
Abstract
Abstract
Secondary prevention of colorectal cancer relies on effective screening through colonoscopy and polypectomy. Resection of some polyps can present technical challenges particularly when polyps are large, flat, or behind colonic folds. Laparoscopy as an adjunct to endoscopy can aid in removing difficult colonic polyps without subjecting patients to radical segmental colectomy. Hybrid laparoendoscopic techniques are increasingly reported in literature as alternatives to segmental colectomy for the treatment of polyps that have a high likelihood of being benign. Laparoscopic-assisted colonoscopic polypectomy is the most frequently utilized technique; it harnesses the power of laparoscopy to aid endoscopic polypectomy by flattening folds, mobilizing flexures, and providing retraction. Colonoscopy-assisted laparoscopic wedge and transluminal resection are often reported in older studies and use the visualization provided by intraoperative colonoscopy to guide colonic resection that is limited to the area of the polyp. Laparoscopic-assisted endoscopic full-thickness resection (EFTR) is a relatively recent technique that provides laparoscopic monitoring of EFTR of polyp as well as endoscopic closure of the ensuing defect. Minimally invasive segmental colectomy based on oncologic principles should be utilized when none of the previous techniques are suitable or when malignancy is strongly suspected. The combined use of laparoscopy and endoscopy can expand the endoscopist's armamentarium when dealing with the most challenging polyps, while serving the patients' best interest by limiting the extent of colon resection.
Introduction
C
There is now ample evidence to support oncologic equivalence as well as improved patient outcomes after laparoscopic segmental colectomy, making this the optimal approach for colon cancer resection in appropriately selected patients. 7 Advantages of laparoscopic surgery over open resection include less blood loss, improved pulmonary function, earlier return of bowel function, decreased postoperative hospital stay, and improved quality of life. 8 Although randomized trials have reported conversion rates ranging from 17% to 29% for colon cancer cases,9,10 this number is much lower for surgical resection of polyps since issues with bulk and invasion into adjacent organs are less likely. Reported conversion rates for laparoscopic colectomy done specifically for unresectable polyps in retrospective data can be as low as 3.2%. 11
The use of laparoscopy assistance in dealing with polyps is usually a last resort maneuver when all other options are exhausted. With improved endoscopic training, tools, and techniques such as EMR and endoscopic submucosal dissection (ESD), only a minority of polyps should require the assistance of laparoscopy. The mortality associated with laparoscopic colon resection is about 1% and overall morbidity about 18%. 8 Rates of wound infection can be quite variable and center dependent, but are estimated at about 6%, 12 which is likely an underestimate of the true numbers. However, when considering the risks and benefits of laparoscopic surgery versus endoscopic treatment, one has to keep in mind that the overall risk of endoscopic treatment for the difficult polyp is higher than the usual risk quoted to patients. For example, the risk of perforation associated with ESD in expert hands can be as high as 2.7%, 13 which is much higher than the 1 in 1400–3000 risk for screening colonoscopy and the 1 in 1000 risk for therapeutic colonoscopy. 14 The risk of complications is higher for endoscopists with lower experience of less than 50 ESDs. 13 There is great enthusiasm among some endoscopists for pushing the envelope and using repeat colonoscopy and EMR for lesions that are initially deemed unresectable. Even in expert hands, however, there is a recurrence rate of up to 50% when these lesions are successfully removed by EMR. 5 From the perspective of the patient, the assistance of laparoscopy will definitively take care of the polyp at a single procedure, which can be more attractive than the prospect of multiple endoscopic procedures in the outpatient endoscopy suite. 15
Polyp Selection
There is considerable debate on characteristics that are most likely to predict whether there is malignancy within a polyp. Residual malignant disease (in the colon wall or locoregional lymph nodes) even after complete endoscopic resection of polyps can be as high as 19%. 16 The rate of lymph node involvement for malignant polyps is 6%–17%. 17 Therefore, there is fairly good consensus that if there is high suspicion of submucosal invasion of malignancy within a polyp, especially for a difficult polyp, the patient should be offered segmental colectomy instead of colon-preserving procedures. 17 What is more contentious is what these markers of “high suspicion” are. It is important to note that an in-depth description of the classification of gastrointestinal neoplasms is beyond the scope of this review. We aim to outline the surgical options for managing polyps that are deemed endoscopically unresectable for any number of reasons, whether it be the polyp location, polyp positioning, polyp characteristics, or even geographical limitations in accessing expert endoscopists by patients in rural areas.
First-line treatment for almost all polyps remains endoscopic treatment and with wider application of EMR, even large sessile polyps are effectively treated using endoscopy alone. Endoscopic criteria can be used to predict whether a lesion contains submucosal invasion, in an effort to guide the most appropriate next step in treatment. 5 Our focus is particularly on polypoid lesions of the colon and rectum, also referred to as protruded lesions, although the criteria can be equally applied to lesions referred to flat adenomas or slightly elevated lesions, which are more likely to be benign than all other subsets. 18 Depressed lesions, which comprise about 2% of colorectal lesions, have been shown to have high malignant potential even at small sizes and therefore are best approached with caution when considering approaches of limited resection outlined below.
Increasing lesion size is often associated with increasing risk of malignancy in polypoid lesions. 19 Some studies have reported rates of malignancy as high as 42% for polyps larger than 2 cm, 20 while others have found the risk lower at around 8%. 21 Size criteria is less predictive in nonpolypoid lesions, with high malignant potential seen even in small depressed lesions in contrast to very large lateral spreading tumors that may be completely benign. 18 Therefore, size alone is not an absolute contraindication to attempting polypectomy, and size criteria should be combined with other polyp features when deciding on the malignant potential of a polyp.
Lesion morphology is another feature that can be used to predict malignancy. Paris classification of 0-IIa+c and a nongranular surface are risk factors for submucosal invasion. 5 In addition to using morphological evaluation systems such as the Paris classification, the general appearance of a polyp based on the experience of the endoscopist can be just as important at predicting malignancy. 22 Morphologic signs that point to malignancy within a polyp include irregular contour, ulceration, broadening of the stalk, hard polyp consistency upon gentle probing, 17 or absence of air deformation indicative of rigidity. 18
Surface pit patterns and vascular patterns, usually better seen on narrow-band imaging can also contribute to the overall distinction between benign and malignant polyps. 23 Regular cribriform convolutions generally reflect an adenoma, whereas irregular and amorhous patterns are more likely to be associated with malignancy. Irregular vascular patterns in protruded lesions and sparse vascular patterns in depressed lesions are characteristics associated with carcinomas. 22
Failure to lift a polyp with submucosal injection is generally regarded as a sign of possible malignancy. 24 However, failure of a polyp to lift should be interpreted with caution if there have been previous attempts at biopsy. As many as 30% of patients with a history of biopsy can exhibit the nonlifting sign even in the absence of malignancy 25 and prior attempt at EMR has been shown to decrease the success rate of a repeat EMR. 5
Some authors have argued that any polyp with high-grade dysplasia should automatically undergo bowel resection, 26 while others have successfully treated multiple polyps with high-grade dysplasia without encountering any malignancy within the specimen. 21 It is probably most reasonable to consider the presence of high-grade dysplasia in combination with other characteristics such as polyp size, morphology, and surface pattern to estimate the risk of malignant change instead of proceeding directly to segmental resection based on high-grade dysplasia alone. 17
Table 1 lists some of the criteria that are usually used to rule out polyp malignancy. In general, the risk of finding a cancer for polyps that are not amenable to endoscopic resection is not negligible. Bertelson et al. looked at 750 patients who underwent oncologic segmental colon resection for unresectable polyps, 90% of which were over 2 cm. The rate of malignancy was 18%, with one-fourth of those patients harboring lymph node metastases. 27 In general, polyps that are smaller than 2 cm, soft in consistency, are nonulcerated, and demonstrate regular pit and vascular patterns are more likely to be benign. If a polyp does not demonstrate enough malignant features, laparoscopic-assisted polypectomy can also be considered a stepping stone to definitive pathologic diagnosis with subsequent segmental resection if malignancy is indeed identified.
NBI, narrow-band imaging.
Intraoperative Frozen Section
It is not clear whether routine intraoperative confirmation of a benign polyp is necessary. Some groups routinely perform intraoperative frozen section for all resected polyps. 28 Others advocate the concept of ‘visual biopsy‘, which is the endoscopist's visual assessment of whether the polyp is malignant. They reserve intraoperative frozen section for highly suspicious lesions that are firm on palpation or seem multilobulated after excision. 21 Given the false-negative rate of intraoperative frozen sections, our preference is to use intraoperative frozen section sparingly in cases that are highly suspicious for cancer. Ultimately, if after the more limited approaches to polypectomy, the final pathology result reveals malignancy, very few bridges are burnt by the use of laparoscopy. The patient then has the benefit of confirmatory pathologic diagnosis and can be staged appropriately before undergoing an oncologic segmental resection.
Laparoscopic-Assisted Colonoscopic Polypectomy
Laparoscopic-assisted polypectomy was first described in 1993 as a means of sparing patients the morbidity associated with major bowel resection. 29 This technique appears to be the one used most frequently when a combined laparoendoscopic approach is required for removing a polyp.
The description of the technique is quite uniform with the exception of a few details. Most groups have used CO2 insufflation for endoscopy to facilitate visualization during laparoscopy,21,30 but the procedure can also be successfully completed with air insufflation. 31 Presenting the polyp to the endoscopist using laparoscopic instruments is the hallmark of this method. This often involves mobilizing flexures and straightening curves that may have impeded the polypectomy on initial colonoscopy. An ileal bowel clamp is used regularly by some, 30 selectively by others, 32 and not at all by the rest. 21
The laparoscopic visualization provided during this technique has the added bonus of allowing inspection of the colon for full-thickness burns and perforations. If there is any such defect, it can be repaired immediately, usually using intercorporeal suturing, thus sparing the patient the morbidity of potentially missed perforations. Vokurka et al. describe suturing the site of the base of the removed polyp in all patients, 33 whereas Franklin and Portillo found only about 10% of patients required laparoscopic suturing. 34
The benefits of laparoscopic-assisted colonoscopic polypectomy (LACP) for the patient are avoidance of a major abdominal resection and preservation of colon length. For most patients, the recovery time more closely resembles that of colonoscopy 34 and most are discharged 1 day after the procedure (Table 2).
number of each alternate treatment for failed LACP.
CAL-TR, colonoscopy-assisted laparoscopic transluminal resection; CAL-WR, colonoscopy-assisted laparoscopic wedge resection; LAC, laparoscopic assisted colectomy; ESD, endoscopic submucosal dissection; EMR, endoscopic mucosal resection; HGD, high grade dysplasia; LACP, laparoscopic-assisted colonoscopic polypectomy; LOS, length of stay; N/S, not specified; n, number of patients receiving specified therapy.
The length of operation varies from 93 to 185 minutes (Table 2). Perhaps the biggest deterrent for most physicians is the additional operating resources and the coordination required between two specialists, one to perform laparoscopy and another to perform simultaneous endoscopy. At the very minimum, this type of hybrid procedure requires additional staff, some with a different skill set than the standard circulating nurse, surgical resident, or assisting surgeon, as well as additional equipment, namely the necessary ESD/EMR equipment. 15
This technique is feasible for polyps located anywhere in the colon with variable success rates of 61%–84% (Table 2). This procedure is most suitable for patients affected by moderate-sized polyps, sessile polyps, and polyps that are located in difficult bowel sites, which are hard to reach by a colonoscope, but for which polypectomy is at least in theory feasible. 35
Laparoscopic Approach to Endoscopic Full-Thickness Resection
While stapling from outside of the colon wall may be more intuitive for the surgeon, closing the polypectomy defect from inside the colon is an endoscopic approach that is gaining popularity 36 with a handful of studies examining its concurrent use with laparoscopy (Table 3). Much of these data are still experimental with human trials lacking for many of the devices. For example, in 1 animal experimental study, the edges of the polyp were marked using BraceBars™ (Olympus Medical Systems Corp., Tokyo, Japan) that were inserted laparoscopically from outside to inside of the colon. The colon was then inverted by oversewing of the inversion in two layers. Subsequent endoscopic full-thickness excision was performed using endoscopic diathermy. 37 However, the original procedure, as described above, took so long and was so cumbersome with its requirement for the use of two endoscopes that it forced the authors to modify their technique into one involving the use of BraceBars to evert the colon with subsequent stapled wedge resection. 38
IMCA, InScope Multiclip Applier; TAS, Tissue Apposition System.
Of the devices used for full-thickness closure, the T-tag Tissue Apposition System (TAS™) appears to be easier to use with good results in both animals 39 and small number of humans. 40 It has been used in combination with laparoscopy to visualize the full-thickness bite of the needle and ensure adjacent organs and blood vessels are not damaged when taking these bites. Laparoscopy can thus be useful as a stepping stone along the learning curve of endoscopic full-thickness resection (EFTR). It can improve its safety profile by improving visualization as well as providing a means of performing immediate repair if the endoscopic closure system should fail. As these systems develop further, laparoscopy may eventually be reserved for dealing with complications of the procedure alone, similar to its current role in managing colonoscopic perforations.
The hybrid laparoscopic and endoscopic approach to polypectomy followed by full-thickness closure offer the benefits of laparoscopic landmarking and mobilization combined with endoscopic retrieval features of LACP. The full-thickness closure is thought to prevent both unrecognized perforations as well as delayed perforation of large polypectomy sites. The main limitation of most EFTR systems, which makes the use of concurrent laparoscopy even more important, is the fact that they are limited to use in antimesenteric polyps. The closure systems can cause bleeding if placed in the mesenteric border and also pose the danger of injury to adjacent organs if used blindly.
Colonoscopy-Assisted Laparoscopic Wedge Resection
There is a subset of patients for whom LACP is not feasible due to polyp morphology or location. There is a further subset for whom, even if LACP might be theoretically feasible, a simple wedge resection may offer a much shorter procedure with minimal increased risk. This is especially true for cecal polyps where the bowel wall can be quite thin and the size of the cecum can easily accommodate a wedge resection. A step-wise approach has been employed by some, whereby intraoperative colonoscopy is used to determine if a lesion is amenable to laparoscopic-assisted EMR or ESD. If the procedure is not deemed feasible, laparoscopic-assisted wedge resection is performed, with segmental colectomy as a last resort option. 24
As with LACP, colonoscopy is used to locate the polyp in the colon. Mobilization of the colon is often necessary to facilitate wedge resection and polyp identification. Most authors recommend advancing the endoscope beyond the lesion to protect the lumen from narrowing during stapling. The key step in this approach is accurate localization of not only the polyp itself but also the extent of its edges, which may be quite irregular, so that complete resection can be performed. Transillumination of the colon with subsequent stapler placement and endoscopic view to ensure complete inclusion of the polyp in the stapler are the most commonly used options. Another option is laparoendoscopically placed BraceBars (Olympus Medical Systems, Olympus KeyMed, Southend-on-Sea, United Kingdom) from inside of the colon to evert the polyp with subsequent stapled resection. 38 Endoscopic tattooing and argon plasma coagulation application with laparoscopic observation of the serosal surface for color and thermal changes are two other options.38,41 Whichever localization method is used, wedge resection is usually performed with an endoscopic linear stapler. For lesions close to the ileocecal valve, the colonoscope can be inserted into the terminal ileum before stapler placement to protect the valve. 24
In one of the largest series on this technique, half of the patients with difficult benign polyps were treated using colonoscopy-assisted laparoscopic wedge resection (CAL-WR) (Table 4). Overall results were excellent with only one local recurrence (0.9%) after 2.9 years. Interestingly, but perhaps not surprisingly, during follow-up colonoscopy, 29% of patients had metachronous adenomas, which highlights the importance of ongoing surveillance in this high-risk population. 42 Success rates can be as high as 100% with good polyp selection, 43 although some groups have used the technique sparingly for only the most benign-appearing polyps. 11
CAL-TR, colonoscopy-assisted laparoscopic transluminal resection; CAL-WR, colonoscopy-assisted laparoscopic wedge resection; LACP, laparoscopic-assisted colonoscopic polypectomy; LOS, length of stay.
Advantages of colonoscopy-assisted laparoscopic wedge resection (CAL-WR) include a full-thickness excision, which does not leave one guessing as to the adequacy of the depth of excision. Procedure time is often shorter than LACP, ranging from 62 to 150 minutes.11,43 Additional equipment requirements are minimal and often an intraoperative endoscopy tower with basic accessories such as injection needles is all that is necessary.
The length of hospital stay is longer than for endoscopic resection, ranging from 1 to 8 days, since this procedure does involve partial colon resection (Table 4). However, since most of the studies were done before implementation of enhanced recovery programs, it is not clear how much of the delay in the past has been due to ileus and other patient-related factors versus surgeon preference. Another minor downside to CAL-WAR is that specimen retrieval may require enlargement of one of the port sites depending on the bulk of the polyp.
Colonoscopy-Assisted Laparoscopic Transluminal Resection
This technique is similar to CAL-WR in principle. Much of the initial steps are as described above. However, instead of a wedge resection, transluminal resection involves a colotomy followed by polypectomy using diathermy or staplers (Table 4).
Colonoscopy-assisted laparoscopic transluminal resection (CAL-TR) can be particularly useful for lesions that are located in challenging positions. For posterior lesions that may be close to the ileocecal valve, a colotomy and excision of polyp under direct vision followed by suture closure has been performed. 35 For lesions located near the mesentery, a small colotomy followed by lesion elevation and resection or stapling can be used. The colotomy is then closed by laparoscopic sutures or a linear stapling device. 42
Colonoscopy-assisted localization with the help of laparoscopy followed by minilaparotomy, colostomy, and polyp excision has also been described.44,45 In some cases, preoperative colonoscopy may suffice if the lesion is tattooed for subsequent laparoscopic localization followed by colotomy and polypectomy. 41
Overall there is a paucity of published studies on this technique, most likely reflecting careful case selection and the more common use of CAL-WR where possible (Table 4). However, one would expect the outcomes to be much the same as CAL-WR, given the similarities between the two techniques.
Laparoscopic Segmental Resection
If a polyp is not amenable to any of the above methods of resection, and especially when there is suspicion for malignancy, a segmental colonic resection may be required. This form of resection should follow oncologic principles wherever possible. It is now widely accepted that minimally invasive colon resection offers the benefits of quicker recovery and shorter hospital stay. 8 Therefore, in our opinion, minimally invasive colectomy should be offered to all patients who are suitable for laparoscopy. When laparoscopic resection is being performed for polyps, rates of conversion to open surgery can be as low as 3%, 11 but are usually in the range of 4.5%–10%46,47 (Table 5). Reporting of complications is highly variable ranging anywhere from 4.6% to 18% with mortality around 1% (Table 5). If a polyp is difficult enough to require segmental resection, colectomy based on oncologic principles should be performed since up to 20% of polyps that were thought to be benign preoperatively will harbor some malignancy within the polyp or the regional lymph nodes. 48 In this situation, returning to the abdomen to perform a more extensive resection with the requisite number of lymph nodes for appropriate staging can be challenging.
Conclusion
The use of laparoscopy can greatly extend the capabilities of endoscopists when dealing with benign-appearing difficult polyps. The role of this technique is continually evolving and may depend on the local endoscopic expertise available. Large sessile polyps that can be removed by piecemeal EMR or ESD at expert quaternary centers may be more easily managed by hybrid laparoendoscopic techniques in other centers with little added morbidity. Table 6 summarizes the above methods and their utility in each situation. We have devised an algorithm (Figure 1) to guide decision making on the use of particular techniques depending on the polyp characteristics that have rendered it unresectable. It is worth keeping in mind that even though different methods have been presented separately here, most groups have actually utilized a number of different approaches to polypectomy by combining laparoscopy and endoscopy in a variety of ways.24,44 It is therefore better to think of these methods as a spectrum of minimally invasive interventions rather than discrete entities. All of these can be available to the advanced endoscopist with proper planning and a collaborative endoscopic/surgical practice.
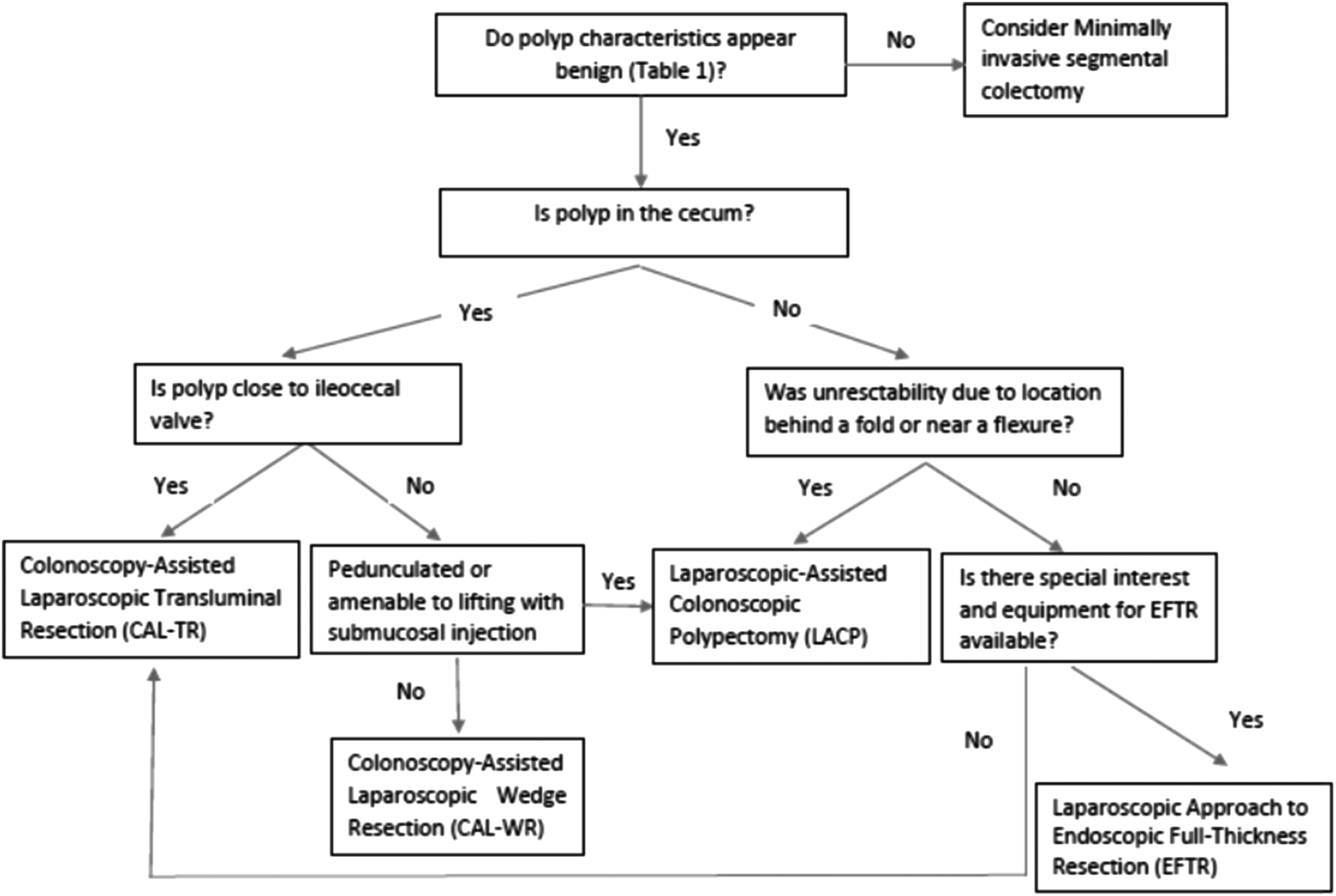
Algorithm outlining the use of various hybrid laparoendoscopic approaches depending on polyp characteristics.
CAL-TR, colonoscopy-assisted laparoscopic transluminal resection; CAL-WR, colonoscopy-assisted laparoscopic wedge resection; EFTR, endoscopic full-thickness resection; LACP, laparoscopic-assisted colonoscopic polypectomy; OR, operating room.
Footnotes
Disclosure Statement
No competing financial interests exist.