
Abstract
Abstract
Objective:
To evaluate a modified laparoscopic transabdominal cervicoisthmic cerclage (LTCC) technique after failure of transvaginal cerclage during pregnancy in women with cervical weakness.
Materials and Methods:
Eighty women in whom transvaginal cerclage was unsuccessful or who were anatomically unsuitable for the procedure underwent modified LTCC between January 2003 and December 2008 at Keimyung University, Dongsan Medical Center, Daegu, South Korea. The modified LTCC was performed using a polyfilament polyester double-armed needle that was sutured laterally to the uterine vessels at the level of the internal cervical os. Survival of the fetus was used to calculate the successful pregnancy rate of this modified LTCC. The relationship between successful pregnancy rate and clinical variables was evaluated using a chi-squared test and a Mann–Whitney U test.
Results:
The mean gestational age was 12.1 weeks (range, 11–15 weeks). The operation time was 52 minutes (range, 25–100 minutes). The successful pregnancy rate was 90% (72/80 pregnancies), with a mean gestational age of 36.3±2.7 weeks. The mean newborn weight was 2690 g (range, 1860–3750 g). Eight pregnancies were lost in the first and second trimesters due to spontaneous abortion, premature rupture of the membrane, and termination due to anomaly; no other complications occurred. No statistical difference was found between the successful pregnancy rate and the measured clinical variables.
Conclusions:
The modified LTCC is feasible and safer than traditional LTCC.
Introduction
C
The transabdominal approach to cerclage placement above the cervix and around the uterine isthmus was originally described by Benson and Durfee 5 in 1965. Subsequently, improved outcomes have been extensively reported with fetal survival rates approaching 90%.5–7
However, one disadvantage to the transabdominal approach is the need for two open laparotomies: one for cerclage and one for cesarean section. Postoperative bowel adhesion is another problem associated with the open method. However, using laparoscopic transabdominal cervicoisthmic cerclage (LTCC) allows the patients to avoid these side effects and complicating factors. Patients experience considerable benefit from a rapid recovery, reduced pain, and the avoidance of two open laparotomies through this minimally invasive procedure. 8
LTCC has been used since 1996 and was first performed during pregnancy. The results of LTCC are as good as with the abdominal approach. 9 We reported in 2003 that LTCC during pregnancy is a safe and effective treatment for women with cervical weakness.
However, some challenges exist when LTCC is performed by the traditional method, including difficulty with manipulating the uterus and increased bleeding risk due to the high vascularization of the area close to the ureters and parametrial veins. These risks lead to an increase in operation time and morbidity. Therefore, we developed an easier, modified method for LTCC in which the sutures for the cervical cerclages are lateral to the uterine vessels. Our findings describe 80 patients who underwent this modified LTCC and present data suggesting that modified LTCC is feasible and easier than traditional LTCC.
Materials and Methods
A prospective observational cohort study was conducted from January 2003 to December 2008 at Keimyung University, Dongsan Medical Center, Daegu, South Korea, with institutional ethics board approval (protocol number 07–26). Eighty women in whom transvaginal cerclage was unsuccessful or unsuitable underwent modified LTCC and were followed up for 6 years. None of the women had histories of congenital anomalies or diethylstilbestrol exposure. Thirty women had marked scarring after failed vaginal cerclage; of the other 50 women in the study, 30 had at least one or two successive second-trimester pregnancy losses. All patients had severe cervical deformities, including short cervixes due to extensive conization and deep forniceal lacerations (Table 1). Preoperatively, endocervical swabs for Chlamydia and Mycoplasma were obtained to ensure that patients did not have cervical infections. Fetal viability was confirmed by ultrasonography. Before surgery, none of the patients had experienced abnormal uterine contractility, ruptured membranes, or uterine bleeding. Extensive counseling was provided regarding the risks and benefits of the procedure.
Modified LTCC was performed at a mean gestational age of 12 weeks (range, 11–15 weeks). One surgeon performed all procedures. After fetal viability was confirmed, the procedure was performed with the patient under combined general and spinal anesthesia to reduce the amount of inhalation anesthetics used during the operation. Patients were placed in the dorsal lithotomy position.
Surgical procedure
A Veress needle was carefully inserted through the umbilicus, and CO2 was insufflated into the peritoneal cavity to obtain a pneumoperitoneum. The laparoscope was then introduced through a laparoscopic trocar at the umbilical incision or at a high level of the umbilicus. An 11-mm port was introduced under visualization in the left lower quadrant, and two additional 5-mm trocars were introduced in the right lower quadrant and suprapubic lesion. Intraabdominal pressure of 12 mm Hg was maintained; a uterine manipulator was not used.
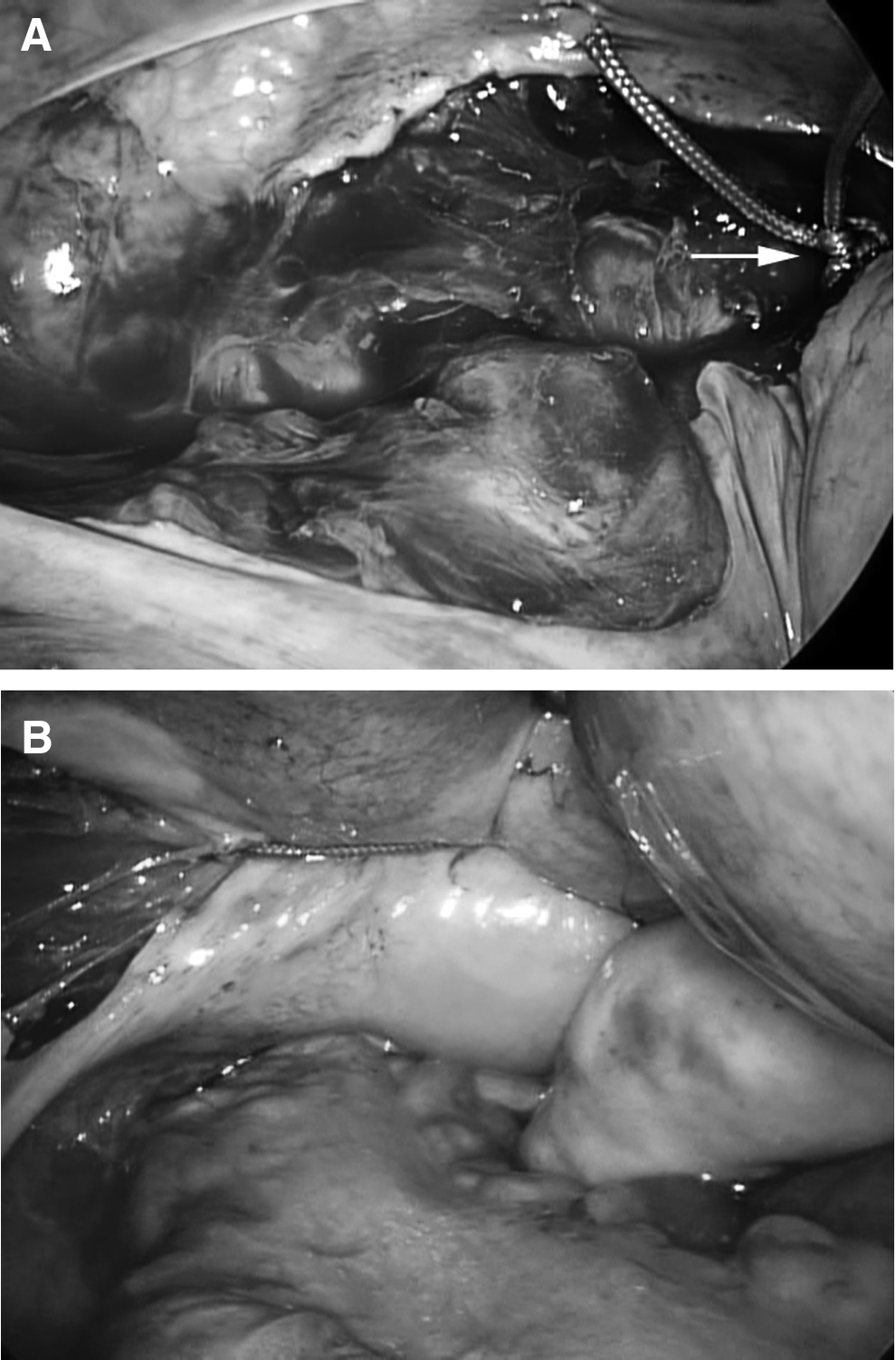
The vesicouterine peritoneum was dissected transversely with laparoscopic scissors, and the bladder was advanced downward to provide an anterior visualization of the course of the uterine arteries. After identification of both ureters (Fig. 1A), the posterior leaves of the broad ligament near the uterine vessels were carefully dissected (Fig. 1B). The uterine arteries and bifurcation of the ascending branch were identified. A polyfilament polyester (Dagrofil®; B-Braun, Melsungen, Germany) double-armed needle, 75 cm in length was prepared. After the uterine vessels were identified posteriorly, each end of the needle was inserted laterally to the uterine vessels (Fig. 1C and 1D). This was done using a posterior-to-anterior method at the level of the uterine isthmus above the uterosacral ligament, bringing both ends of the thread anterior to the uterine isthmus. Both ends of Dagrofil were tied extracorporeally in a snug fashion and reinserted with a knot pusher. The Dagrofil was then secured on the anterior aspect of the cervix with a triple square knot. The suture placement with this procedure sits at the level of the internal cervical os, above the uterosacral ligaments, with the knot at the anterior aspect of the uterus (Fig. 2). The difference between this modified LTCC and the traditional LTCC is that tape is inserted laterally to the uterine vessels and above the ureters at the level of the uterine isthmus, above the uterosacral ligament.

No tocolytics were administered to the patient either during or immediately after the procedure. Perioperative antibiotics were administered on the day of the procedure. The patient was observed in the hospital room for 2–3 days until she was comfortable.
Transvaginal ultrasonography was performed 2 weeks after discharge to confirm proper cerclage placement. Following ultrasonography, patients were managed through regular follow-up by a specialized obstetric team.
To evaluate the possibility of intrauterine growth restriction, we compared the systolic–diastolic (S/D) ratio in the umbilical artery Doppler velocimetry scan between this modified LTCC group and a normal age-matched control group between 30 and 34 gestational weeks. The control group consisted of healthy normal pregnant women who had no factors related to high-risk pregnancies (e.g., preeclampsia, gestational diabetes mellitus, and other risk factors).
Statistical analysis
Statistical analyses were performed with SPSS statistical software (version 20.0; IBM SPSS, Inc., Chicago, IL). The relationship between successful pregnancy rate and clinical variables such as age, history of delivery, history of transvaginal cerclage, and gestational age was evaluated using a chi-squared or Fisher's exact test and a Mann–Whitney U test. Values of P<.05 were considered statistically significant, and all P values correspond to two-sided significance tests.
Results
Eighty patients underwent modified LTCC during the study period; patient demographics are presented in Table 1, and a summary of our cases is presented in Table 2. The average operation time of the modified LTCC was 52 minutes, the average estimated blood loss during the procedure was less than 100 mL, and no perioperative or postoperative complications occurred. The mean gestational age was 12.1 (range, 11–15) weeks. The overall pregnancy survival rate was 90% as defined by the number of live births per total number of pregnancies recorded; details of the pregnancy outcomes are presented in Table 3. The mean gestational age at delivery if the pregnancy continued past viability was 36.3±2.7 weeks (range, 26.0–39.3 weeks); mean birth weight was 2690 g.
Data are mean (range) values.
LTCC, laparoscopic transabdominal cervicoisthmic cerclage.
Data are number of patients, mean (range) values, or number (%) as indicated.
LTCC, laparoscopic transabdominal cervicoisthmic cerclage; NICU, neonatal intensive care unit.
Details of the various clinical presentations are presented in Table 3; two failures were in the second trimester and attributed to the clinical consequences of preterm labor or premature rupture of the membrane that occurred in patients with a history of recurrent second trimester pregnancy loss. The fetus and products of conception were successfully removed by dilatation and curettage after removing the tape by laparoscopy. Six of the failed pregnancies were aborted in the first trimester (2 patients terminated due to fetal anomaly); all cases were managed by dilatation and curettage through the cerclage.
Seventy-two patients successfully delivered 76 live newborn infants (four sets of twins) by cesarean delivery. The cerclage band was left in situ in all patients. Eleven patients have had a second term pregnancy (>37 weeks) with the same cerclage in situ.
Nineteen of the 72 patients delivered between 26 weeks and 37 weeks because of a premature rupture of the membrane, severe pregnancy-induced hypertension, or premature labor. Thirteen newborn infants were admitted to the neonatal intensive care unit, but no other long-term sequelae of prematurity were reported. The smallest newborn in this group weighed 1860 g at birth. During the course of the pregnancies, 10 women were admitted before 34 gestational weeks for observation on suspicion of uterine contractions. Some of these patients were briefly treated with intravenous tocolytics. The total successful pregnancy rate was 90%. No statistical difference was found between successful pregnancy rate and clinical variables. Successful pregnancy rate was not related with clinical variables including age, history of delivery, number of abortion, gestational weeks at operation, and operation time (Table 4).
LTCC, laparoscopic transabdominal cervicoisthmic cerclage.
Because this modified LTCC uses a thread inserted laterally to the uterine vessels, we were concerned about the effects of fetal growth. Therefore, we compared the S/D ratio between the modified LTCC group and a normal control group between 30 and 34 gestational weeks in the Doppler velocimetry scan of the umbilical artery. The S/D ratio with the modified LTCC was a mean of 2.13 (normal range, <3). The results showed that the comparison of S/D ratio in both groups was not statistically different (Fig. 3).
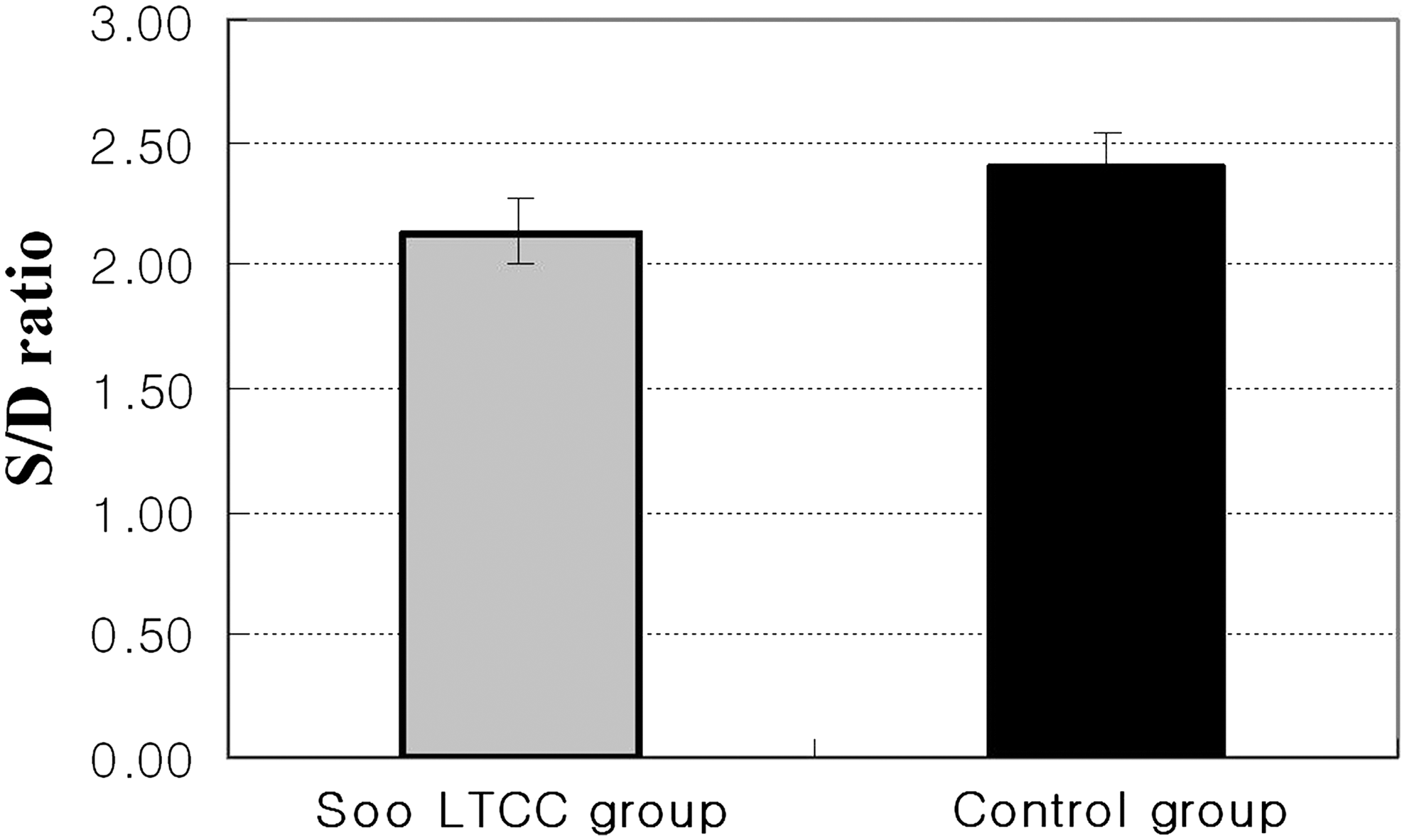
Comparison of the umbilical artery systolic–diastolic (S/D) ratio in laparoscopic transabdominal cervicoisthmic cerclage (LTCC) and the control group between 30 and 34 gestational weeks.
Discussion
The success of transabdominal cerclage has now been well established for more than three decades. Many authors have reported a cumulative fetal survival rate of about 90% in treated patients compared with a rate of 20% in the group of patients who did not undergo the procedure.7–10 Transabdominal cerclage also avoids the placement of foreign bodies within the vagina and the subsequent risk of ascending lower genital tract infection. 11 But, transabdominal cerclage has several real and potential drawbacks. In addition to the need for two laparotomies, during the placement of cerclage, a rupture in the thin-walled parametrial veins may lead to substantial hemorrhage. The laparoscopic approach has the advantage of obviating the need for a laparotomy, reducing the abdominal wall trauma and recovery time, and is less invasive with less postoperative adhesion formations. The amount of bleeding is also greatly reduced because the vascular area is magnified by the laparoscope. 8 In this study, this modified LTCC offers the benefit of reduced operation time and blood loss as well as decreased length of hospital day and faster recovery time in comparison with classical LTCC.
Several case reports and case series have been published in the medical literature describing LTCC that attest to its safety and effectiveness in well-selected patients.2,8,12,13 Previously reported retrospective studies of cervicoisthmic cerclage placed by both laparotomy and laparoscopy have operative complication rates of 0%–25% and fetal survival rates between 60%–100%. For some cases, an interval LTCC procedure is recommended to avoid additional surgery during pregnancy and to minimize blood loss during the procedure.2,14 However, an obvious disadvantage of interval LTCC is that pregnancy may not occur or result in early abortion. A review of literature revealed that more than 80% of traditional procedures were performed during pregnancies, usually after 10 weeks of gestation. 10 In the current study, we performed a modified LTCC procedure during pregnancy between 11 and 15 weeks of gestation without any complications. Cesarean delivery must be performed in all pregnancies. The cerclage is not removed after cesarean delivery as it may be useful or necessary during the next pregnancy. In this study, 11 patients who underwent the modified LTCC procedure subsequently became successfully pregnant after their first delivery.
Other risks and challenges exist with the performance of LTCC during pregnancy. One of the problems is LTCC-related risks to the mother associated with suturing the cervicoisthmic junction in a highly vascularized area close to the parametrial veins.13–15 This risk leads to an increase in operation time and morbidity. To address the risk, we developed an easier, modified method for LTCC that is sutured laterally to the uterine vessels at the level of the ascending and descending branch of the uterine artery. This level is easily detected because it is located at the avascular area. Therefore, dissection on the lateral portion of the cervicoisthmic junction is not necessary. One should identify the location of the ureter before suturing. Then, we can make windows between the ureter and the uterine vessels at the level of uterine isthmus above the uterosacral ligament to avoid puncturing the surrounding blood vessels. In our experience, wide dissection is not necessary; the vessel-free area can be easily determined by transillumination, and during the puncture of the paracervical tissue, the uterine vessels and the ureters are avoided by gently pushing them medially. The risk of damaging the parametrial vessels may be further reduced by the use of fiber optic lighting to transilluminate the broad ligament. Whittle et al. 16 reported that 7 cases were converted to laparotomy due to either complications arising from uterine vessel bleeding or impaired surgical visibility due to morbid obesity. In this study, we did not have any conversions to laparotomy. We suggest that our technique can be used by an experienced surgeon or surgical team with good operative laparoscopic skills.
The other problem was the difficulty of manipulating the uterus during pregnancy. In this modified LTCC, a uterine manipulator is not required. We use four trocars with atraumatic forceps for manipulation. These forceps enable the impregnated uterus to be gently pushed and controlled; however, too much pressure can cause preterm labor. Gestational age is also an important factor in the manipulation of the impregnated uterus because it could be difficult to manipulate a larger uterus, and the initial surgical access point may not be adequately exposed. We recommend that an elective modified LTCC procedure may best be done between 11 and 14 weeks of gestation.
Although the concern exists that the fetus may be affected during CO2 peritoneal insufflation, animal studies and human case series indicate the relative safety of laparoscopy during pregnancy.17,18 In addition to this, we used combined general and spinal anesthesia and also operated during a shorter time frame with modified LTCC to reduce the use and volume of inhalation anesthetics during the procedure.
The other major concern with the modified LTCC procedure was its effect on fetal development, as suturing material confines the uterine vessels. We sutured the impregnated uterus in a snug fashion so as to adapt suturing materials according to increasing size. This technique did not completely block blood flow to the uterus, and existing collateral circulation helps ensure that there will be no effect on fetal growth. There are many reports demonstrating a relationship between the Doppler indexes of fetal vessels and the fetal pressure of O2. Elevation of the umbilical artery Doppler index in the presence of positive end-diastolic flow is associated with hypoxemia at a steady state.19,20 Loss of end-diastolic flow in the umbilical artery is associated with significant worsening of hypoxemia, and acidemia may be present. 19 Therefore, we evaluated the S/D ratio using umbilical artery Doppler velocimetry between patients undergoing modified LTCC and a normal control group between 30 and 34 gestational weeks. The S/D ratio was not statistically different in the two groups. Blood supply to the uterus and fetal development were not affected by this modified LTCC because the pelvic vasculature is supplied with an extensive network of collateral connections that provides a rich anastomotic communication between different major vessel systems. 21
Overall, cerclage did not fail after the gestational age of 23 weeks. In our series, the successful pregnancy rate was 90%.
Conclusions
This is the largest reported cohort study on the use of a modified LTCC procedure during pregnancy. Our data indicated that this modified LTCC with a needle inserted laterally into the uterine vessels is an easier and safer procedure than the previously reported conventional LTCC with respect to operative technique, risk of complications, and successful pregnancy rate. Additionally, this modified LTCC does not influence fetal growth. We propose that this modified LTCC is feasible and easier to perform than traditional LTCC.
Footnotes
Disclosure Statement
No competing financial interests exist.