
Abstract
Abstract
Introduction:
Reliable closure and infection prevention are the main barriers for implementation of pure transgastric peritoneoscopy. The primary aim of this study was to assess healing of over the scope clip (OTSC) closed gastrotomies.
Materials and Methods:
Pure transgastric peritoneoscopy was performed in 7 pigs. The pigs were randomized to 14 or 28 postoperative days (POD) of follow-up. Decontamination of the access route was performed before instrumentation. A full necropsy was performed. Closure was evaluated with histopathological examination of excised gastrorrhaphies.
Results:
Three pigs were allowed 14 POD of follow-up, and 4 pigs were allowed 28 POD of follow-up. Survival was achieved in 6 of the 7 animals; 1 pig was euthanized due to diffuse peritonitis. Based on our definition, full-thickness healing had only been achieved in a single pig allowed 28 POD. With respect to clinical relevancy, full-thickness healing was deemed achieved in 4 of 6 pigs completing follow-up and in all pigs allowed and surviving 28 POD. Access required repeated punctures and the use of several endoscopic instruments.
Conclusions:
Full-thickness healing of the gastrotomy was only found in a single case when adhering to the per protocol definition. Endoscopic ultrasonography-guided access was difficult. It lacks reproducibility and needs refinement. Despite a combined decontamination regimen, infectious complications still occurred.
Introduction
N
The most significant barriers for clinical implementation of TG pure NOTES are reliable gastric closure and prevention of infectious complications. The incidence of postoperative infectious complications has been reported to be as high as 100% in animal studies, 3 raising the question of how to achieve adequate decontamination of the access way. For gastric closure, several methods have been evaluated such as the over the scope clip (OTSC® System; Ovesco Endoscopy AG, Tübingen, Germany), which holds the promise of quick and reliable closure. 4 Contradictory results regarding the inflammatory response and healing of gastrotomies closed by the OTSC System have been reported,5–8 raising hypothetical concerns of postoperative perforation of the gastric wall. 9
The primary aim of this study was to examine the healing process of gastrotomies closed with the OTSC System. Second, the study aimed to evaluate endoscopic ultrasonography (EUS)-guided access and the efficiency of a combined decontamination regimen against the risk of postoperative infectious complications.
Materials and Methods
Animals and preparation
Survival experiments were performed in 7 female pigs of the Danish Landrace breed (median weight, 37 kg; range, 35–41 kg). Institutional Review Board approval was obtained from The Animal Experiments Inspectorate in Denmark (case number 2012-15-2934-00035). The study was performed at The Laboratory Animal Facility, The Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark.
The pig pens were without hay and litter, and the pigs were fed a liquid diet consisting of Nutridrink (Nutricia A/S, Allerød, Denmark) 3 days prior to the procedure. Preoperative fasting was 12 hours.
Preanesthesia sedation consisted of intramuscular administration of zoletil mix. General anesthesia was achieved with propofol bolus followed by continuous intravenous infusion. Analgesia consisted of continuous intravenous infusion of fentanyl. Anesthesia was performed and monitored by veterinary technicians. Preoperative prophylactic antibiotics consisted of 20 mg/kg of body weight of intravenous metronidazole and cefuroxime. Intramuscular heparin was administered for thromboprophylaxis.
Before intubation, the mouth was rinsed with 20 mL of 0.2% chlorhexidine. Immediately after intubation and before introduction of the endoscope, the mouth was cleaned again with swabs soaked in 0.2 chlorhexidine using a grasper. A linear ultrasonic videogastroscope (model GF-UCT140-AL5; Olympus, Tokyo, Japan) was advanced into the stomach transorally together with an overtube (Guardus® overtube; US Endoscopy, Mentor, OH). Gastric lavage was performed with a volume of 1 L of sterile water containing 1 g of metronidazole and 1 g of cefazoline. The stomach content was fully aspirated prior to gaining TG access.
EUS-guided TG access
Internal indentation from abdominal palpation and diaphanoscopy was used to locate the anterior gastric wall. The precise location of access was then determined based on EUS, identifying the anterior abdominal wall from within the gastric lumen, avoiding adjacent organs or vessels at the access point. The gastrotomy was created by an EUS-guided puncture of the gastric wall with a 19-gauge needle (EchoTip® Ultra; Cook Medical, Bloomington, IN). Correct needle tip placement in the peritoneal cavity was controlled by instillation of sterile physiological saline. This fluid cushion also helped to displace structures adjacent to the puncture site. Thereafter, a guidewire (VisiGlide; Olympus) was introduced through the needle. The fistula tract was dilated with an 18-mm balloon (CRE™ wireguided balloon dilatation catheter and Alliance™ II single-use syringe/gauge assembly; Boston Scientific, Natick, MA) over the guidewire to accommodate passage of the endoscope. Sphincterotomes (CleverCut3; Olympus) and needle knives (NeedleCut3; Olympus) were available to expand the fistula tract, making advancement of the balloon possible, if required.
With the ultrasonic videogastroscope in place within the peritoneal cavity, a Veress needle was introduced through the abdominal wall under visual guidance from the videogastroscope. The skin was disinfected before puncture. Pneumoperitoneum with carbon dioxide was established through an autoinsufflation system set at 12 mm Hg. After penumoperitoneum, a peritoneoscopy lasting approximately 10 minutes was performed with the ultrasonic videogastroscope in each animal.
Gastrotomy closure
An OTSC applicator cap with a 12-mm OTSC System set mounted on a dual-channel gastroscope (model GIF-2T160; Olympus) was introduced into the stomach. A dual grasping instrument (OTSC-Twin Grasper; Ovesco Endoscopy AG) was used to approximate the two sides of the gastrotomy, and closure was achieved by deploying the OTSC clip. The closure site was inspected macroscopically for adequate closure. If deemed inadequate, endoscopic clips (Quickclip; Olympus) and the supplementary OTSC Reloader (Ovesco Endoscopy AG) were available.
Randomization
The pigs were randomized in blocks of 2 for either 14 or 28 postoperative days (POD) of follow-up. In this way, at least 1 pig was randomized for either group on a given operation day. The randomization was revealed at the end of each day; thus all staff members were blinded to the respective allocation during the actual procedures.
Follow-up
The pigs were allowed access to ordinary feeds the same day as they were operated on (0 POD). Intramuscular buprenorphine and meloxicam were administered as analgesics until 1 POD and 2 POD, respectively. The pigs were monitored clinically by veterinary technicians throughout the postoperative period. Euthanasia and necropsy would be performed if a pig showed signs of deteriorating health. Survival was assessed with respect to allocation (14 or 28 POD), at which point the pigs were euthanized. Necropsy was performed by a veterinarian pathologist as described elsewhere. 10 The abdominal cavity was examined for organ injury, adhesions, and infectious lesions. The closed gastrotomy was inspected for macroscopic full-wall closure. The gastrorrhaphies were excised, formalin-fixed, and processed further to permit histological evaluation of full-thickness healing and signs of inflammation, ischemia, or necrosis. The histological examination was performed by a pathologist blinded to the respective allocation.
Outcome parameters
The primary outcome parameter was microscopic full-thickness healing of the gastrotomy, defined as healing of the fistula tract with layer-to-layer fibrosis covered by intact epithelium on the luminal side and intact mesothelium on the peritoneal side. The excised gastrorrhaphies were also examined for histological signs of inflammation, ischemia, and necrosis. Based on results regarding the level of fibrosis and inflammatory response, the pathologist gave a blinded assessment of group allocation.
Secondary outcome parameters were uncomplicated follow-up and survival, intraoperative complications, lesions in the abdominal cavity related to EUS-guided access, adhesions, and signs of infectious complications. Total procedural time, time for EUS-guided TG access (from the end of gastric lavage until the endoscope located in the peritoneal cavity), and time for gastrotomy closure (from introduction of the endoscope with the attached OTSC cap to the stomach to successful closure evaluated by visual inspection) were also recorded.
Quantitative data are expressed as median and range or as number and percentage.
Results
Animal allocation with descriptive characteristics regarding access and closure is depicted in Table 1. Pathology revealed during necropsy for each individual animal with respect to allocation is summarized in Table 2. Results regarding full-thickness healing of the respective gastrorrhaphies are given in Table 3.
Animal number represents the consecutive order in which the animals had surgery. For clips in situ at necropsy, (+) indicates the presence of and (0) indicates the absence of this parameter.
b, balloon dilation; n, needle knife; OTSC, over the scope clip; POD, postoperative days; s, sphincterotome.
For peritoneal granulation, fibrin deposits, and adhesions, (0) indicates none, and (+++) indicates severe.
DFP, diffuse fibrinopurulent peritonitis; POD, postoperative days.
For focal peritonitis, omentum adhesion, microscopic abscesses, foreign body giant cells (FBGC), ischemia/necrosis, and full-thickness healing, (+) indicates the presence of and (0) indicates the absence of the specific parameter. The term per protocol adheres to the definition of closure given in Materials and Methods. For the parameters ulceration and inflammation (overall/acute/chronic), (0) indicates none, (+) indicates slight, (++) indicates moderate, and (+++) indicates severe.
POD, postoperative days.
Three pigs were allocated to 14 POD (pigs 2, 5, and 7) and 4 pigs to 28 POD (1, 3, 4, and 6) of follow-up (Table 1). The postoperative follow-up was uneventful for 6/7 (86%) pigs. One pig allocated to 28 POD (number 4) had a slight fever and decreased activity on 2 POD but recovered on 3 POD. The health deteriorated again on 5 POD, and the pig was euthanized on 6 POD. The remaining pigs survived with uneventful recovery until 14 POD (3 pigs; median weight, 45 kg; range, 43–46 kg) and 28 POD (3 pigs; median weight, 50 kg; range, 44–53 kg).
Total procedure time was a median of 95 minutes (range, 68–105 minutes). EUS-guided access was achieved with a median duration of 43 minutes (range, 22–66 minutes). Closure of the gastrotomy lasted a median of 7 minutes (range, 5–12 minutes). Correct needle tip placement and access were achieved through the first transmural puncture in 4 pigs (Table 1). In the remaining 3 pigs correct needle tip placement and advancement of the guidewire were achieved in the second to fourth puncture. Immediate advancement of the balloon over the guidewire was only possible in a single case. A sphincterotome was needed in 5 out of the remaining 6 pigs, of which 3 required further use of a needle knife before advancement of the balloon was possible. In 1 pig the sphincterotome could not be guided into the fistula; thus a needle knife was used instead to expand the fistula for the balloon. There were no immediate injuries to adjacent organs according to the peritoneoscopic examination. Sufficient closure with a single OTSC System was achieved in 6/7 (86%) pigs. Additional use of two endoclips was necessary in 1 pig before the closure was deemed sufficient.
One intraoperative complication occurred in a pig allocated to 14 POD (pig 2). The passage of the OTSC System resulted in a 5-cm longitudinal superficial mucosal tear in the proximal esophagus. The tear was revealed during retraction of the endoscope after closure had been achieved. There was only minor bleeding, and no treatment was performed. Necropsy on 14 POD revealed complete healing of the mucosal tear without stenosis.
Pathological lesions in the peritoneal cavity was found in 2/7 (29%) pigs (pigs 4 and 5; Table 2). Necropsy of the pig that was euthanized due to deteriorating health revealed acute diffuse fibrinopurulent peritonitis. The gastrorrhaphy was intact, and there were no signs of bowel perforation. No other pathology was present in the abdomen. The infection had spread to the left pleura, resulting in acute fibrinopurulent pleuritis. This pig required four EUS-guided transmural punctures and the use of both the sphincterotome and the needle knife before advancement was possible. The other case of pathology was a single encapsulated abscess measuring 1.5 cm in diameter in the omentum of a pig allocated to 14 POD of follow-up. The remaining pigs were without any intraabdominal pathological lesions.
Regarding the gastrorrhaphies, macroscopic inspection during necropsy revealed no mucosal ulcerations and the serosa side had no signs of peritonitis or granulation. The omentum adhered to the closure site in 5/7 (71%) pigs. No other adhesions were present. Microscopy showed extensive ulceration of the mucosa and severe inflammation with neutrophil granulocytes and localized micro-abscesses in relation to the OSTC System in three of the excised gastrorrhaphies (pigs 2, 4, and 5; Table 3), all with the OSTC System in situ (Fig. 1). In one of these (pig 4, euthanized on 6 POD), the inflammation was not limited to the proximity of the OSTC System but was evident in all layers of the gastric wall and was accompanied by acute inflammation of the serosa. In three excised gastrorrhaphies (pigs 1, 3, and 7) only minute mucosal ulcerations were seen and were accompanied by slight to moderate chronic inflammation with lymphocytes and plasma cells, all without the OSTC System in situ (Figs. 2 and 3). In one of the excised gastrorrhaphies (pig 6), also without the OSTC System in situ, no mucosal ulcerations and only slight chronic inflammation were seen (Fig. 4). Based on the definition, histology-proven full-thickness healing was only achieved in this gastrorrhaphy for 1/7 pigs (14%). In all but one (pig 6) of the excised gastrorrhaphies, areas of chronic inflammation with foreign body giant cells were seen in relation to ingested feed lodged inside the gastric wall. No signs of ischemia or necrosis were identified, and all but one (pig 4, euthanized on 6 POD) showed extensive fibrosis in relation to the fistula tract.
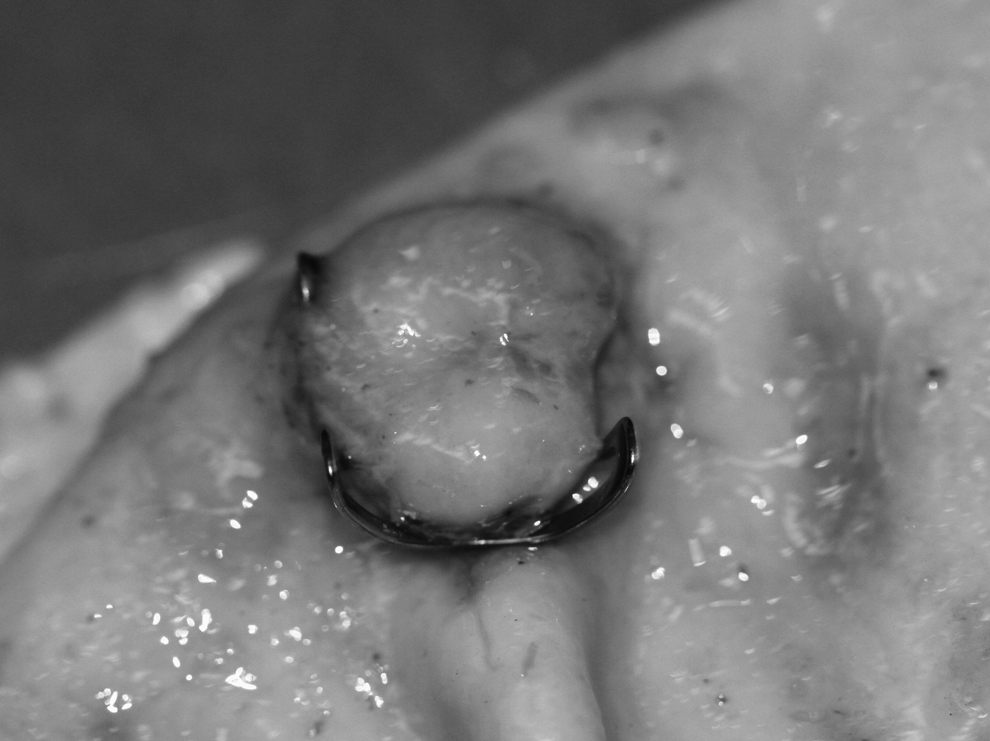
Gastrorrhaphy with the OTSC System in situ at necropsy.

Microscopy of excised gastrorrhaphy with ulceration, chronic inflammation, and foreign body reaction to ingested feed lodged in the wall (hematoxylin and eosin stain).

Gastrorrhaphy without the OTSC System showing macroscopic healing of the mucosa.
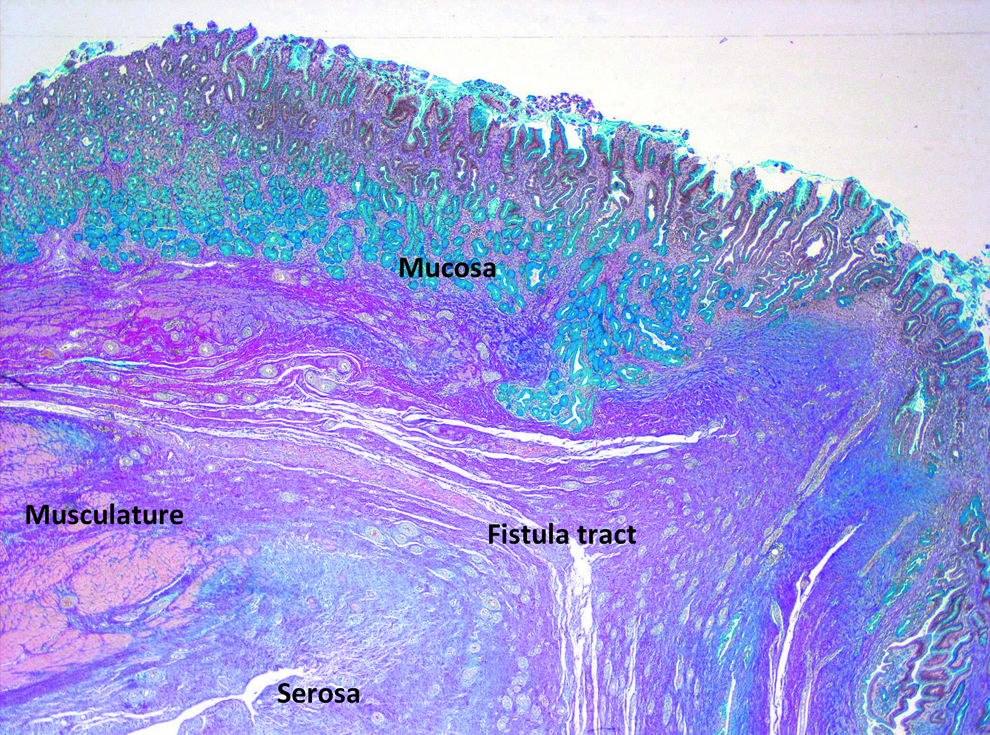
Full-thickness healing of the fistula tract with layer-to-layer fibrosis and intact mucosa and serosa (Alcian blue and van Gieson stain).
Regarding the pathologist-blinded assessment of respective allocation, 1 pig allocated to 28 POD was euthanized ahead of time on 6 POD due to deteriorating health and as such was assessed as allocated to 14 POD (pig 4; Table1). Excluding this case the pathologist's assessment was only wrong in a single case out of the remaining 6. One pig allocated to 14 POD but with full-thickness healing was assessed as allocated to 28 POD (pig 6; Table 1). The pathologist's assessment was thus correct in 83% of cases (5/6).
Discussion
In summary, closure was easily achieved with the OTSC System. Despite this, full-thickness healing was only present in a single case when adhering to the protocol definition. EUS-guided TG access was achieved without iatrogenic organ lesions. The technique was not simple and lacked reproducibility with repeated transmural punctures. One pig having four punctures was euthanized prematurely due to infectious complications. One case of mucosal tear occurred from passing the OTSC System through the esophagus. This did not require surgical intervention and healed without complications. Despite using a combined decontamination regimen, an abscess was found in the omentum of 1 pig during necropsy.
Several techniques for TG access have been evaluated in the literature.9,11–14 Despite showing promise, common for all techniques is the lack of sufficient evidence on safety, efficiency, and reproducibility due to various study designs and low sample sizes. For the same reasons comparison of techniques as to which is best suited in clinical trials is difficult. It has been shown that direct endoscopic gastrotomy creation with a needle knife in a “blind” manner carries a high risk of iatrogenic organ injury. 15 EUS-guided access has the advantage that it may help minimize these lesions to adjacent organs. 16 In the present study EUS-guided access ensured that no iatrogenic lesions or bleeding requiring intervention occurred. EUS-guided transmural puncture and immediate balloon advancement lacked reproducibility. This was reflected in the number of punctures and instruments needed before balloon dilatation and advancement of the endoscope were possible. The lack of reproducibility and difficulties associated with access was also reflected by the median procedural time of 43 minutes.
Further refinement of the technique is mandatory. We encountered problems with the oblique-guided needle access through the stomach wall due to the construction of the linear EUS endoscope. This access resulted in a separation of the stomach wall layers while attempting to pass with accessories and the EUS endoscope. A forward-viewing EUS scope could perhaps facilitate a TG puncture perpendicular to the gastric wall and thereby ease advancement through the fistula. Predilatation with bougies over the guidewire has also been shown to facilitate gastrotomy creation and should be evaluated in future EUS-guided trials. 17
Results from experimental studies and experience from laparoscopic intragastric surgery have proposed that the gastrotomy does not necessarily need surgical closure after TG NOTES, especially if access has been achieved with balloon dilation.18,19 The gastric access site seems to close rapidly within minutes after withdrawal of the endoscope. 19 There are several limitations to this proposal. It is unknown what effect a longer procedural time has on the closure of the dilated TG fistula. Second, the evidence is based on small sample sizes. Finally, from a surgeon's perspective it would be unethical not to perform surgical closure of the access site. Leak rates as low as 1% in a NOTES setting have been deemed unacceptable due to the associated risk of peritonitis and morbidity. 4 This is an unnecessary risk for the patients, as the same procedure could be performed with the conventional laparoscopic technique.
In the present study the OTSC System was evaluated for surgical closure of the access site. Full-thickness healing according to the protocol was only achieved in a single case. It can be argued that the definition used in this study was too strict and that minute microscopic mucosal ulcerations and slight to moderate chronic inflammation were without clinical importance. From this perspective full-thickness healing were achieved in all pigs allocated to and surviving until 28 POD of follow-up. Full-thickness healing was also achieved in a pig allocated to 14 POD of follow-up. Thus it could be argued that full-thickness healing was achieved in 4 out of the total 7 pigs (57%) (Table 3). The remaining pigs euthanized on POD 14 had severe mucosal ulcerations and inflammation of the gastric wall with micro-abscesses. In an earlier study involving 10 gastrotomies closed with the OTSC System, mucosal ulcerations, severe inflammation, and micro-abscesses were present in all pigs at 14 POD. 9 It was then speculated whether these histopathological findings might predict clinical progression toward spontaneous perforation of the gastric wall.
Other studies have documented the histopathology of OTSC closed gastrotomies. Two studies have reported no signs of inflammation or abscesses at 10 and 14 POD, respectively.6,8 Another study reported mucosal ulcerations without ischemia or inflammation at 14 POD. 5 Full-thickness healing was achieved in all three studies but without a clear statement of histological definition. Another study reported complete healing defined as gastric wall layers with intact and continuous structures without mucosal erosion and interrupted layers due to significant fibrosis. 7 This study reported no incidences of ischemia or necrosis, but complete healing was only achieved in 4/6 cases (67%) on 14 POD.
The results presented in this study support the use of the OTSC System for gastrotomy closure. The severe inflammatory response and mucosal erosions seen at 14 POD showed promising signs of healing at 28 POD. With respect to clinical relevance, full-thickness healing had been achieved in all animals surviving until 28 POD, leaving no hypothetical risk of spontaneous perforation. To further support the use of the OTSC System in TG NOTES, it has been shown that OTSC closed gastrotomies have the same leakage pressure as hand-sutured closure. 7 Evidence also supports the safe and effective use of the OTSC System for closure of gastrointestinal fistulas, iatrogenic perforations, and acute anastomotic leaks.20,21
The OTSC System was no longer in situ in the animals surviving until 28 POD and in 1 animal allocated to 14 POD follow-up, with all having clinical relevant full-thickness healing in common. It could be speculated that the presence of the clip is the reason for the severe histopathology found in the remaining animals and thus delaying the healing process. Larger studies are required to fully evaluate this aspect.
Some studies evaluating closure methods have used bursting pressure of the gastrorrhaphy as a measure for sufficient closure or adequate healing. Although contradictory results have been reported, the majority of randomized experimental studies report bursting pressure of OTSC closed gastrotomies comparable to or higher than that achieved with the gold standard of hand-sutured closure.7,22 Whether the reported high pressure levels have any clinical relevance could be debated. It has been reported that postoperative vomiting can elicit an intragastric pressures as high as 290 mm Hg, but at the same time the intraabdominal pressure reaches 255 mm Hg. Thus the resulting additional pressure exerted on the gastric wall only reaches 45 mm Hg. 22 As the clinical relevance of pressure testing and subsequent leakage is debatable, the primary aim of this study was to evaluate the histopathology of the healing process instead.
The results from animal survival studies are contradictory as to the role of bacterial contamination on the risk of infection. The incidence of infectious complications after TG access has been reported in the range from 0% to 100%. 3 Several decontamination measures both as standalone and in combination have been evaluated. 3 Randomized animal trials comparing contamination after TG NOTES with that of laparoscopy or open surgery have also been performed. In these trials both the TG laparoscopic and open groups had positive cultures at some point during the postoperative period, but clinical peritonitis did not develop.23,24 In the present study a rigorous decontamination regimen was adopted including oral chlorhexidine, gastric lavage with an antibiotic solution, sterile overtube, and systemic administration of prophylactic antibiotics. In an earlier study using only intravenous antibiotics, local to multifocal peritoneal granulation was observed in 100% as a sign of minor spillage/contamination. 9 No such pathological lesions were found in the present study, indicating that the decontamination regimen minimized spillage/contamination. Despite this reduction, 28% (2/7) still presented with infectious complications. It could be argued that one of these was due to multiple transmural perforations leading to increased intraperitonal bacterial contamination and subsequent peritonitis. For future application, access by TG NOTES should be achieved in the first try. Failure to do so should prompt the surgeon to convert the procedure to prevent complications.
Due to the contradictory results acquired from animal studies, it has been proposed that the animal model is not representative for the human setting concerning the risk of postoperative infections. 25 A review on 130 patients enrolled in different pre-NOTES protocols evaluating bacterial contamination concluded that the risk of bacterial contamination from TG access was clinically insignificant in humans. 26 Although still limited, data from human clinical series, trials, and registries also report no procedure-related risk of infectious complications after TG surgery.2,27–29 The primary fear of increased risk of infection from TG NOTES in humans is thus perhaps unsubstantial. 30 As a result, a Grade C recommendation based on Level 4 evidence has been proposed stating that no preoperative disinfection or preparation of the access way is required for the TG approach to the abdomen in humans. 3
The primary limitation with the present study was the lack of a power calculation. Also, the sample size was too small for any statistical analyses, and as such this study remained descriptive. To further evaluate the healing process a group with even longer follow-up could have been included. Another limitation was the use of the term pure NOTES. A Veress needle was used to control pneumoperitoneum, and as such the procedure was not “pure” NOTES in the strict definition of the term. Lastly, it has been proposed that a dog stomach has closer resemblance to the human stomach. 18 Although being a more expensive model, a dog model could thus perhaps be more appropriate for evaluating closure than the pig model.
In conclusion, the results regarding closure and healing supported the safe and reliable use of the OTSC System. EUS-guided access seemed safe, but refinement of the technique was necessary to increase reproducibility. Despite an intensive decontamination regimen, infections were still observed. Whether decontamination is needed in the human setting remains unknown, but the risk of infection seems minimal compared with that reported in animal models.
Footnotes
Acknowledgments
The authors acknowledge Olympus Corporation for supplying the endoscopic hardware necessary for this study and the EURO-NOTES Foundation, Toyota Foundation, Axel Muusfeldt Foundation, University of Copenhagen, The Research Council at Copenhagen University Hospital Herlev, and The Capital Region of Denmark, Foundation for Health Research for financial support.
Disclosure Statement
A.M.D., L.A., and O.L.N. declare no competing financial interests exist. S.M. has received consultancy honoraria from Boston Scientific and Coloplast Denmark and research support from Olympus Europa. L.N.J. has received a travel grant from Olympus and lecture fees from Covidien. J.R. has received payment for expert testimony from Baxter Healthcare, research support from Bard, Johnson & Johnson, and Baxter Healthcare, and payment for lectures by Merck and Bard. P.V. has received a consultancy honorarium from MediGlobe GmbH, Grassau, Germany and travel reimbursement from Olympus, Denmark.