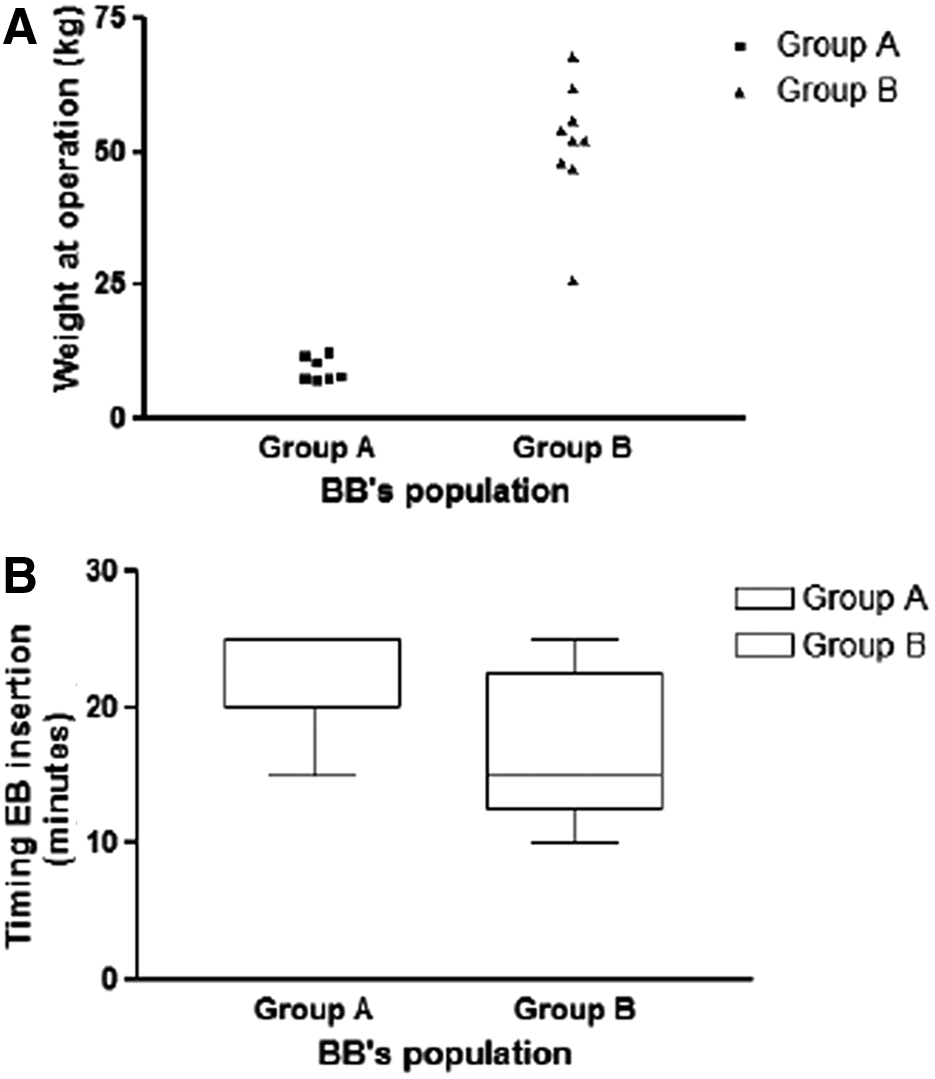
Statistical analysis of two patient subgroups according their age as less than (Group A) or greater than (Group B) 2 years by
In all cases there was no deterioration in the heart rate or mean arterial pressure during OLV. The quality of lung deflation was judged to be excellent in all patients except in 1 (Patient 2 in Table 1) in whom the malposition of the BB had excluded only the inferior lobe with hyperinflation of the middle lobe and consequent difficulty in the dissection of this lobe. In 1 case (Patient 4 in Table 1) during the manipulation of the tracheobronchial tree, the blocker became dislodged into the trachea. This malpositioning caused an immediate increase in peak inspiratory pressure, which was resolved quickly by a simple advance of the BB under endoscopic guidance into a main bronchus. In another case (Patient 7 in Table 1) the sliding of the BB from its initial position created an obstacle at the level of the superior left lobe that proved to be optimal for the dissection. Even though all complications were found in patients of Group A, there was no significant difference between the two groups.
At the end of the thoracoscopic procedure, the surgeon requested re-expansion of the collapsed lung to ensure complete expansion of the entire lung parenchyma under thoracoscopic vision. No airway trauma was described in any patient during insertion or use and inspection of the bronchial walls after BB removal.
Discussion
The increased use of thoracoscopic surgical procedures in small infants and children, due to prenatal diagnosis for congenital bronchopulmonary malformations, requires an increasing experience for lung isolation in pediatric anesthesia practice. OLV during thoracoscopy is recommended to create an adequate space for visualization, exposure, and dissection while oxygenation is maintained. 7 For the surgeon, there are several advantages to using OLV. The operative lung remains collapsed and calm, thereby optimizing surgical exposure and enabling adequate “working space” in a relatively small anatomic compartment. In our cases it was particularly helpful for lesions such as congenital cystic adenomatoid malformation that may be collapsed, piercing it in several places. Lung isolation will also facilitate demarcation of normal parenchyma from the abnormal tissue in cases where incomplete fissures between the lobes make this differentiation difficult. In the 2 cases of giant lobar emphysema, OLV helped us to minimize overdistension of the pathologic lobe. Also, in the presence of an abscess cavity or a hydatid cyst, the selectively blocking of the bronchus of the affected lung prevented the contamination of the bronchial tree during manipulation of the diseased lung. In our series lung isolation by BBs has found wide application in the cases of spine curvature disorders in which collapsing the lung for several hours of surgery is required.
Rothenberg 8 postulated that most children tolerate OLV without significant respiratory compromise during major thoracoscopic procedures. Lung isolation in infants and young children can be technically challenging. Techniques and equipment commonly used in adults, such as double-lumen endobronchial tubes or the Univent tube, have not been available for the pediatric population. The simplest technique of lung isolation is to push an endotracheal tube into an endobronchial position, with or without bronchoscopic guidance. Even if a small, uncuffed endotracheal tube is used, it may be difficult to obtain a perfect seal, allowing some ventilation of the operative lung and imperfect protection of the healthy lung from contamination. Another disadvantage of mainstem intubation is the inability to temporarily re-inflate and subsequently re-isolate the operative lung. This may be required to improve oxygenation, to facilitate the surgeon's ability to distinguish normal from pathologic tissue, or to identify a bronchial leaks. Because of the unavailability of double-lumen endobronchial tubes for use in young children, the BB represents a valid alternative and the technique of choice in pediatric patients under the age of 6 years. 4
Over the years various BBs have been designed and used according to their purpose. In 1969, Vale 9 already described use of the Fogarty embolectomy catheter for lung isolation in small children and suggested appropriate size selection for this age group. Tan and Tan-Kendrick 10 measured right and left bronchi of 250 children 2 days to 16 years of age using computed tomography of the thorax and correlated the value with the patient's age and weight, in order to create a guide to size selection of the Fogarty catheter. From this study, they found out that the age, but not the weight, of the patient is a good predictor of the main bronchial diameters. 10 Even if widely used, the Fogarty is a vascular embolectomy closed-end catheter not designed to function as a BB.
The recent renewed interest for these devices has led to the development of several new designs and an appreciation of characteristics of the ideal BB, which should include a balloon shape for stabilizing in the bronchus, high pressure, low volume, flexibility, a channel for deflation and suction distal to the blocker, adaptable for use to internal and external to a standard tracheal tube, and a wide variety of size. Recently a BB with most of these requirements is the Arndt, which was shown to provide highly effective single-lung isolation and ventilation in pediatric thoracic surgery. 6
Several complications related to the use of a BB have been reported over the past 10 years, such as avulsion of the BB cuff in the trachea 11 and accidental fracture of the tip of the bronchial blocker. 12 Displacement of the BB can lead to ventilation problems and even cardiac arrest. 13 Finally, entrapment of the BB catheter by a surgical stapler has been reported. 14 In our series we had 2 cases of dislodgement involving the left mainstem bronchus during the manipulation of the bronchial tree.
Bauer et al. 15 compared lung isolation with left-sided double-lumen tubes, left BBs, and right BBs. Left BBs took longer to be placed than double-lumen tubes or right-sided blockers and had to be placed as far distally in the bronchus as possible because they tend to migrate proximally, but the lung deflation was better in the left blocker than in the right blocker cases. We also showed in our series how the time of the BB's insertion and the outcome of OLV are not significantly affected by the difference of age, and so this should be able to stimulate a wider use.
In conclusion, the use of the BB in our series provided a useful and highly effective means of OLV for children undergoing the thoracoscopic approach. This is an extremely versatile technique that requires experience with these devices to avoid any risks, but also represents a continuous stimulus to improve the armamentarium of the pediatric thoracic anesthesiologist.
Footnotes
Disclosure Statement
No competing financial interests exist.