
Abstract
Abstract
Objective:
In the present study, intraoperative ureteral injuries inflicted during retrograde intrarenal surgery (RIRS) with ureteral access sheath (UAS) use were evaluated using the Post- Ureteroscopic Lesion Scale (PULS).
Materials and Methods:
Patients in whom a UAS was used during RIRS and for whom ureter images were video recorded during the procedure were included in the study. PULS grading was performed after UAS removal, and video sequences of all patients were viewed by a junior resident, a senior resident, and four experienced urologists and assessed according to the PULS. Ureteral lesions in distal, middle, proximal, and multiple locations were evaluated and compared according to the PULS scale. The inter-rater reliability of PULS grading among various urologists was also evaluated.
Results:
The evaluation comprised 101 patients. In 77 patients, 9.5/11.5 French UAS devices were used, and in 24 patients, 12/14 French UAS devices were used. The stone-free rate, clinical insignificant residual fragments, and final stone-free rate were 41.6%, 53.5%, and 98%, respectively. In 58.4% of the patients, no lesions were present according to PULS grading. No lesions of Grade 3 and above were found; however, there were lesions of Grade 1 and 2 in 38.6% and 2.9% of the patients, respectively. Injuries were found in the proximal ureter only and distal ureter only in 45.23% and 40.47% of the patients, respectively. Multiple injuries occurred in 5.94% of the patients (in 3.96% in the proximal and distal ureter, in 0.99% in the mid- and distal ureter, and in 0,99% in the proximal, mid-, and distal ureter). In the grading performed according to the PULS classification, there was a high accuracy among the residents and specialists.
Conclusions:
The assessment of UAS-induced injuries using standardized intraoperative methods will help to evaluate the procedure more objectively and will guide the postoperative follow-up of patients.
Introduction
U
Any initiative proposed for the maximum benefit and minimum damage of patients has inherent limitations. Hence, clarification of the limitations with a comprehensive evaluation using standardized objective methods is necessary.
To classify ureteral lesions that occur during ureteroscopy, two ureteral wall injury classifications were recently proposed according to endoscopic findings: endoscopic ureteral wall injury and the Post-Ureteroscopic Lesion Scale (PULS).3–5 Despite minor differences in the description of ureter lesions of differing degrees, both classification systems are relatively compatible with each other. In this respect, an evaluation of UAS-related discernible damage systematically showed that ureteral wall injuries involving the ureteral smooth muscle layer after UAS insertion during RIRS are not rare. 3
In the present study, intraoperative ureteral injuries inflicted in patients during RIRS with UAS use were evaluated using the PULS.
Materials and Methods
Patients with stones in whom a UAS was used during RIRS from January 2013 to May 2014 in our clinic were reviewed. The study comprised 101 patients whose ureter images were video recorded after UAS removal during the procedure. Patients in whom a double J (DJ) stent was previously inserted or UAS insertion failed on the first attempt and patients with balloon dilatation or passive dilatation were excluded from the study. The medical records, physical examinations, urine analyses, urine cultures, biochemistry, complete blood counts, computed tomography scans, operation results, and complications of all the patients were assessed according to the Clavien classification system. 6
The study was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Ureteroscopy
With the patient under general anesthesia in the lithotomic position, a hydrophilic guide wire was inserted to the renal pelvis via a Storz semirigid ureteroscope (Karl Storz, Tuttlingen, Germany) with a diameter of 7.5–9.5 French under fluoroscopic guidance. A 0.035-inch, 145-cm Roadrunner® (Cook, Bloomington, IN) guide wire was used in all cases. The whole ureter until the ureteropelvic junction was visualized with ureteroscopy. Although patients with ureteral stricture or ureteral stone were excluded from the study, in patients with normal ureters RIRS was subsequently performed by leaving the hydrophilic guide wire in the renal pelvis.
RIRS
Two types of UAS with diameters of 9.5/11 French and 12/14 French were used. UAS selection differed according to the preference of the surgeon. The UAS was inserted into the ureter via a guide wire under fluoroscopic guidance. For stone fragmentation, the holmium:YAG laser was used.
PULS grading
After UAS removal, video sequences of all the patients were viewed by six experienced urologists and assessed according to the PULS (see Table A1 in the Appendix). Stone size, intrarenal localization, access sheath type, and process time were evaluated according to the PULS grade. Ureteral lesions in distal, middle, proximal, and multiple locations were evaluated and compared according to the PULS scale. The inter-rater reliability of the PULS grading among various urologists was also evaluated in the present study (see Appendix).
Statistics
The mean, standard deviation, median, minimum–maximum, ratio, and frequency values were used in the descriptive statistics of the data. Kendall's t test was used for a correlation-compliance analysis.
Results
The evaluation comprised 101 patients. The mean patient age was 44.6 (± 14.0) years, with a population of 36.6% female and 63.4% male, and patients had an average stone size of 2834 (± 2279) mm3. The mean intervention time was 126.3 (± 48.9) minutes and 1.1 (± 0.4) hospitalization days. In 77 patients, 9.5/11.5 French UAS devices was used, and in 24 patients, 12/14 French UAS devices was used. The stone-free rate, clinical insignificant residual fragments, and final stone free rate were 41.6%, 53.5%, and 98%, respectively. In 2 patients, Clavien Grade 3a complications occurred, and in another 2 patients, Clavien Grade 2 complications developed. 6 Hydronephrosis of Grade 0–3 was present in 41.6%, 9.9%, 24.8%, and 23.8% of the patients, respectively. Grade 4 hydronephrosis was not observed in any patient. In 45 of the patients (44.6%), a basket was used.
PULS Grade 1 injuries occurred in 11.88% of the patients during the first ureteral access using a semirigid ureteroscope. This slight injury occurred before the insertion of a UAS. Among the lesions related to the semirigid ureteroscope, 83.33% were at the distal ureter, 8.33% at the midureter, and 8.33% at the proximal ureter (Table 1).
PULS, Post-Ureteroscopic Lesion Scale.
No lesions were present in 58.41% of the patients in the final evaluation performed according to the PULS grading. No lesions of Grade 3 and above were found; however, there were lesions of Grade 1 and 2 in 38.63% and 2.97% of the patients, respectively. In 54.76% of the patients with ureteral injuries, some injuries included the distal ureter. Injuries were found in the proximal ureter only and distal ureter only in 45.23% and 40.47% of the patients, respectively. Multiple injuries occurred in 5.94% of the patients (in 3.96% in the proximal and distal ureter, in 0.99% in the mid- and distal ureter, and in 0.99% in the proximal, mid-, and distal ureter) (Fig. 1).

The distribution of ureteral injuries according to Post-Ureteroscopic Lesion Scale localization at the end of the procedure.
Significant differences were observed between female and male patients according to the PULS grade. All patients with a PULS grade of 2 were male. No statistically significant difference was observed between different UAS diameters and respective PULS grades. DJ stents were placed in all 101 patients. The mean DJ stent placement time was 14.89 days.
During the evaluation of the video films of the endoscopic procedures, we obtained information about how the injuries had occurred. Among the injuries involving the proximal ureter, the most common cause, with the exception of the injuries inflicted during UAS insertion, was friction of the UAS on the mucosa caused by maneuvers of the flexible ureteroscope, leading to reflexive proximal and distal UAS movement throughout the operation or mucosal clamp during insertion of the UAS into the calculus in an attempt to extract it with a basket catheter. In the injuries involving the distal ureter, the most common cause was injury of the intramural segment of the ureter caused by the semirigid ureteroscope or by the UAS.
In the grading performed according to the PULS classification, there was a statistically significant (P < .05) correlation among a junior resident, a senior resident, and four specialists (Fig. 2).
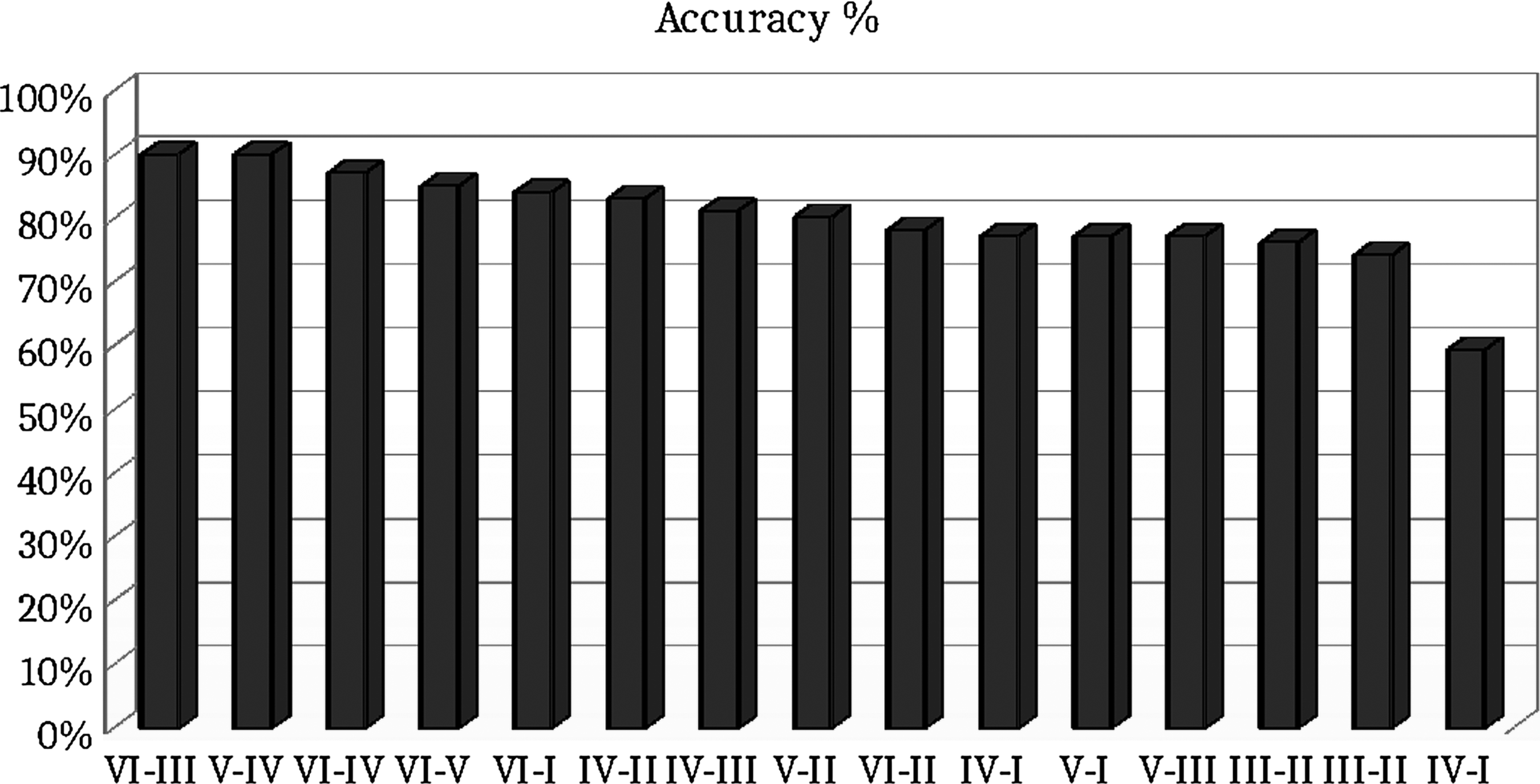
Inter-rater reliability of the Post-Ureteroscopic Lesion Scale, shown as the accuracy among six different urologists.
Discussion
Urology quickly adapts to new treatment modalities and incorporates these modalities as routine procedure; yet, the assessment of intraoperative complications using standardized methods is insufficient.3–8 Many of the new tools and devices that have recently begun to be used, such as the UAS, are based on the initiative of maximum benefit and minimum damage to the patient; yet, these tools also have inherent limitations. Considering that the UAS is placed into a fragile luminal organ such as the ureter, intraoperative events should be evaluated systematically. UAS-related ureteral injuries may stem from ureteral blood supply deterioration, as well as from the instant damage caused by the insertion procedure conducted blindly via the guide wire. 9
Except for the recent article published by Traxer and Thomas, 5 there is insufficient information about the intraoperative evaluation of ureteral integrity. Upon assessment of intraoperative events, intraoperative ureteral injury is not rare. In our study, 38.61% of the patients had injuries; yet, none of the injuries was Grade 3 and above. Almost all injuries were Grade 1. This rate is lower than that reported in the previous publication. We consider that one of the underlying reasons for this difference may stem from the UAS type used. In the majority of our cases (76.2%), a 9.5/11.5 French UAS was used; in the other (previous) study, a thicker 12/14 French diameter UAS was used. This UAS is larger than a nonstented ureter, which has a 9–10 French diameter as reported previously in cadaveric studies. 10 In addition, in the study of Traxer and Thomas, 5 patients who underwent the procedure using a semirigid UAS were excluded from the study, and this exclusion may lead to the fact that further pathologies go unnoticed. Blind insertion of the UAS into the ureter can cause injuries and thus higher PULS positivity. Moreover, the authors also used a different self-defined classification system (endoscopic ureteral wall injury) to report injury outcomes. In their classification, ureteral injuries were classified into two groups as high-grade and low-grade injuries. The two classification systems are very similar to each other; low-grade injuries (Grade 0–1) and PULS (Grade 1–2) are quite similar, but the high-grade (Grade 2–4) injury evaluation differed from the PULS (Grade 3–5). The inter-rater reliability of the self-defined classification system was not evaluated.
Previous studies have considered ureteral injuries as a single entity. No information has been reported regarding whether ureteral injuries occur mostly in the proximal, mid-, or distal ureter.3–5 In the present study, we also analyzed ureteral injuries according to ureteral location, labeled as proximal, middle, and distal. Our study also shows that the lower end of the ureter has a relatively higher risk of injury when considering ureteral injuries occurring during RIRS. During a routine RIRS procedure, a guide wire is inserted into all patients with a semirigid ureteroscope; hence, ureteral injuries during RIRS may not only result from UAS insertion. Reviews of the video images revealed that 54.76% of the injuries were at the lower end of the ureter. We determined that of the ureteral injuries at the lower end, 28.57% occurred before UAS insertion using a semirigid ureteroscope.
While evaluating UAS-related ureteral injuries, we preferred the PULS in the present study. The PULS was proposed by Schoenthaler et al. 4 to standardize intraoperative ureteral lesion grade occurring during ureteroscopy (see Appendix). The inter-rater reliability among a junior resident, senior resident, and specialist, evaluated using Kendall and Spearman tests, was generally high. 2 Subsequently, the PULS was validated more recently by urologists from different countries with a video-based multicenter evaluation. 3 The use of the PULS is recommended for standardized reporting of ureteral injuries after ureteroscopy and more selective standardization of indications for postoperative DJ stenting based on randomized controlled trials. In the present study, ureteral injuries were assessed by six different urologists with compatible inter-rater reliability to prevent rater-related biases. Absence of long-term results of injuries that occurred during semirigid ureteroscopy or UAS insertion is the limitation of the study.
In conclusion, ureteral injuries occur mostly at the distal and proximal ends of the ureter. In addition to the UAS, equipment used at different stages of the procedure, such as the semirigid ureteroscope, may lead to injuries in the ureter, especially in the distal segment. Presenting intraoperative UAS-related injuries within a standardized framework through the PULS provides a common nomenclature and integration between intra- and postoperative management.
Footnotes
Disclosure Statement
No competing financial interests exist.
Appendix
| Grade | Description |
|---|---|
| 0 | No lesion |
| 1 | Superficial mucosal lesion and/or significant mucosal edema/ hematoma |
| 2 | Submucosal lesion |
| 3 | Perforation with less than 50% partial transection |
| 4 | More than 50% partial transection |
| 5 | Complete transection |