
Abstract
Abstract
Background:
The manual dexterity of a surgeon is known to be related with surgical proficiency. Recently, as an objective measurement of surgical skills, inanimate methods using several types of simulators have been introduced. Using these simulators, we aimed to investigate the impact of manual dexterity on laparoscopic and robotic surgical proficiency.
Materials and Methods:
Fellow surgeons, surgical residents, and medical students (n = 32) participated in this study. For the measurement of dexterity, the sums and differences of the right and left hand performance times for the Grooved Pegboard Test were used as an index of dexterity speed and ambidexterity, respectively. The performance times during three sessions of laparoscopic suturing using a D-box trainer and the performance scores during three sessions using two robotic suturing programs with different degrees of difficulty provided by the da Vinci® Skills Simulator™ (Intuitive Surgical Inc., Sunnyvale, CA) were analyzed according to the measured manual dexterity.
Results:
Manual dexterity was not a significant factor for performance time during laparoscopic suturing, which was more influenced by participants' surgical experiences. In robotic suturing, the performance score was impacted significantly by manual dexterity in terms of ambidexterity rather than dexterity speed. For an easy robotic suturing task, the gap of proficiency between the lower and higher ambidexterity groups was decreased successively with each of the three sessions. However, that gap in cases with a difficult task was maintained consistently throughout all three sessions.
Conclusions:
The degree of ambidexterity was an initial predictor for proficiency with simulated robotic suture. However, this relation could be lessened through a few sessions of training, although for a more difficult task further repetitions would be needed.
Introduction
L
The innate dexterity of the surgeon in relation to education and skill training in the surgical field has been evaluated in several previous studies.6–8 One previous study reported that a medical student's innate manual dexterities, as measured by the Purdue Pegboard Test, were predictive of his or her initial surgical suturing performance. 6 Another study reported that the relationship between a medical student's innate manual dexterity and the quality of his or her performance of a small bowel anastomosis was significant only at the initial phase and that this relationship disappeared after a period of training. 7
With regard to the actual mechanisms of manual dexterity, the ability to use both the dominant and nondominant hand, in other words, ambidexterity, has been assumed to have an association with surgical proficiency because surgical tasks usually require simultaneous movements of both arms in a specific relationship.8,9 Previous studies have reported that the degree of ambidexterity in task performance increased with overall task performance improvement and that ambidexterity provides an indication of the level of proficiency for surgical skills.8,9
Accordingly, for the objective and quantified measurement of the level of proficiency for surgical skills, the use of several types of simulators has been introduced.10–14 These simulators have demonstrated construct validity,15–17 and the psychomotor skills assessed with these simulators have been shown to correlate with actual performance in the operating room. 11 Among the several simulated tasks, we adopted the suturing task, which is one of the more difficult and complex exercises and therefore can clearly reveal the proficiency of participants.18,19 In the current study, we used laparoscopic and robotic simulators to measure the suturing proficiency for these two types of surgery and analyzed these findings in relation to the operator's innate manual dexterity assessed by the Grooved Pegboard Test.
Materials and Methods
Fifteen fellow surgeons, 13 surgical residents, and 4 medical students participated in this Institutional Review Board–approved (H-1410-126-620) study after informed consent was obtained. The participants had various levels of laparoscopic experience, but none had any prior robotic surgery or simulator experience. Additionally, none had previously been exposed to the Grooved Pegboard Test, which measures innate manual dexterities of all participants. In this study, “status” was defined as fellow, resident, or student. All participants claimed to be right handed for writing, 20 and all took the Edinburgh Handedness Inventory 21 to assess the degree of handedness, calculated on a Likert-scale format that has been generally used since this inventory was trialed. 22 In this inventory, a calculated score of −100 corresponds to complete left handedness, and a score of +100 corresponds to complete right handedness.
After completing the Edinburgh Handedness Inventory, each participant performed the Grooved Pegboard Test using the standard grooved pegboard apparatus (Lafayette Instrument Co., Lafayette, IN). This apparatus consists of a 5 × 5 matrix of keyhole-shaped holes in varying orientations and key-shaped pegs. 23 To perform this task, the pegs must be finely rotated into position for correct insertion. 23 This was first performed with the right hand, and subsequently with the left hand. This was then repeated once, in the same order. The performance times recorded for the two sessions for each hand were added and were designated as Peg Right and Peg Left. We then calculated the sum (Peg Sum) and difference (Peg Diff) of Peg Right and Peg Left. Therefore, Peg Sum is the sum of manual dexterity speed for both hands, with a lower value corresponding to a faster performance. Peg Diff reflects the degree of ambidexterity; a lower value means that the dexterity of the left hand is comparable to that of the right hand. If the left hand performance was faster than the right hand performance, the Peg Diff value would be a negative number.
For the measurement of laparoscopic surgical skills, a D-box equipped with a miniature camera and a skin-model pad for suturing was used. Several holes in the side walls of the D-box enabled the operators to insert laparoscopic instruments and perform suturing on the model pad, and they simultaneously viewed a monitor that was connected to the miniature camera. Participants executed two simple sutures, first with the right and then with the left hand. This was repeated three times, consecutively. The performance time of both hands was assessed at each of the three trials. The summed performance time was used later in the analysis to define laparoscopic competence in the robotic suturing trials.
For the measurement of robotic surgical skills the da Vinci® Skills Simulator™ (Intuitive Surgical), consisting of a da Vinci SI Surgeon Console and an integrated backpack unit with Mimic virtual reality software (Mimic Technologies, Inc., Seattle, WA), was used. This platform redirects the operator's manipulation of the master controller in the console to a movement of the virtual robotic instruments in a computer-generated environment. 16
Initially, participants received a basic orientation regarding how to operate the master controller in the console, including camera and clutch use from an investigator who also taught the two simple simulation tasks (Pick and Place, Camera Targeting). After completing these two simple tasks, participants undertook two virtual reality suturing programs, one easy (Dots and Needles, Level 1) and the other difficult (Suture Sponge, Level 3). Participants repeated the suturing programs four times. During the first round, the investigator explained how to perform the task in detail, and the first score was not included in the subsequent analysis. The simulator performance score was recorded based on eight specific metrics: time to completion, economy of motion, instrument collision, needle drop, instruments out of view, excessive instrument force, master controller range, and number of missed targets. Subsequently, the algorithm developed by Mimic Technologies converted these individual metric units into percentage scores and assigned each individual metric a weight of 1.0, except the master controller range, which was assigned a weight of 0.2 for calculating the overall score. 16
Statistical analysis was performed using SPSS version 20.0 software (SPSS Inc., Chicago, IL). The association between the participants' factors was examined using the chi-squared test. The effect of each consecutive session and participants' factors on performance times or score was analyzed using mixed repeated-measures analysis of variance. If there was no significant interaction between the effects of each consecutive session and the participants' factors on performance time or score, simple main effects of these variables was evaluated with the paired t test and the independent t test, respectively. A P value of < .05 (two-sided) was considered significant.
Results
The characteristics of the 32 participants are presented in Table 1. All participants were right-handed, and none of their Edinburgh Handedness Inventory scores were less than 0 (median value, 90.0; range, 0–100). The median total time required to complete two sessions of the Grooved Pegboard Test with the right hand (Peg Right) and left hand (Peg Left) was 111.5 seconds and 123.0 seconds, respectively. The median calculated sum (Peg Sum) and difference (Peg Diff) of Peg Right and Peg Left were 231.5 seconds and 11.5 seconds, respectively. Based on these median values, participants with Peg Sum ≤231 seconds were considered to have higher dexterity speed, whereas those with Peg Sum >231 seconds were considered to have lower dexterity speed. Also, participants with a Peg Diff ≤11 seconds were considered to have higher ambidexterity, whereas those with Peg Diff >11 seconds were considered to have lower ambidexterity. These groups categorized for dexterity speed and ambidexterity were not distributed differently among the participants' status (Table 2). There was also no relationship between gender and status. Predictably, the proportion of participants >31 years of age was significantly higher in fellows, compared with residents or students (P = .003).
Peg Diff, difference of Grooved Pegboard Test performance times for both hands; Peg Left, sum of performance times recorded for two sessions with the left hand; Peg Right, sum of performance times recorded for two sessions with the right hand; Peg Sum, Sum of Grooved Pegboard Test performance times for both hands.
By chi-squared test.
Peg Diff, difference of Grooved Pegboard Test performance times for both hands; Peg Sum, sum of Grooved Pegboard Test performance times for both hands.
The trends for performance times over the three sessions of laparoscopic suturing according to the participants' status, degree of dexterity speed, and ambidexterity are presented in Figure 1 and Table 3. There was no significant interaction between any of these three factors and session number for the effects on performance time (P = .164, P = .324, and P = .159, respectively, by mixed repeated-measures analysis of variance). Regarding the main effects, participants' status was a significant factor (P = .016), in that fellows performed faster than residents (P = .012 by post hoc test using Tukey's correction). Also, the medical students appeared to have performed better than the residents; however, their apparent difference was not statistically significant (P = .717 by post hoc test using Tukey's correction). The session number was also significant (P = .000), in that performance time decreased consecutively throughout the three sessions. This was confirmed by post hoc test using Bonferroni's correction. The participants with higher dexterity speed or ambidexterity demonstrated a tendency for a shorter performance time; however, this association was not statistically significant.
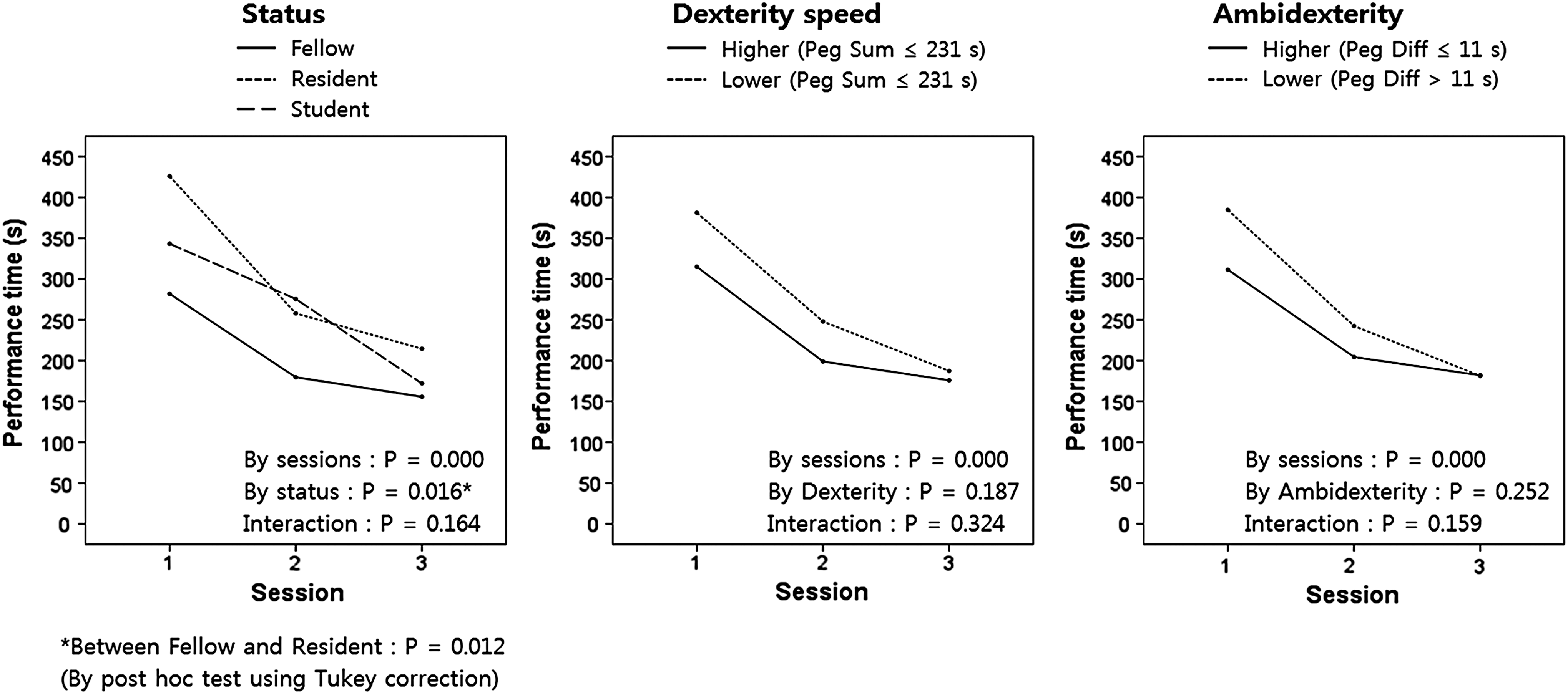
Trends of performance times over three sessions of laparoscopic suturing according to the participants' status, dexterity speed, and ambidexterity. *Between fellow and resident, P = .012 by post hoc test using Tukey's correction. Peg Diff, difference of Grooved Pegboard Test performance times for both hands; Peg Sum, sum of Grooved Pegboard Test performance times for both hands.
Data are mean (standard deviation) values.
Repeated-measures analysis of variance with Bonferroni's correction.
Repeated-measures analysis of variance (with Tukey's correction in analysis regarding status).
Peg Diff, difference of Grooved Pegboard Test performance times for both hands; Peg Sum, sum of Grooved Pegboard Test performance times for both hands.
The overall scores of three consecutive sessions performing the two robotic suturing tasks of different difficulty according to the participants' status, laparoscopic competence, degree of dexterity speed, and ambidexterity are presented in Figure 2 and Tables 4 and 5. Laparoscopic competence, one of the parameters for robotic suturing proficiency, was defined by the median value of the participants' summed up performance times in the three laparoscopic suturing sessions, and the median value was 736 seconds (Tables 4 and 5). Based on this definition, participants with a cumulative time of ≤736 seconds were considered to have higher laparoscopic competence, and those with a cumulative time of >736 seconds were considered to have a lower laparoscopic competence. As shown in Figure 2, the trends for the overall score over three sessions showed successive improvement in both the easy and difficult robotic suturing tasks; however, post hoc analysis using Bonferroni's correction revealed that this improvement was only significant between sessions 1 and 3 of the easy task (Table 4), as opposed to laparoscopic suturing where the performance time decreased consecutively through all three sessions. In the difficult robotic suturing task, the improvement between sessions 1 and 3 was not statistically significant (P > .05) (Table 5).
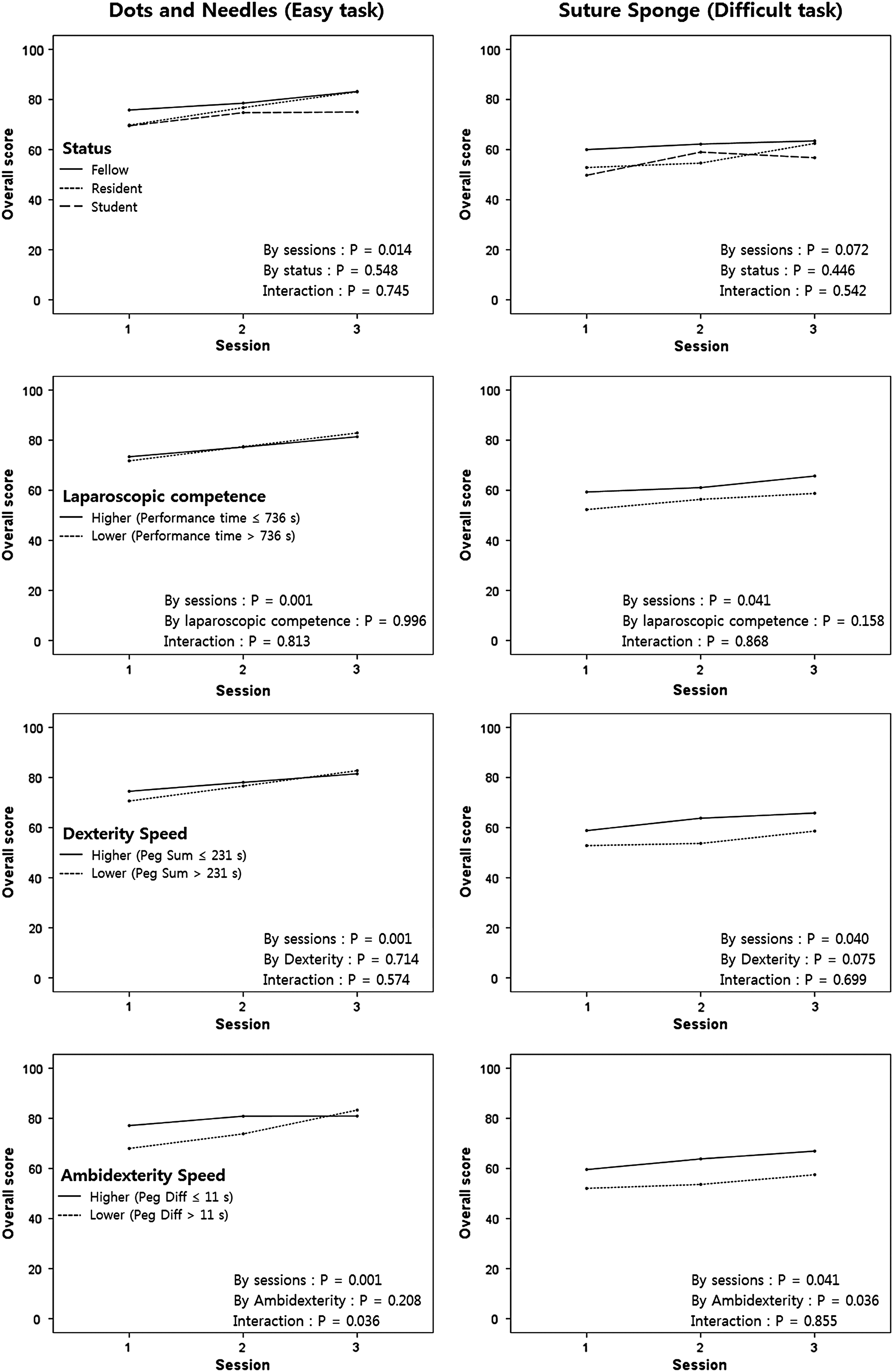
Trends of overall scores over three sessions of two robotic suturing tasks with different difficulty according to the participants' status, laparoscopic competence, dexterity speed, and ambidexterity. Peg Diff, difference of Grooved Pegboard Test performance times for both hands; Peg Sum, sum of Grooved Pegboard Test performance times for both hands.
Data are mean (standard deviation) values. Laparoscopic competence was determined as high or low using the median value of the laparoscopic suture performance time over three sessions as the cutoff value (736 seconds).
Repeated-measures analysis of variance with Bonferroni's correction (except analysis regarding ambidexterity).
By paired t test.
By independent t test.
Peg Diff, difference of Grooved Pegboard Test performance times for both hands; Peg Sum, sum of Grooved Pegboard Test performance times for both hands.
Data are mean (standard deviation) values. Laparoscopic competence was determined as high or low using the median value of the laparoscopic suture performance time over three sessions as the cutoff value (736 seconds).
Repeated-measures analysis of variance with Bonferroni's correction.
Peg Diff, difference of Grooved Pegboard Test performance times for both hands; Peg Sum, sum of Grooved Pegboard Test performance times for both hands.
In the easy robotic suturing task, there was a significant interaction between the effects of ambidexterity and session number on the performance score (P = .036, by mixed repeated-measures analysis of variance) (Fig. 2). Participants with higher ambidexterity achieved better scores than those with lower ambidexterity in session 1 (P = .070); however, this difference was not apparent in session 3 (P = .589) (Table 4). Also, in participants with higher ambidexterity, the score improvement from sessions 1 to 3 (P = .165) was not significant; however, those with lower ambidexterity achieved significant improvement in their score from session 1 to 3 (P = .000) (Table 4). This interaction indicates that participants with lower ambidexterity had steeper learning curves than those with higher ambidexterity. Other than ambidexterity, there was no interaction between the participants' factors and session number for the effects on the performance score of the easy task. The main effects of the participants' status, laparoscopic competence, and dexterity speed on the easy task performance score were not significant as shown in Figure 2.
In the difficult robotic suturing task, there was no significant interaction between the participants' factors and session number for the effects on the performance score (Fig. 2). Regarding the main effects, participants with higher ambidexterity achieved better scores than those with lower ambidexterity over the three sessions (P = .036). In contrast to what was seen with the easy task, the difference in scores in terms of ambidexterity was maintained throughout the three consecutive sessions. Participants with higher laparoscopic competence or dexterity speed also showed a tendency to achieve a better score; however, these associations were not significant (P = .158 and P = .075, respectively).
Ambidexterity was a significant factor regarding interaction with session number for the effects on the performance score in the easy task. Additionally, ambidexterity was a significant factor regarding main effect in the difficult task. We further examined the individual composite metric scores, in addition to the overall scores, according to the ambidexterity (Fig. 3). We found that some of these metrics including time to completion, economy of motion, and missed target rate displayed the concurrent features with overall score. In the easy task, the gaps of scores from these metrics between the lower and higher ambidexterity groups were decreased successively through the three sessions, whereas those gaps in the difficult task were maintained consistently over the three sessions, although some of these findings were not statistically significant.
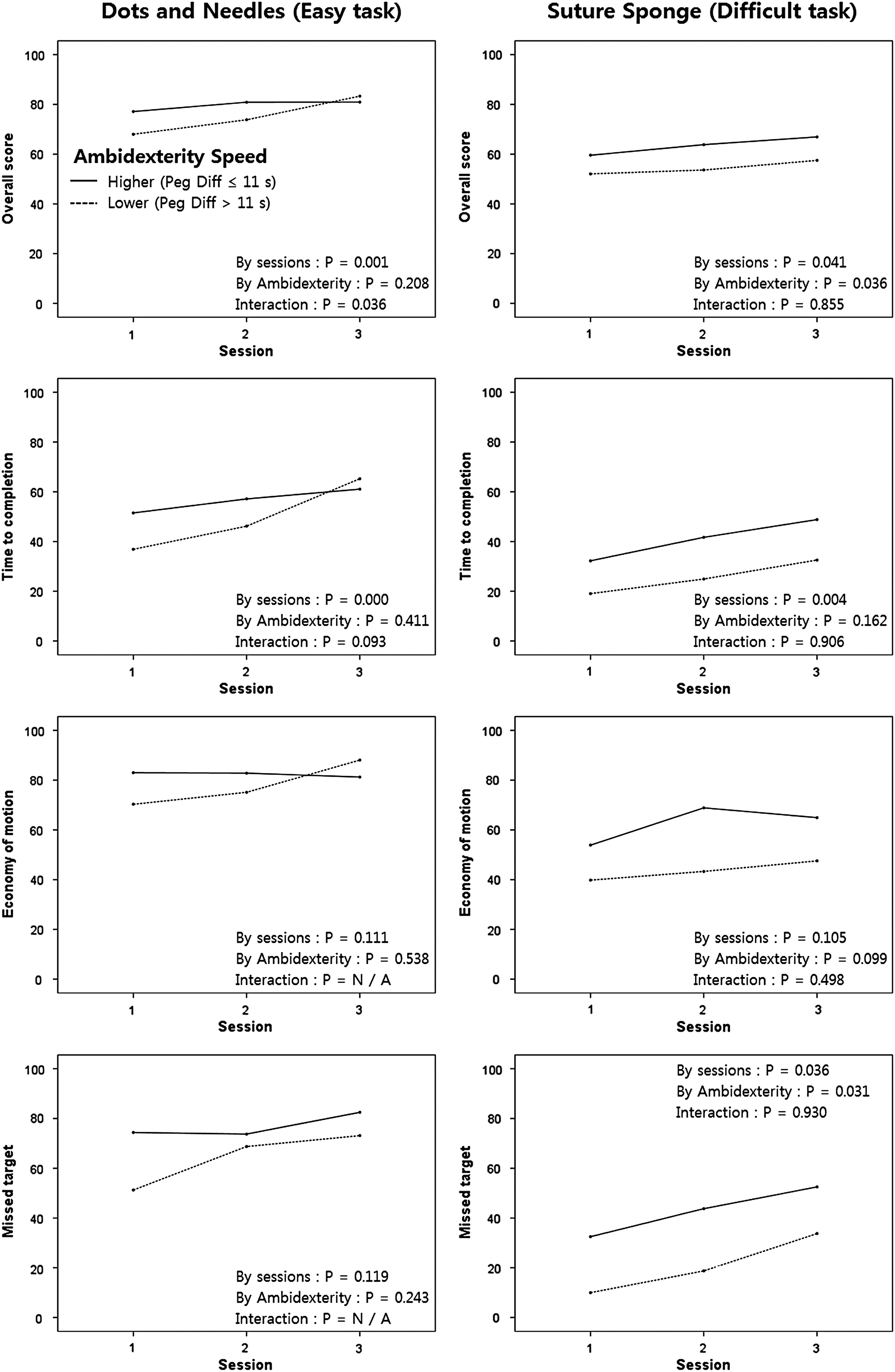
Trends of overall and composite metrics scores over three sessions of two robotic suturing tasks with different difficulty according to the participants' ambidexterity.
Discussion
Surgical suturing requires three-dimensional manipulation and fine bimanual coordination to even simply grab the needle and pierce the tissue. 7 In this study, we used the suturing skill as an indicator of surgical proficiency; however, actual surgical proficiency cannot be estimated by just suturing skill. The reason we chose suture among the other surgical performances was that this skill had been steadily investigated through previous studies6–8 for the relationship with bimanual dexterity and coordination. In this study, the performance time for simulated laparoscopic suturing appeared to be shorter in participants with higher dexterity speed and ambidexterity, although this was not statistically significant. This lack of statistical significance in relation to manual dexterity may be due to the varied levels of laparoscopic experiences of the participants in the study. Indeed, the performance time for laparoscopic suturing was influenced by the participants' status (fellow surgeons or residents), which reflected their cumulative laparoscopic experiences and skills.
On the other hand, the participants in this study had no prior experiences of robotic surgery or simulator. Therefore, their manual dexterity could be shown to be a significant factor in the performance of robotic suturing. Specifically, ambidexterity was demonstrated to be more significantly related to performance than the dexterity speed of both hands. In further detail, the dexterity speed and ambidexterity of the participants in our study were mutually associated (P = .034; data not shown). We assumed that this association might explain the tendency of better score with robotic suturing (difficult task) in the participants with higher dexterity speed, as well as in those with higher ambidexterity. However, this tendency of relation between score and dexterity speed was not statistically significant (P = .075), whereas the relation between score and ambidexterity was significant (P = .036) as described above. This was because the participants with higher ambidexterity but lower dexterity speed performed better than those with lower ambidexterity but higher dexterity speed. Also, this means that the scores of robotic suture were better explained by ambidexterity, rather than dexterity speed. These findings concur with those of Narazaki et al., 9 who reported that robotic surgery experts performed the surgical tasks with higher bimanual dexterity than novices and that the degree of bimanual coordination could be an objective criterion for proficiency in robotic surgical skills.
Meanwhile, there have been several studies regarding the influence of the robotic system on the operator's ambidexterity. It was reported that the da Vinci robotic system could overcome innate hand dominance among novice surgical trainees.4,24 Bocci et al. 25 reported that bimanual object manipulation is mediated by callosal fibers that interconnect the cerebral hemispheres, and there was a preferential activation of this human “mirror” system in surgeons operating with the robotic system compared with those performing conventional laparoscopy. These reports have suggested that because of the enhanced ambidexterity with the robotic system, the degree of an operator's innate ambidexterity might be less important in robotic surgery. However, the enhancement of ambidexterity with the robotic system does not exclusively occur in participants with lower baseline ambidexterity, but also in those with higher baseline ambidexterity. As demonstrated in our study, the gap of proficiency between the lower and higher ambidexterity groups was not decreased in spite of several repetitive trainings, especially for the difficult robotic surgical task.
In this regard, Kourtis et al. 26 reported that participants with a consistent hand preference were slower in initiating more difficult asymmetrical bimanual movements than symmetrical movements. However, participants with an inconsistent hand preference initiated symmetrical and asymmetrical movements with equal speed. Similarly, Judge and Stirling 27 reported that for left handers, there is a smaller performance difference between the two hands, and these left handers performed significantly better on an assembly task that was more difficult than the other tasks in their study. These studies have commonly suggested that the degree of ambidexterity is more significantly related to the performance of a difficult task rather than an easy task. In our study the difference in the performance score associated with ambidexterity became successively less in performing the easy task with each of the three sessions. However, in performing the difficult task, this difference in performance scores was maintained throughout all three sessions. This means that the challenges associated with ambidexterity cannot be fully overcome in performing relatively difficult tasks in robotic surgery through a few sessions of trainings during the early adaptation period, although this gap associated with ambidexterity might be overcome by the more sessions of trainings in late phase.
There have been several studies regarding specific training of the nondominant hand for improving surgical proficiency. Nieboer et al. 28 reported that specific training of the nondominant upper extremity, using handwriting, drawing lines in a labyrinth, and cutting paper, leads to improved skills on the dominant side, a phenomenon known as the intermanual transfer of skill learning. These authors suggested that bimanual training might be important for improving laparoscopic surgical skills. Middleton et al. 29 reported that nondominant hand performance on a laparoscopic virtual reality simulator was improved after short-term playing of the Nintendo (Kyoto, Japan) Wii™ video game system. This study suggested that ambidexterity could be developed with appropriate training of the nondominant hand.
Other than manual dexterity, laparoscopic competence measured by the performance time for laparoscopic suturing was not a significant factor for the proficiency of robotic suturing in our study. However, Hagen et al. 30 reported that robotic performance significantly correlated with laparoscopic experience. Their results, which are contrary to ours, may be because the participants of their study were categorized definitely into two groups: a novice group with no laparoscopic training and a laparoscopically trained surgeon group. However, the participants of our study could not be clearly divided into two groups in terms of laparoscopic competency; therefore, we used the median value of laparoscopic suturing time in our study as a cutoff point. In spite of this arbitrary grouping of our study participants, laparoscopic experience showed a tendency to impact the performance of robotic surgery especially in the difficult task, although this was not statistically significant (Fig. 2). This skill transfer phenomenon from laparoscopic to robotic surgery has been suggested in other previous studies.31,32 Stefanidis et al. 31 reported that experienced laparoscopists performed robotic surgery better than novices, and Zorn et al. 32 reported that the robot-assisted radical prostatectomy learning curve for a fellowship-trained general laparoscopic surgeon with limited experience in radical prostatectomy was similar to that of a laparoscopically naive yet experienced practitioner of open radical prostatectomy.
Our study has several limitations. First, the participants attempted each task only three times. Therefore, in the easy robotic suturing task, the participants with lower ambidexterity improved to the level of those with higher ambidexterity in their second and third attempts. However, with the difficult task, these relatively few repetitions were not sufficient to allow those with lower ambidexterity to overcome the score gap associated with ambidexterity.
Second, in the current study, during simulated robotic suturing, eight composite metrics and their overall scores measured by the da Vinci Skills Simulator were analyzed. However, for laparoscopic suturing using the D-box, performance time was the only parameter measured. Because of this imbalance in measured parameters between the laparoscopic and robotic simulators, it is difficult to fully compare one with the other. Therefore, our results showing no significant association of dexterity with laparoscopic suturing may not have been caused completely by our participants' varied amounts of laparoscopic experiences, as noted above. Our ability to collect one relatively simple parameter—performance time—for the measurement of laparoscopic proficiency compared with the robotic simulator score with multiple composite metrics may have also contributed to this finding.
Actually, a closer view revealed that dexterity speed and ambidexterity had a tendency to impact the performance time for laparoscopic suturing, as shown in Table 3 and Fig. 1, although this was not statistically significant (P = .187 and P = .252, respectively). Likewise, in robotic suturing, the statistical significance found for impact of ambidexterity on overall score was not attained when analyzed on performance time, individually, as one of the composite metrics scores (Fig. 3).
Gallagher et al. 33 suggested that only performance time analyzed as an independent variable would be at best, a crude, and at worst, a dangerous metric. Integration with other metrics like economy of motion and error rate would be necessary.
An integrated assessment, such as this, could be well provided by a simulator using a virtual-reality platform with its fine discriminative capabilities. We suppose that such integrated assessments could reveal the significant impact of ambidexterity on the laparoscopic proficiency, as demonstrated in other studies.8,25,34
In conclusion, the degree of ambidexterity measured by the Grooved Pegboard Test was a significant factor for proficiency with simulated robotic suture during the initial course of skill acquisition. However, the gap of proficiency associated with ambidexterity could be lessened through a few sessions of training, although for a more difficult task, more numbers of repetitions would be needed.
Footnotes
Disclosure Statement
No competing financial interests exist.