
Abstract
Abstract
Background:
To compare the efficacy of three chemotherapeutic combinations for laparoscopic hyperthermic intraperitoneal perfusion chemotherapy (HIPPC) in the treatment of malignant ascites secondary to unresectable gastric cancer (GC).
Materials and Methods:
From January 2010 to December 2013, 38 GC patients were randomly divided into three groups and treated by laparoscopic HIPPC with one of the three following chemotherapy combinations: raltitrexed (Ra) with oxaliplatin [trans-(±)-diaminocyclohexane oxalatoplatinum (
Results:
The intraoperative course was successful in all patients, and no perioperative death or complication related to laparoscopic HIPPC was documented. The median follow-up period was 9 months, and the median survival was 7.5 months for all patients. Patients in the Ra/
Conclusions:
Laparoscopy-assisted HIPPC provides modest yet encouraging efficacy for malignant ascites secondary to disseminated GC. Our preliminary data indicate that the chemotherapeutic combination of Ra/
Introduction
T
Hyperthermic intraperitoneal perfusion chemotherapy (HIPPC), combining chemo- with hyperthermic therapy, has demonstrated good efficacy in the prevention and treatment of peritoneal metastasis of malignant tumor.11–19 HIPPC in combination with cytoreductive surgery (CRS) improves the QOL and survival of patients with PC originating from GC,17–24 colorectal cancer,25–28 pseudomyxoma peritonea,29–32 and ovarian cancer. 33 Laparoscope-assisted HIPPC combines the benefits of a palliative and a minimally invasive procedure.34–37 Its use leads to less pain and surgical trauma, shorter recovery, and improved repeatability. Also, with the laparoscopic technique, occult metastases can be assessed with an increased accuracy compared to B-mode ultrasound, computed tomography, magnetic resonance imaging, or positron emission tomography–computed tomography.36,37 Recently, laparoscope-assisted HIPPC has been proposed by us and others as a palliative tool for patients with malignant ascites from PC, of both digestive and extradigestive origins.38–40 Potential candidates for laparoscope-assisted HIPPC are patients with peritoneal diffusive seeding and malignant ascites who are not suitable for surgical resection.
The aim of the present study was to evaluate three common chemotherapeutic combinations for laparoscopic HIPPC and their efficacy in treating malignant ascites secondary to disseminated, unresectable PC from advanced GC. Patients' QoL and survival were evaluated as the outcome, and the main end point was patients' long-term survival.
Materials and Methods
Inclusion and exclusion criteria
The diagnosis of GC was confirmed by a series of examinations, including exploratory laparotomy, gastroscopic biopsy, ascites cytology, ultrasonic imaging, and detection of serum tumor markers. Massive malignant ascites was verified by B ultrasound (Table 1). The diagnosis of unresectable PC from advanced GC was made by a medical team consisting of an imaging specialist, an oncologist, and a gastrointestinal surgeon. Patients with extensive abdominal adhesions due to multiple operations, complete intestinal obstruction, or minimal ascites were excluded from this study (Table 1). Written informed consents for HIPPC and laparoscopic examination were obtained from all patients. The study was approved (protocol number GZMCY20080825) by the Medical Ethics Committee of the Cancer Hospital of Guangzhou Medical College, Guangzhou, China.
CA199, cancer antigen 199; CEA, carcinoembryonic antigen; FCC, free cancer cells; GC, gastric cancer; PC, peritoneal carcinomatosis; PCI, Peritoneal Carcinomatosis Index; SD, standard deviation.
Laparoscopic examination and chemotherapeutic catheter placement
Laparoscopic examination and chemotherapeutic catheter placement were conducted as described before (Fig. 1). 39 In brief, patients were placed in a supine position following conventional endotracheal anesthesia, and a 1.2-cm transverse incision was made on the right side at the cross-point of the midclavicular line and the transverse surfaces, positioned approximately two fingerwidths (3–4 cm) below the umbilicus. All ascites were drained as completely as possible before an artificial pneumoperitoneum was established via a closed procedure with a pressure of 13 mm Hg (1 mm Hg = 0.133 kPa), and a trocar (1.2 cm in diameter) was inserted into the abdominal cavity via the first working port (Fig. 1, point A). Subsequently, a laparoscope (10 mm, 30°) was inserted via the trocar. The site, size, and clinical stage of the tumor were then examined by laparoscopic exploration.
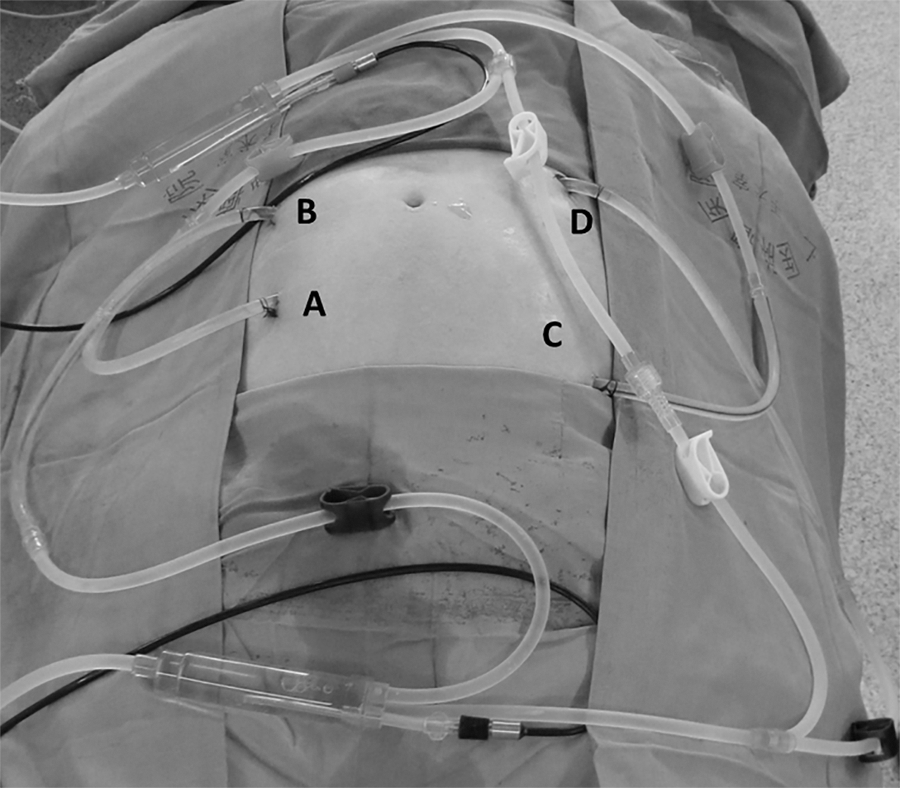
The placement sites of infusion catheters and outflow catheters in patients with malignant ascites secondary to disseminated, unresectable peritoneal carcinomatosis from advanced gastric cancer undergoing laparoscope-assisted hyperthermic intraperitoneal perfusion chemotherapy: point A, the first working port; point B, the second working port; point C, the third working port; and point D, the fourth working port. Gray clips mark two infusion catheters, black clips mark two outflow catheters, and white clips mark the loop circuit bypass for hyperthermic intraperitoneal perfusion chemotherapy preparation.
While laparoscopic examination was being conducted, three new ports were prepared under laparoscopic guidance. On the left side, the second and third working ports (both 1.2 cm long) (Fig. 1, points B and C) were prepared at the cross-point of the midclavicular line and the transverse surfaces, positioned approximately two fingerwidths (3–4 cm) above and below the umbilicus, respectively. On the right side, the fourth working port (1.2 cm long) (Fig. 1, point D) was prepared at the cross-point of the midclavicular line and the transverse surface, positioned approximately two fingerwidths (3–4 cm) above the umbilicus. Subsequently, a trocar (1.2 cm in diameter) was inserted into the abdominal cavity through the working port under laparoscopic guidance (Fig. 1). Two outflow catheters were placed in the Douglas cavity, the lowest region in the pelvic cavity, via the second and the fourth working ports using laparoscopic guidance. An infusion catheter was placed in the left superior abdominal cavity via the third working port guided by laparoscope. The laparoscope was then placed in the right superior abdominal cavity, and the trocar was completely inserted. Subsequently, the laparoscope was removed, and one outflow catheter was placed in the right superior abdominal cavity under the guidance of the last remaining trocar (Fig. 1).
HIPPC procedures
HIPPC was performed using the “high-precision body cavity hyperthermic perfusion treatment system” invented by us and custom-manufactured (model BR-TRG-II; Guangzhou Baorui Medical Instrument Co., Ltd., Guangzhou). The system has a precise temperature control of ±0.15°C and a flow control of ±5% and couples with an automatic cooling function. These innovative devices have been approved by the State Food Drug Administration Firearms of China (approval number 2009-3260924). Four perfusion catheters (two infusion catheters and two outflow catheters) were placed in the peritoneal cavity or the pelvic cavity connected with the “catheter system” (Fig. 2A) of this high-precision body cavity hyperthermic perfusion treatment system.
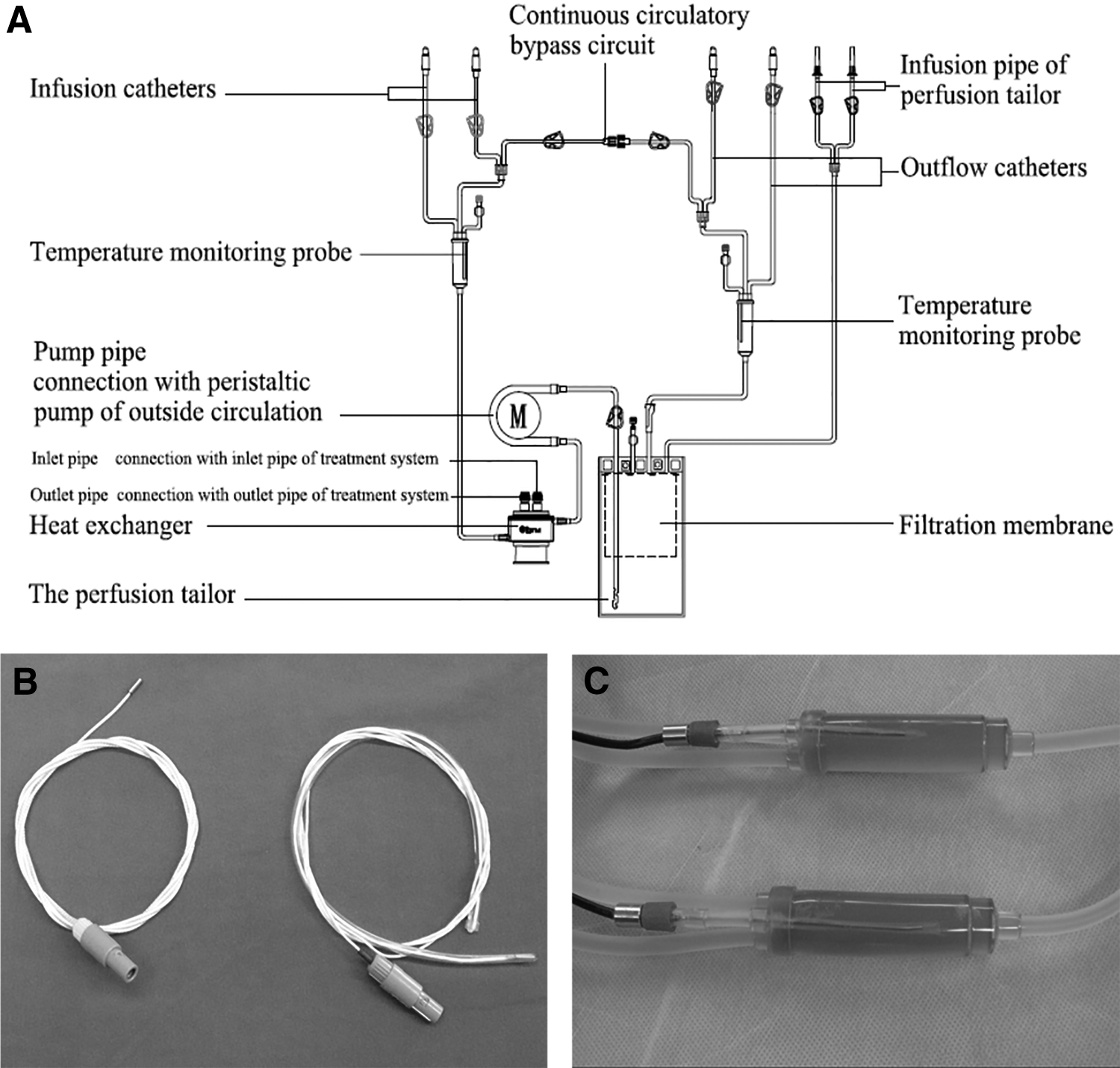
Structure of the BR-TRG-II-type high-precision body cavity hyperthermic perfusion treatment system and temperature monitoring probes.
The treatment temperature during HIPPC was measured by the high-precision body cavity hyperthermic perfusion treatment system, and the temperature monitoring probes were placed in the infusion catheter and outflow catheter through a blind pipe in the catheters (Fig. 2B) or on the tympanic membrane surface through the external auditory canal (Fig. 2C). Patients' blood pressure, heart rate, respiration rate, and blood oxygen saturation values were monitored using the “multiparameter patient monitor system” (model G3HJ20025; Shenzhen MINDRAY Bio Medical Electronic Ltd. by Share Ltd., Shenzhen, China).
HIPPC was delivered for three sessions for each patient, lasting about 90 minutes for each session. The first was completed in the operating room, with the patient under endotracheal anesthesia after the placement of perfusion catheters under laparoscopic assistance. The second and the third sessions were performed in the intensive care unit on the first and the second days after the first HIPPC session, respectively. Intravenous propofol was administered continuously at a rate of 3–8 mL/hour as an anesthetic agent, and its administration was adjusted according to the patient's status.
The 38 patients treated with laparoscopic HIPPC include 22 who had had no previous surgery for GC and 16 patients with PC after GC resection. The groups of 16 and 22 patients were randomly divided into the raltitrexed (Ra) with oxaliplatin [trans-(±)-diaminocyclohexane oxalatoplatinum (
When
All the patients received one to six cycles of systemic chemotherapy according to FOLFOX4 (folinic acid, fluorouracil, and oxaliplatin) at the beginning of 2 weeks following laparoscope-assisted HIPPC.
Evaluation of HIPPC efficacy
To assess the therapeutic efficacy on ascites remission and tumor progression, serum tumor markers were measured, and B ultrasonic and/or computed tomography examinations were performed at least once every 2 weeks. The status of ascites remission, Karnofsky Performance Scale (KPS) for QOL, and serum tumor markers of all participants were determined 4 weeks post-HIPPC to evaluate clinical efficacy.
The clinical efficacy for all participants was classified into three grades, according to previously modified World Health Organization criteria for efficacy assessment of malignant ascites. 9 Toxic effects of anticancer drugs were graded according to the common toxicity criteria of the National Cancer Institute for adverse events. 41 The anatomical extension of the GC in the peritoneal cavity was evaluated by the Peritoneal Carcinomatosis Index (PCI) as described by Schoennemann et al. 42
Statistical analysis
Overall survival was analyzed and compared with the Kaplan–Meier method using the GraphPad (San Diego, CA) Prism software (version 5.01). KPS scores for each patient's QOL were also analyzed using Student's t test for paired data. P < .05 was considered statistically significant.
Results
Patients' clinical data
From January 2010 to December 2013, 38 patients with massive malignant ascites secondary to unresectable GC, including 23 males and 15 females (age, 33–76 years; median, 59 years), were admitted to the Intracelom Hyperthermic Perfusion Therapy Center, Cancer Hospital of Guangzhou Medical College. The average interval from time of diagnosis to time of study enrollment of these patients with malignant ascites was 16 days (range, 5–45 days), and the average amount of ascites measured as drainage fluid during laparoscopic laparotomy was 3825.81 ± 121.37 mL (range, 2500–6500 mL). The KPS score for QOL was a mean of 51.75 ± 6.35 (range, 40–70).
In total, 114 sessions of HIPPC were successfully conducted. The mean operating time was 45 minutes (range, 25–75 minutes) for laparoscopic exploration and placement of four perfusion catheters in all patients involved in this study. No postoperative death or complication related to laparoscopic HIPPC was documented.
The free cancer cell rate in malignant ascites was about 84.21% (32/38) determined by ascites cytology examination. The mean PCI by laparoscopic examination was 27 ± 1.27 (range, 17–35) in our patient cohort (Table 1).
Vital sign fluctuation
During HIPPC, temperature in the infusion catheter was stabilized at about 43°C. Temperature in the outflow catheter was about 41.70 ± 0.23°C, ranging from 41.65°C to 41.80°C. The maximum temperature on the tympanic membrane surface was less than 37.5°C in all patients (Table 2).
HIPPC, hyperthermic intraperitoneal perfusion chemotherapy.
In all patients of this study, blood oxygen saturation values were maintained within the normal range during HIPPC. Fluctuations of blood pressure were mild, and a slight increase in diastolic pressure was observed. Heart and respiration rates increased obviously during HIPPC but were well tolerated by the patients. All vital signs returned to the pre-HIPPC level 30 minutes post-HIPPC (Table 2).
Clinical efficacy
After HIPPC, the KPS scores for QOL assessment of these patients increased from 51.75 ± 6.35 pre-HIPPC to 85.25 ± 7.36 post-HIPPC. There was no significant difference (P > .05) in the increase of the KPS scores among the three groups between pre-HIPPC and post-HIPPC (24.56%, 23.38%, and 23.67%, respectively) (Table 3).
CA, chemotherapeutic agent; DDP, cisplatin; KPS, Karnofsky Performance Scale; L-OHP, oxaliplatin [trans-(±)-diaminocyclohexane oxalatoplatinum]; MMC, mitomycin C.
Patients' symptoms related to malignant ascites were alleviated after HIPPC. Thirty-one patients (81.58%) had a complete remission (CR), 7 patients (18.42%) had a partial remission (PR), and the objective remission rate (ORR) (ORR = CR + PR) was 100%. All patients with Ra and
Adverse effects
During HIPPC treatment, patients had no significant discomfort except for transient abdominal distension. A slight gastrointestinal reaction was observed in 6 patients in the Ra/
Follow-up and prognosis
All patients of this study were followed up, and the median follow-up interval was 9 months (ranging from 2 to 17 months). Patients' survival in our cohort ranged from 2 to 17 months (median, 7.5 months) (Fig. 3). The patients' survival in the Ra/
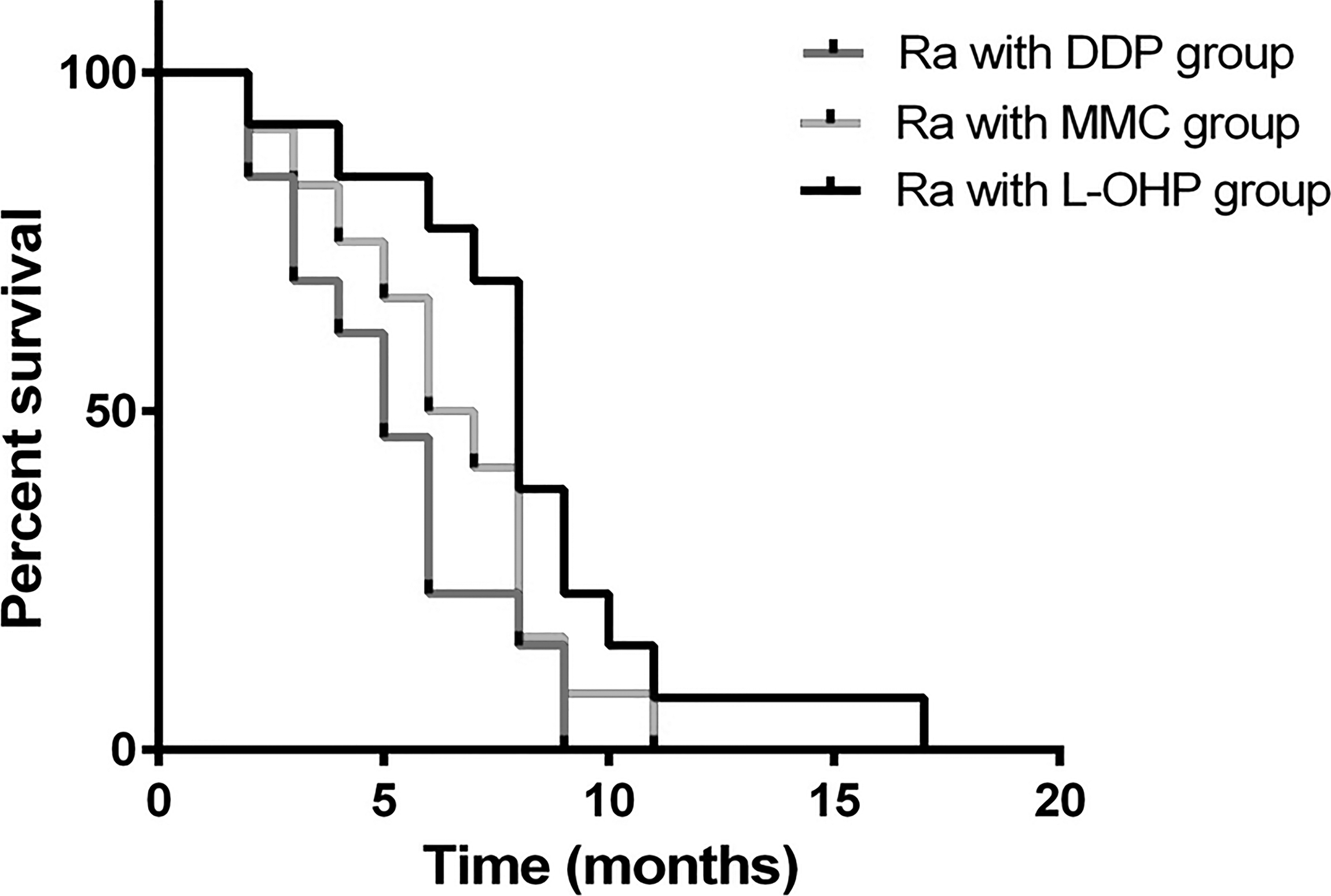
A Kaplan–Meier survival curve for patients with malignant ascites secondary to unresectable gastric cancer treated by laparoscopic hyperthermic intraperitoneal perfusion chemotherapy. The survival time of the patients ranged from 2 to 17 months, with a median survival time near 7.50 months. Patients' survival in the raltitrexed (Ra)/oxaliplatin [trans-(±)-diaminocyclohexane oxalatoplatinum (
Six patients (15.78% of the cohort; 2 received Ra with
Discussion
In this study, we evaluated the safety and efficacy of laparoscopic HIPPC in patients with malignant ascites secondary to disseminated, unresectable PC from advanced GC. During HIPPC, blood oxygen saturation rates were maintained within the normal range in all patients in our study. The fluctuations of blood pressure and temperature were mild, and the maximum temperature on the tympanic membrane surface was less than 37.5°C. Heart and respiration rates of all patients increased obviously during HIPPC, but all returned to pre-HIPPC levels within 30 minutes post-HIPPC. These results demonstrated that HIPPC has only a mild influence on vital signs. Consistent with previous studies,33,38,39 this study further demonstrated that laparoscope-assisted HIPPC successfully alleviated symptoms related to malignant ascites, and patients' KPS scores improved substantially. No intraoperative death or complication related to laparoscopic HIPPC was documented, suggesting that laparoscope-assisted HIPPC is a safe, feasible, and effective procedure for the treatment of debilitating malignant ascites induced by disseminated, unresectable PC from advanced GC.
PCI, a useful prognostic indicator, can also be used for sequential determination of the extent of carcinomatosis over time and the likelihood of a completely CRS after re-operative surgery. Patients with high PCI should not be considered for CRS. 42 Like other carcinomatosis assessments, PCI is determined at the time of surgical exploration or laparoscopic exploration of the abdomen and pelvis. In this study, the median PCI of the cohort was 27 (range, 17–35), indicating diffused peritoneal metastases of GC in all patients.
The common use of laparoscopy in the diagnosis and treatment abdominal malignancy has led to increased reports on the occurrence of port-site metastases. The proposed mechanism is that cancer cells are forced into the subcutaneous tissue along the trocar sites as a result of increased intraabdominal pressures.35–37 In this study, 6 patients (15.78%) were re-admitted with abdominal wall metastasis at the laparoscopic puncture sites. All patients in this study had high PCI, and HIPPC is not effective for treating PC with diameters over 5 mm, so surgical resection of port-site metastases was not considered after laparoscope-assisted HIPPC.
Optimizing chemotherapeutic agents and combinations is critical in achieving satisfactory curative effect of HIPPC. Currently, there is no standard in China or abroad on chemotherapeutic drug selection and treatment regimen for HIPPC, and the usual practice is the implementation of systemic chemotherapy with reference to the primary disease. 5-Fluorouracil is the most commonly used chemotherapeutic agent for malignant tumors from gastrointestinal tract. It functions as an inhibitor of thymidylate synthase, a key enzyme in thymidine synthesis, and therefore interrupts DNA replication. However, 5-fluorouracil must be metabolized into 5-fluorouracil deoxyribonucleoside for its antitumor effect. Ra is another thymidylate synthase inhibitor that does not require hepatic metabolism and is widely used for tumors of the digestive system. In this study we chose Ra instead of 5-fluorouracil for HIPPC in the treatment of debilitating malignant ascites induced by disseminated, unresectable PC from advanced GC and achieved satisfactory curative efficacy.
MMC belongs to the azithromycin family of natural products. It is a DNA cross-linking and damaging agent, making it a useful antitumor compound. Some studies have shown that 30 mg of MMC used in HIPPC for 2 hours killed all GC cells found in the ascites and on the peritoneal surface. 24 However, in this study, severe hematological events occurred in 2 of the patients treated with MMC, even though the concentration of MMC (6 mg/m2, or 10 mg total) in our study was substantially lower compared with other studies. Although it is currently unknown why such serious hematological reactions occurred, we suggest in the future that hematological events should be closely monitored when MMC is used as the HIPPC chemotherapeutic agent.
DDP is platinum-based and was the first medicine developed in its drug class. Despite the many newer chemotherapy drugs developed over the past decades, DDP is still widely used today for treating cancers, including sarcoma, small cell lung cancer, and stomach and ovarian cancer. However, DDP has a poor efficacy in treating patients with digestive duct cancers.
Like other platinum compounds,
In this study, patients receiving Ra/
Due to the relatively small scale of the present study, it is possible that some adverse events and complications were not represented but may be revealed with a larger patient cohort. Our results, however, indicate that laparoscopic HIPPC is a safe, feasible, and effective procedure for the treatment of debilitating malignant ascites induced by disseminated, unresectable PC from advanced GC. Our preliminary data also indicate that the chemotherapeutic combination of Ra/
Footnotes
Disclosure Statement
No competing financial interests exist.