
Abstract
Abstract
Background:
Diagnostic peritoneoscopy is typically performed by using a rigid laparoscope. Inspired by gastric submucosal tunneling for peritoneal natural orifice transluminal endoscopic surgery access and peroral endoscopic myotomy for the treatment of achalasia, we developed a novel esophago-cardial-gastric tunneling (ECGT) peritoneoscopy technique with a flexible endoscope. This study aims to evaluate its feasibility and safety.
Materials and Methods:
The study comprised 10 Beagle dogs. A longitudinal mucosal incision was made on the esophageal wall, and a submucosal tunnel was created through the cardia into the stomach. An incision was made in the muscular layer of the stomach, and then the endoscope was advanced into the peritoneal cavity. Peritoneoscopy with the flexible endoscope was performed. After intraperitoneal exploration, the esophageal mucosal entry was closed with endoclips. All dogs resumed food intake 12 hours after the procedures. Diets, behavior, and body temperature of all of the dogs were observed. Endoscopic examinations were performed 4 weeks after the procedure, and then the animals were sacrificed for necropsy.
Results:
The ECGT peritoneoscopy was successfully done in all dogs. Diets, behavior, and body temperature were normal in all dogs. The entry of the esophagus was healed well in 9 dogs; the mucosa of the entry was torn in 1 dog, but the submucosal tunnel was healed well at the cardia. Necropsy showed complete closure of the gastric serosal exit, and no intraperitoneal abscess was found. Histopathological examinations showed submucosal tunnels healed well.
Conclusions:
The ECGT peritoneoscopy is feasible and safe for peritoneal exploration. It should be a good choice for the clinical application of diagnostic peritoneoscopy.
Introduction
N
Recently, the gastric submucosal tunneling technique has been used for NOTES peritoneoscopy in animal models.7,8 However, the gastric submucosal tunneling had disadvantages such as the difficulty of in-line endoscope positioning, uncertain tunnel direction, and the infection risk of the gastric submucosal tunnel.9–11 Peroral endoscopic myotomy (POEM) has had good clinical results for the treatment of achalasia with the gastroesophageal submucosal tunneling technique, which has also been applied in endoscopic resection.12–15 We previously reported endoscopic resection of cardial subepithelial tumors originating from the deep muscularis propria by a POEM-like submucosal tunneling technique; the full-thickness muscularis propria defect was achieved after tumor removal sometimes through which we could observe intraperitoneal organs. 16 Inspired by the clinical practice, we designed the esophago-cardial-gastric tunneling (ECGT) access to enter the peritoneal cavity for peritoneoscopy and evaluated the feasibility and safety of this technique in a dog model.
Materials and Methods
Animals
Ten adult Beagle dogs (6 females, 4 males) were used in the study. The animals were fasted for 24 hours prior to the procedure. The study protocol was approved by the Animal Care and Use Committee at the Harbin Medical University (Harbin, People's Republic of China). Animals were housed at the Laboratory Animal Research Center at the Harbin Medical University.
Endoscopes and instruments
A standard gastroscope (model GIF-H260; Olympus, Tokyo, Japan) with a transparent hood attached to its tip was used during the procedure. Other equipment used included an insulated-tip knife (model KD-611L; Olympus), hook knife (model KD-620LR; Olympus), coagrasper (model FD-410LR; Olympus), injection needle (model NM-400L-0525; Olympus), endoclips (model HX-610-135 or HX-610-90; Olympus), clip fixing devices (model HX-5LR-1; Olympus), CO2 insufflator (model UCR; Olympus), and high-frequency generator (model ICC200; Erbe, Tübingen, Germany). The endoscope and all accessories were subjected to high-level disinfection and gas sterilization before use.
Procedure and technique
General anesthesia was induced by intramuscular injection of ketamine (100 mg) and diazepam (10 mg) and was maintained with 2% pentobarbital sodium. After endotracheal intubation, the esophagus and stomach were lavaged with sterile normal saline solution until free of gross food material. After evacuation of the irrigant, 200 mL of 10% povidone iodine solution was instilled, left in place for 10 minutes, and then aspirated.
Creation of submucosal tunnel
After a submucosal injection, a 2.0-cm longitudinal mucosal incision was made at the right wall of the esophagus approximately 5 cm proximal to the esophagogastric junction. Then, a submucosal tunnel was created downward, passing the cardia and extending 3–5 cm into the gastric submucosal space (Figs. 1A and 2A–C).
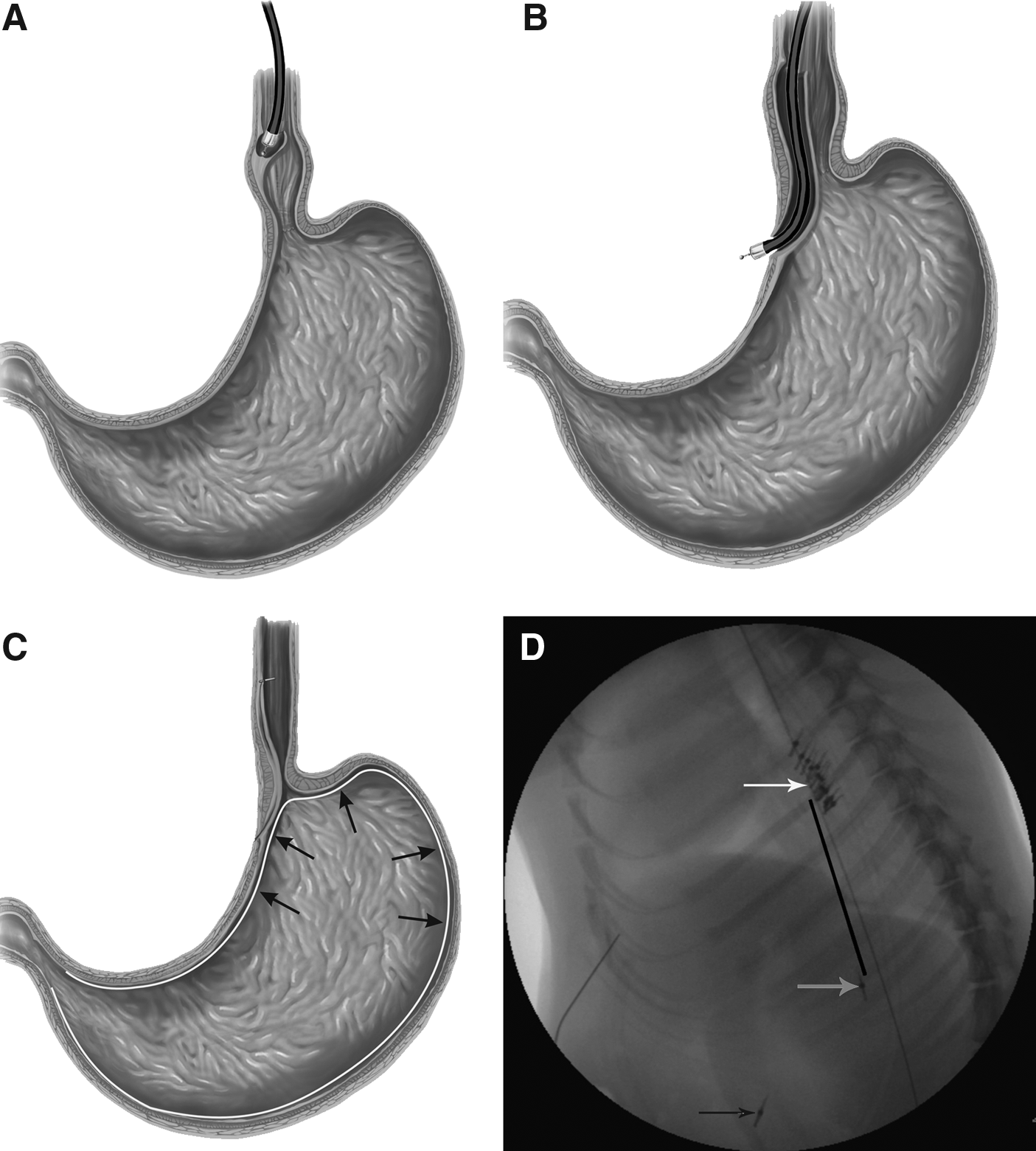
Diagram of esophago-cardial-gastric tunneling access.
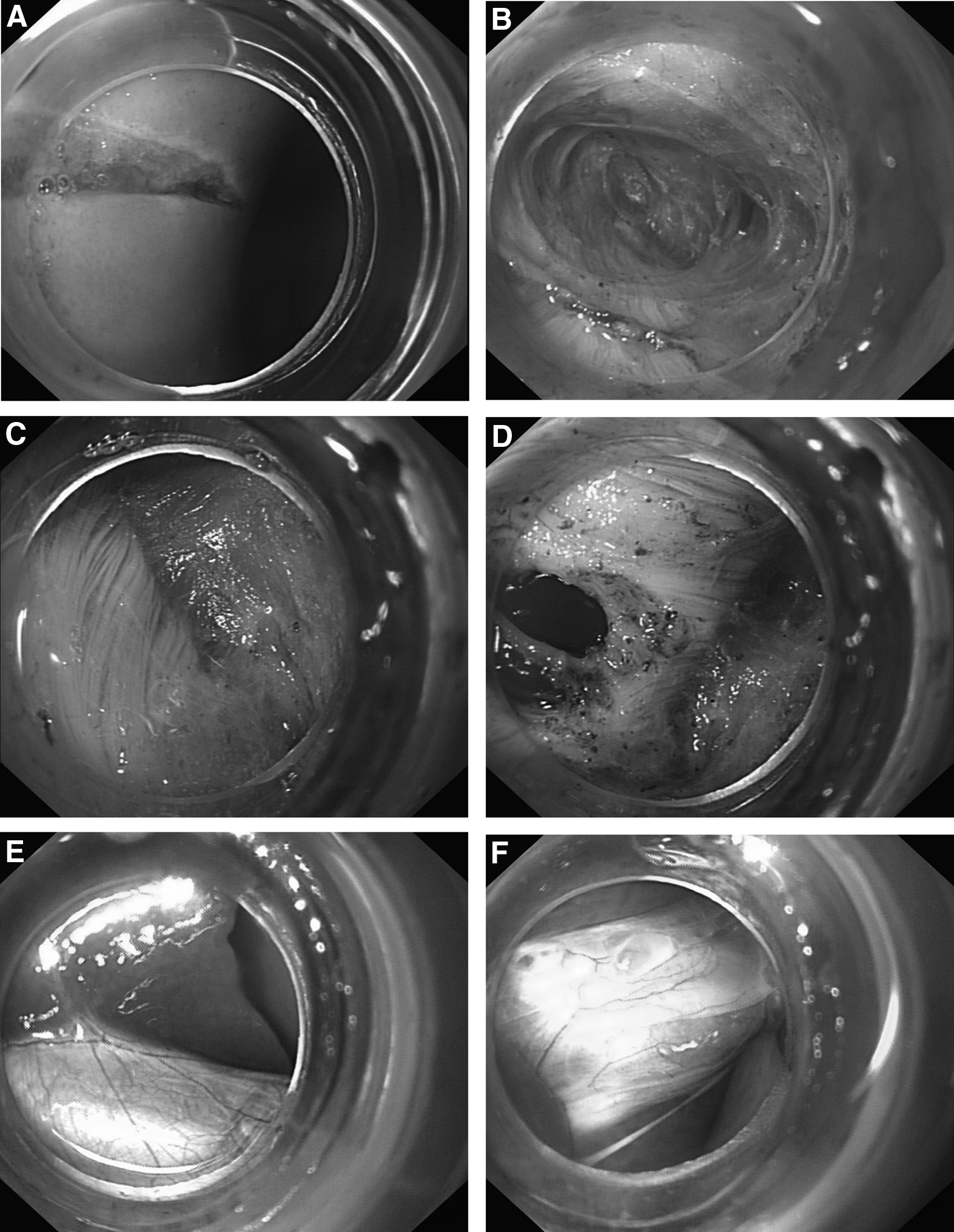
The esophago-cardial-gastric tunneling access technique.
Seromuscular incision of gastric wall
At the distal end of the submucosal tunnel, we incised the muscular layer of the gastric wall to the serosal layer and then made a blunt puncture into the peritoneal cavity with the insulated-tip knife. Then the incision was enlarged with the insulated-tip knife, allowing the endoscope to enter the peritoneal cavity (Figs. 1B and 2D).
Intraperitoneal exploration and closure of mucosal entry
The liver, gallbladder (Fig. 2E), cystic duct (Fig. 2F), spleen, bladder, uterus, and small and large intestines were observed and touched using a biopsy forceps. After intraperitoneal exploration, the esophageal mucosal entry was closed with endoclips (Figs. 1C and 2H). In the initial 4 dogs, the gastric exit sites and the greater curvature of the stomach were marked by endoclips (Fig. 2G), and X-ray fluoroscopy was performed for tracing the ECGT access track by introducing a guidewire (Figs. 1D and 2I)
Follow-up and necropsy
Liquid diets were given the morning after the procedure, and soft diets were resumed the next day. Behavior and food intake were observed. Body temperature was checked twice daily. Follow-up endoscopy was performed to assess the healing of the esophageal mucosal entry after the 4-week survival period, and then the dogs were euthanized. The peritoneal cavity was examined for signs of organ injury, bleeding, or abscess. The gastric serosal incision site was assessed by gross examination. The tissue between the esophageal entry and gastric exit was resected for microscopic histopathologic examination.
Results
The abdominal cavity was successfully entered in all 10 dogs. No complications such as severe bleeding and/or mucosal injury occurred during the procedure. The esophageal mucosal entry site was successfully closed with endoclips in all cases. In the initial 4 dogs the ECGT access track was shown to be straight on plain radiographs (Fig. 1D). Contrast radiography showed that the gastric wall incision site was located on the less curvature of the proximal stomach (Fig. 2I). All dogs recovered well without any signs of infection. Diets, behavior, and body temperature were normal after the procedures in all dogs.
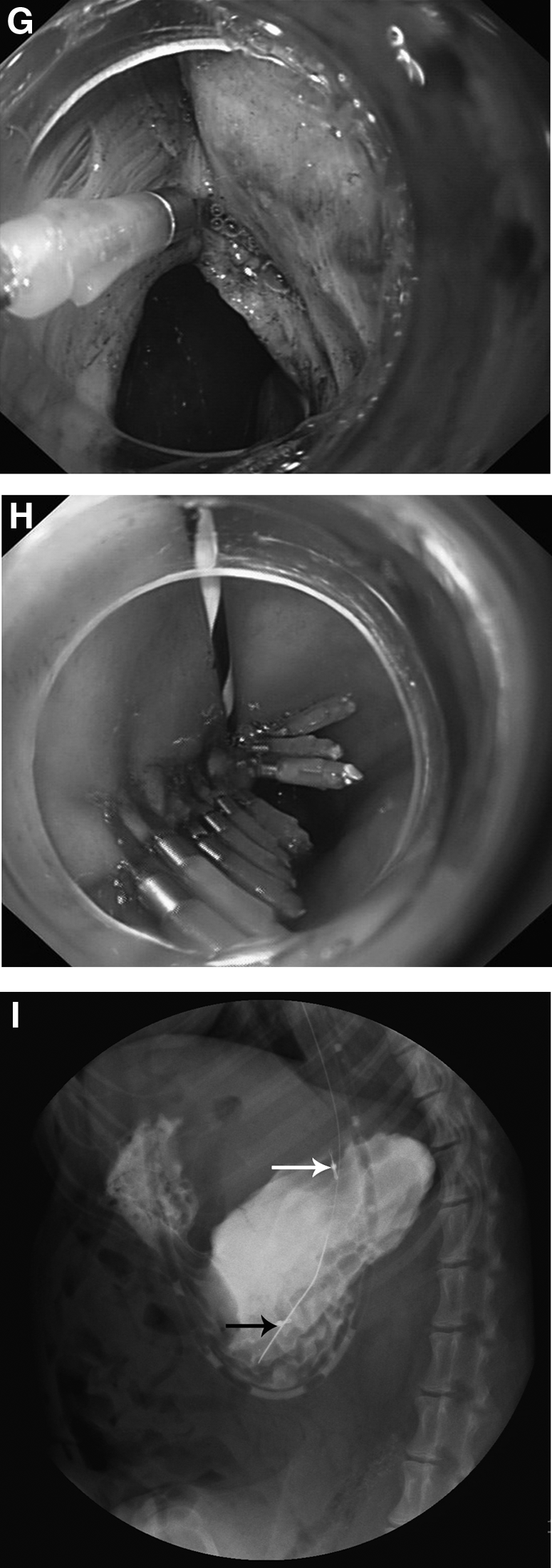
Follow-up endoscopy showed mucosal healing (Fig. 3A) of the esophageal mucosal entry in 9 dogs, and mucosal tearing occurred in 1 dog, but the submucosal tunnel was healed well at the cardia (Fig. 3B). The mucosa of the gastric fundus remained intact (Fig. 3C). Necropsy revealed no evidence of organ injury, intraabdominal hemorrhage, or abscess, therefore confirming the closure of the gastric serosal exit (Fig. 3D). The microscopic histopathologic examination showed excellent healing of the fibrous scar in the esophageal submucosal tunnel and the collagen fibers at the gastric seromuscular incision site.
The follow-up endoscopic findings in postoperative Week 4.
Discussion
In the past, diagnostic peritoneoscopy was often performed with a rigid laparoscope. With the development of the NOTES technique, NOTES peritoneoscopy with a flexible endoscope has been reported. Feasibility has been already demonstrated in several human case series.17,18 The peroral transgastric route is frequently used as an access to the peritoneal cavity due to the fact that the transvaginal approach only applies to women and the transcolonic approach might lead to a severe bacterial load in the peritoneal cavity.19,20 However, it was previously reported that the gastrostomy site of the transgastric access had a relatively weak leak resistance, even though it was closed under endoscopy. 21 It is necessary to fast for several days after the procedure because the stomach is a food-storing organ. Gastric submucosal tunneling is another technique for transgastric peritoneal access developed by Sumiyama et al. 22 Although the leak resistance was enhanced due to malpositioning between the mucosal entrance and the serosal exit of the tunnel, there were inherent disadvantages, such as the relatively difficult creation, uncertain tunnel direction, the difficulty of in-line endoscope positioning, and the infection risk of the submucosal tunnel.9–11
Recently, the technique of POEM for esophageal achalasia has shown promising results in clinical application. During the POEM procedure, a submucosal tunnel is created from the esophagus to the stomach via the cardia. Creating this tunnel is easy and safe, and the tunnel is straight. Inspired by this, we examined whether this submucosal tunnel could also be used as a peritoneal access for NOTES peritoneoscopy. Our present study has demonstrated, in a dog survival model, the feasibility and safety of the ECGT access to the peritoneal cavity.
The advantages include that the ECGT access keeps in line with the esophagus and the lesser curvature of the proximal stomach. We can create the ECGT access easily just like in the POEM procedure. In the initial 4 dogs, the submucosal tunnel exits were marked by endoclips. The plain radiographs showed that the ECGT access was straight, which avoided the mechanical limitations during creation of the gastric submucosal tunnel.
Otherwise, the ECGT access passes the esophagogastric junction where the lower esophageal sphincter is usually contractive. The contraction of the lower esophageal sphincter may accelerate the adherence of the mucosa to the underlying muscular layer, which promotes the healing of the submucosal tunnel. Previous experimental studies showed that the submucosal void might provide an excellent environment for bacterial growth, which led to abscess formation. 11 In our study, submucosal abscess was not noted in any of the animals. Although mucosal tearing was found in 1 dog, the submucosal tunnel near the cardia was completely healed without infection or fistula formation. It was consistent with our notion that lower esophageal sphincter contraction may contribute to a safe and reliable closure of the ECGT peritoneal access.
Another advantage of ECGT access is that the gastric mucosa is kept intact, not requiring any meal restrictions after the procedure. In our study, all animals took food on the next morning when recovered from the anesthesia without abnormalities. The storage function of the stomach was preserved effectively. Although the esophageal mucosa was incised as a tunnel entrance, it could be closed easily by endoclips. The entry site and the gastric exit site are separated by lower esophageal sphincter contraction, which can avoid fistula formation. Above all, these results suggest that the ECGT access might be more secure than prior methods to access the peritoneal cavity.
The limitations of this study include the small number of animals and that it was an uncontrolled study. Further control studies will be required. The other limitation of the ECGT access is that the tunnel diameter often is less than 2 cm. This means that it will be difficult to extract a larger specimen via the ECGT access. However, it can be used to perform peritoneoscopy, peritoneal biopsy, and some NOTES drainage with and without closure of an intraabdominal organ.
In conclusion, the ECGT approach is technically feasible and provides safe peritoneal access. The ECGT peritoneal access may be a promising technique for diagnostic peritoneoscopy.
Footnotes
Acknowledgments
This work was supported by grant ZD2008-09 from The Science Foundation of The Second Affiliated Hospital of Harbin Medical University. We would like to express our gratitude to all those who helped us during this study. A special acknowledgement should be shown to Prof. David Y. Graham and Dr. Sergey Kantsevoy, who gave us great encouragement and assisted in revising this article.
Disclosure Statement
No competing financial interests exist.