
Abstract
Abstract
Purpose:
This study aimed to evaluate the safety and efficacy of single-incision laparoscopic-assisted anorectoplasty (SILAARP) for children with persistent cloaca.
Materials and Methods:
Five patients with persistent cloaca underwent SILAARP and repair of the urogenital sinus between June 2014 and February 2015. The mean age of the patients at the time of operation was 0.80 ± 0.16 year (range, 0.6–1.0 year). An extralong 5-mm 30° laparoscope was inserted through the 5-mm middle port. Two 3-mm lateral ports were placed for instruments. The three ports were placed at a horizontal line through a 2-cm transumbilical incision. CO2 pressure was maintained between 8 and 12 mm Hg. The patients were evaluated for fecal continence and complications.
Results:
SILAARP and repair of the urogenital sinus were successfully performed in all patients. The mean operation time ranged from 120 minutes to 130 minutes. The operative blood loss was minimal. There were no operative complications. All patients were followed up for 0.64 ± 0.29 year (range, 0.3–1.0 year). No patient developed fecal incontinence. Two of the 5 patients (40%) had two to four stools per days, but this did not cause social problems. Only 1 patient (20%) had constipation and required changes in diet. No wound infection, port-site hernia, urethrovaginal fistula, acquired anorectal atresia, or urethral injury occurred.
Conclusions:
Our results show that SILAARP is an effective and safe option for patients with persistent cloaca.
Introduction
P
Since June 2014, SILAARP has been performed in our center for children with persistent cloaca. The current study is the first series to evaluate the safety and efficacy of SILAARP for children with persistent cloaca.
Patients and Methods
Patients
Five patients with persistent cloaca underwent SILAARP and repair of the urogenital sinus between June 2014 and February 2015. Distal colostogram and micturating cystogram were performed preoperatively to identify the type of persistent cloaca (Fig. 1). The rectal pouch was above the pubococcygeal line in these patients. The ages of the patients at the time of operation ranged from 0.6 year to 1 year. The follow-up period varied between 0.3 year and 1 year. All patients had colostomy during the neonatal period (Table 1). Of the 5 patients, 3 (60%) had associated anomalies, including urinary tract (n = 2, 40%) and spinal abnormalities (n = 3, 60%) (Table 2). Ethics approval from the Ethics Committee of the Capital Institute of Pediatrics was obtained. Written informed consents were obtained from the parents of the ARM patients prior to the surgery.
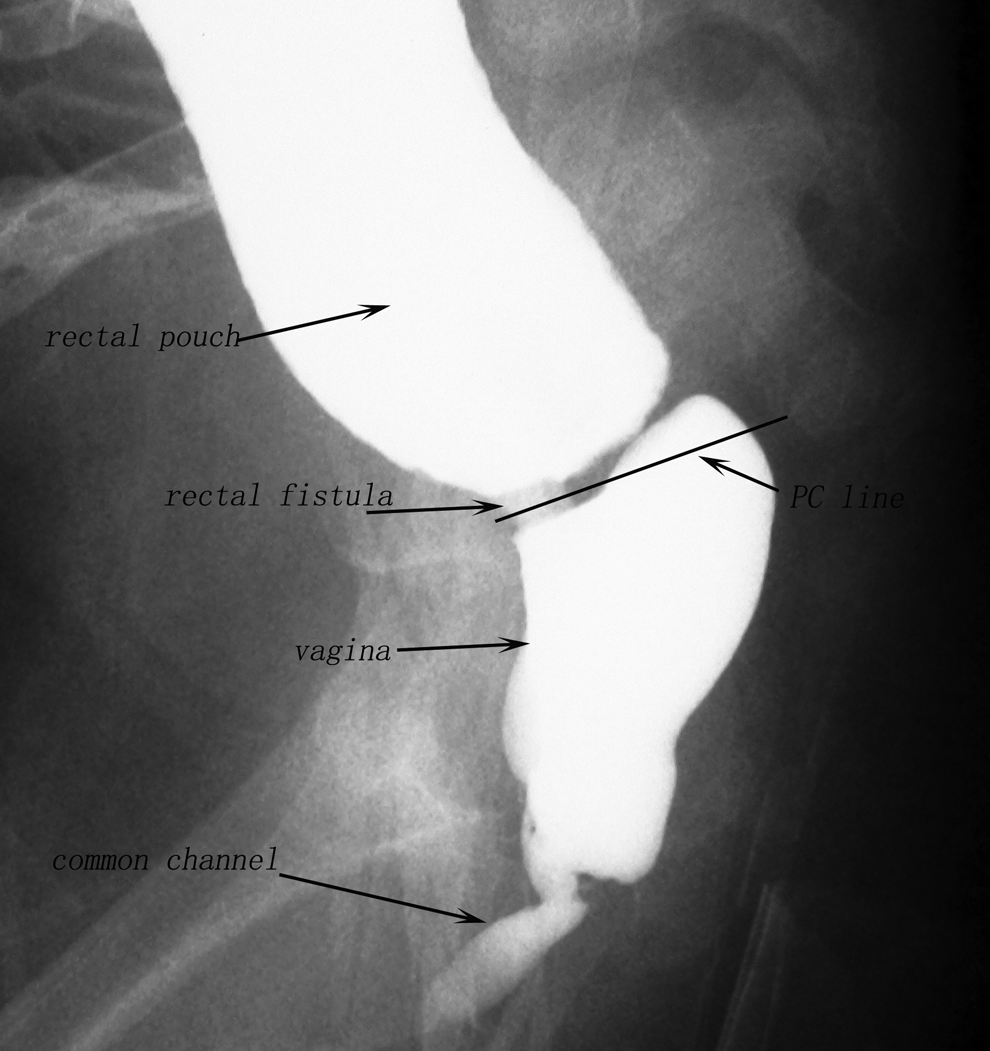
Radiological image of a patient with persistent cloaca.
Surgical technique
The patient was placed in a Trendelenburg position. A surgical towel roll was placed under the buttocks to achieve good exposure of the pelvic cavity.
The bladder was emptied using a urinary catheter. A 2-cm vertical umbilical incision was made and stretched horizontally. An extralong 5-mm 30° laparoscope (model 26046BA; Karl Storz GmbH & Co. KG, Tuttlingen, Germany) was inserted through the 5-mm middle port. Two 3-mm lateral ports were used for instruments. The three ports were placed in a horizontal line (Fig. 2). CO2 pressure was maintained between 8 and 12 mm Hg.
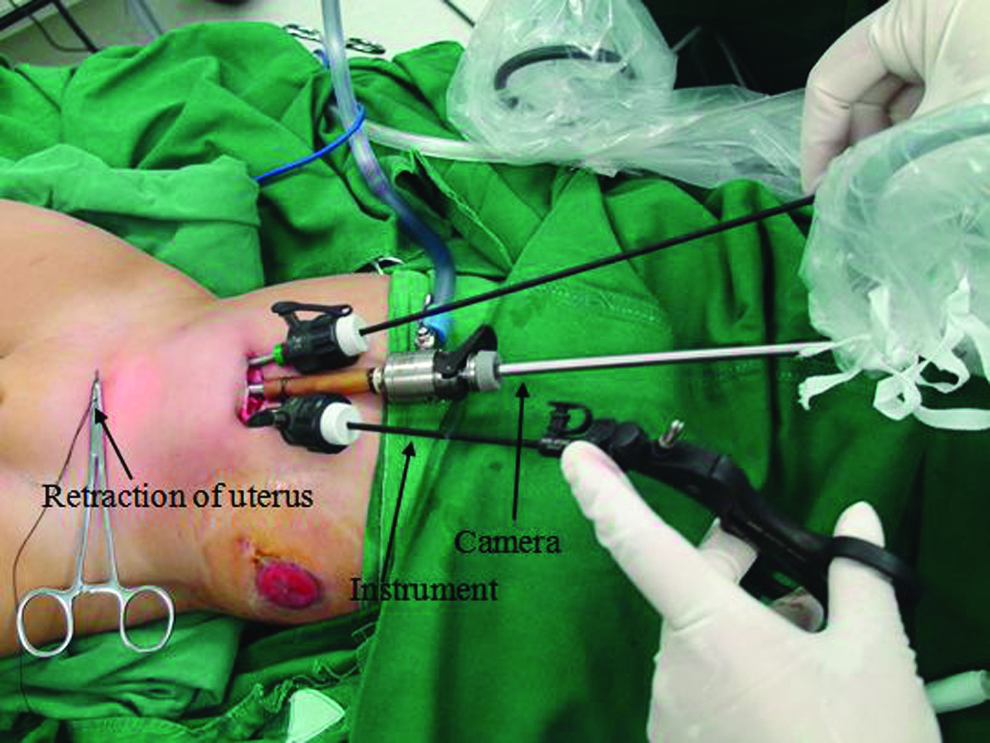
External view of the three ports placed in the umbilicus.
Laparoscopic rectal dissection was begun at the peritoneal reflection. A “window” through the rectal mesentery was created. The terminal branches of the sigmoid and rectal arteries were divided to gain adequate bowel length. A transabdominal suture was placed to help retract the uterus out of the way if the distal rectal pouch was dilated (Fig. 3a and b). The circumferential dissection around the rectal pouch was continued until the junction of the fistula and urogenital sinus was identified. The dissection was performed adjacent to the rectal wall to avoid the injury of surrounding structures. The fistula was clipped with a Weck® Hem-o-lok® clip (Teleflex Medical, Morrisville, NC) as close to the urogenital sinus as possible and then divided (Fig. 3c). If the fistula was wide and short or located in a relatively shallow pelvis, we would transfix the fistula with polydioxanone (PDS®; Ethicon, Somerville, NJ) suture. After dissection of the rectal pouch, the pelvic floor was inspected, and the levators were identified.
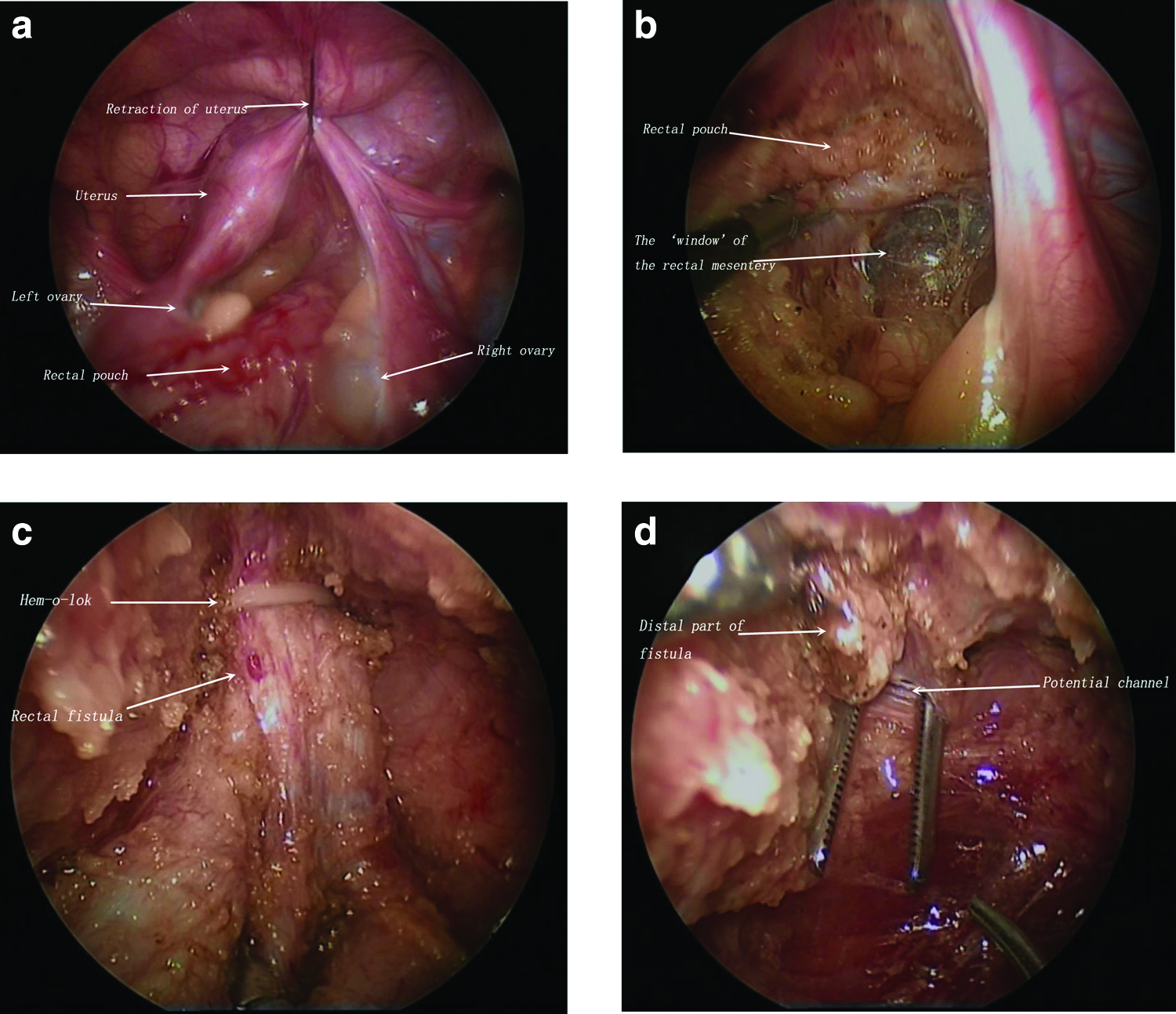
The legs were flexed toward the head, and the perineum was exposed. The center of the external sphincter on the anal dimple was identified using a muscle stimulator. A 1-cm midline skin incision was made over the anal orifice located beforehand. The incision was deepened through the subcutaneous tissues, and the muscle stimulator was used again to identify the midline of the external sphincter. A potential tunnel through the center of the sphincter complex to the pelvis was created using a 7-inch artery forceps under laparoscopic guidance (Fig. 3d). The created tunnel was dilated with a Hegar dilator up to 12 mm. The separated rectal pouch was grasped and pulled down through the muscle complex to the perineum without tension. Anastomosis between the rectum and the anus was performed with absorbable interrupted 5-0 PDS suture.
Repair of the urogenital sinus was then performed. Only the posterior and lateral walls of the common channel were dissected and mobilized through the perineal approach in our procedure. The tissue of the common channel was used to extend the urethra and vagina. The openings of the reconstructed urethra and vagina were sutured to the skin without tension (Fig. 4).
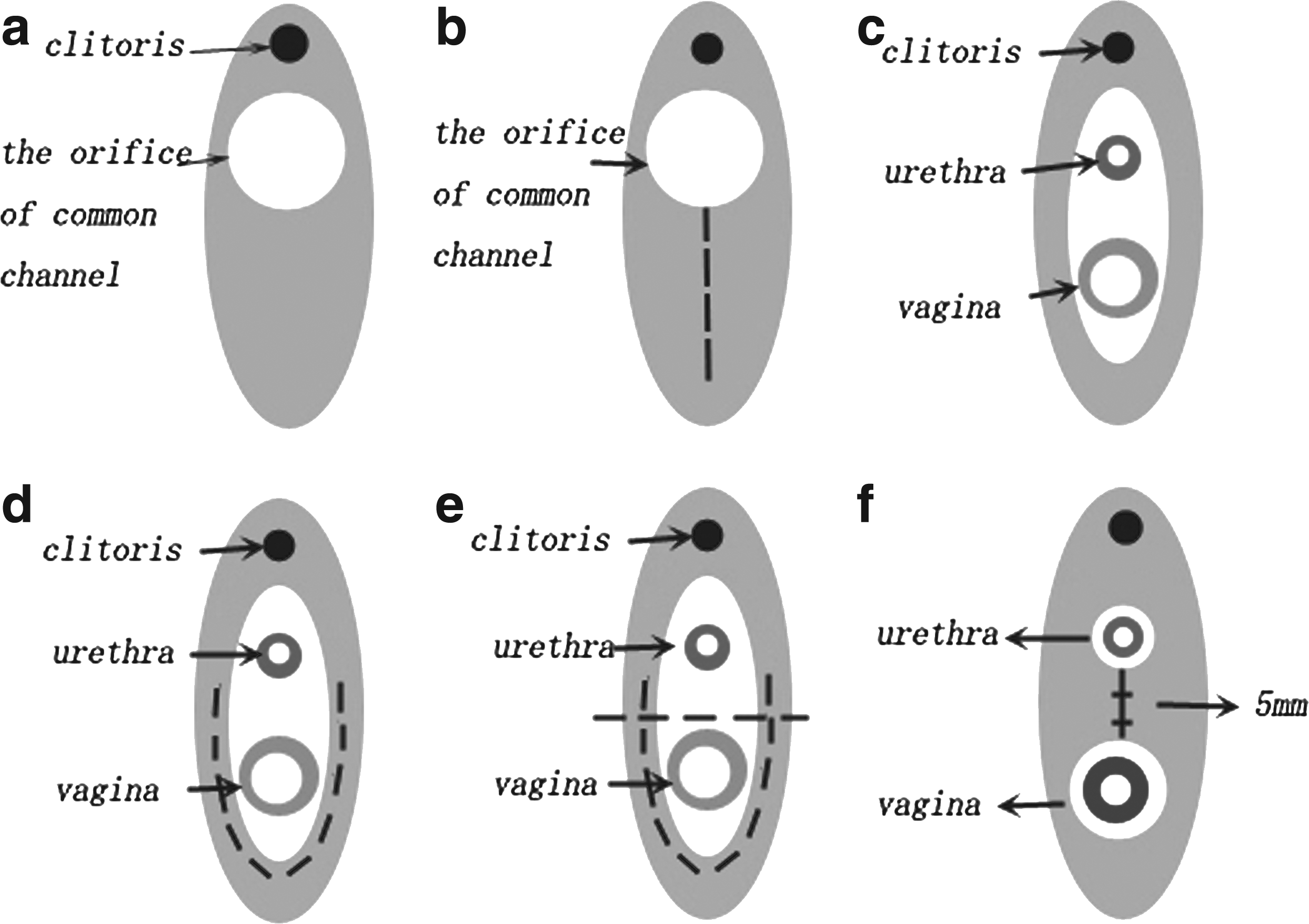
The repair of the urogenital sinus.
On postoperative Day 14, anal calibration and dilatation were initiated. The anus was dilated twice daily, and the size of the dilator was increased weekly until the desired size was reached. The urethral catheter was removed after a micturating cystogram was performed on postoperative Day 10. The colostomy was closed 2 months postoperatively when the anus had reached the desired size. Micturating cystogram and distal colostogram were routinely performed prior to colostomy closure.
Results
SILAARP and repair of the urogenital sinus were successfully performed in all cases. Anorectoplasty, vaginoplasty, and urethroplasty were carried out in the same setting in all patients. The mean operation time was 125.0 ± 5.0 minutes (range, 120–130 minutes). The intraoperative blood loss was minimal. No blood transfusion was required. There was no intraoperative complication. All patients were followed up. The median follow-up period was 0.64 ± 0.29 year (range, 0.3–1.0 year). A good cosmetic outcome was observed in all patients (Fig. 5).

The postoperative bowel function was assessed according to the Krickenbeck classification. 5 We considered those presenting with Grade 3 soiling to have incontinence. None of the patients was labeled as having fecal incontinence. Because all patients were not 2 years old, we did not evaluate the index of voluntary bowel movements. Of the 5 patients, 2 (40%) had two to four stools per days, but this did not cause social problems. Only 1 patient (20%) had constipation and required changes in diet (Table 3).
Mucosal prolapse occurred in 1 case (20%). There was no wound infection, port-site hernia, urethrovaginal fistula, acquired anorectal atresia, or urethral injury. None of the patients needed intermittent catherization to stay dry.
Discussion
Single-incision laparoscopic surgery represents a recent advance in laparoscopic surgery claiming to be less invasive than conventional laparoscopic surgery. 6 Single-incision laparoscopic surgery has been adopted by various divisions of surgery such as gastroenterology,7,8 choledochal cyst, 9 pancreas, 10 gynecology, 11 and urology 12 surgery. Conventional laparoscopic-assisted anorectoplasty has been proven to be a feasible and safe approach for high- and intermediate-type ARM.13,14 Compared with posterior sagittal anorectoplasty, this approach has some advantages, including excellent visualization of the rectal fistula and gynecologic anatomy, minimal surgical trauma, and accurate placement of the rectum into the muscle complex.15,16 SILAARP combines the advantages of conventional laparoscopy and transumbilical techniques. Since 2012, SILAARP has been performed for the management of ARM with rectourethral or rectovesical fistula in our center. The midterm results show SILAARP with conventional straight instruments is safe and feasible. However, there have been few reports in the literature describing SILAARP for management of cloacal malformation. This study is the first series to evaluate the safety and the efficacy of SILAARP using conventional straight instruments for children with persistent cloaca.
The repair of persistent cloaca represents a major technical challenge involving correction of the urogenital defect in addition to anorectoplasty. Some authors recommended repairing the rectal component and leaving the urogenital component for later. 17 We advocate simultaneous repair of all three components. 18 This could reduce the risks found with multiple anesthesias and multiple operations. Furthermore, it eases the physiologic, psychological, and economic burdens of the patients and their parents. However, for patients with a common channel longer than 3 cm, the procedure of urethroplasty and vaginoplasty is complicated. When a patient presents with a long common channel (>5 cm) or a narrow common channel without enough tissue to extend the urethra and the vagina simultaneously, or vaginal agenesis, our technique of urethroplasty and vaginoplasty is not suitable. The common channel would be left intact for construction of the urethra. Colovaginoplasty would be performed. Previous large-volume experience of laparoscopic-assisted anorectoplasty could shorten the learning curve for SILAARP. In our center conventional laparoscopic-assisted anorectoplasty has been performed for the management of persistent cloaca since 2005. Before we started the practice of using SILAARP, we had operated on 9 patients with persistent cloaca and 60 ARM patients with rectovesical or rectoprostatic fistula through a conventional laparoscopic-assisted anorectoplasty procedure. The result of SILAARP is comparable to that of conventional laparoscopic-assisted anorectoplasty.
Although SILAARP provides a better cosmetic outcome, it raises several specific new challenges compared with conventional laparoscopic-assisted anorectoplasty, such as the loss of triangulation with conventional instruments, difficulty of achieving correct exposure and the necessary traction to tissues, and restricted external working space. Despite such expected problems, through our experience we think that our progress in surgical skills helped in overcoming these limitations to a certain extent. First, we placed trocars as described above instead of placing trocars to form an inverted triangle in the umbilicus (Fig. 6). With this placement, the freedom of motion with conventional instruments is increased, and the operation is easily carried out, especially when dissecting the rectal fistula in the lower pelvis. Second, we used the transabdominal suture retraction method to obtain a good laparoscopic view of the pelvic cavity. This method is simple and easy and requires no special surgical instruments, not even laparoscopic forceps. On the other hand, between the rectum and the vagina there was normally firm connective tissue; it is important to lift up the uterus to obtain the optimal tension for the dissection along the plane between the posterior vaginal wall and the rectum.
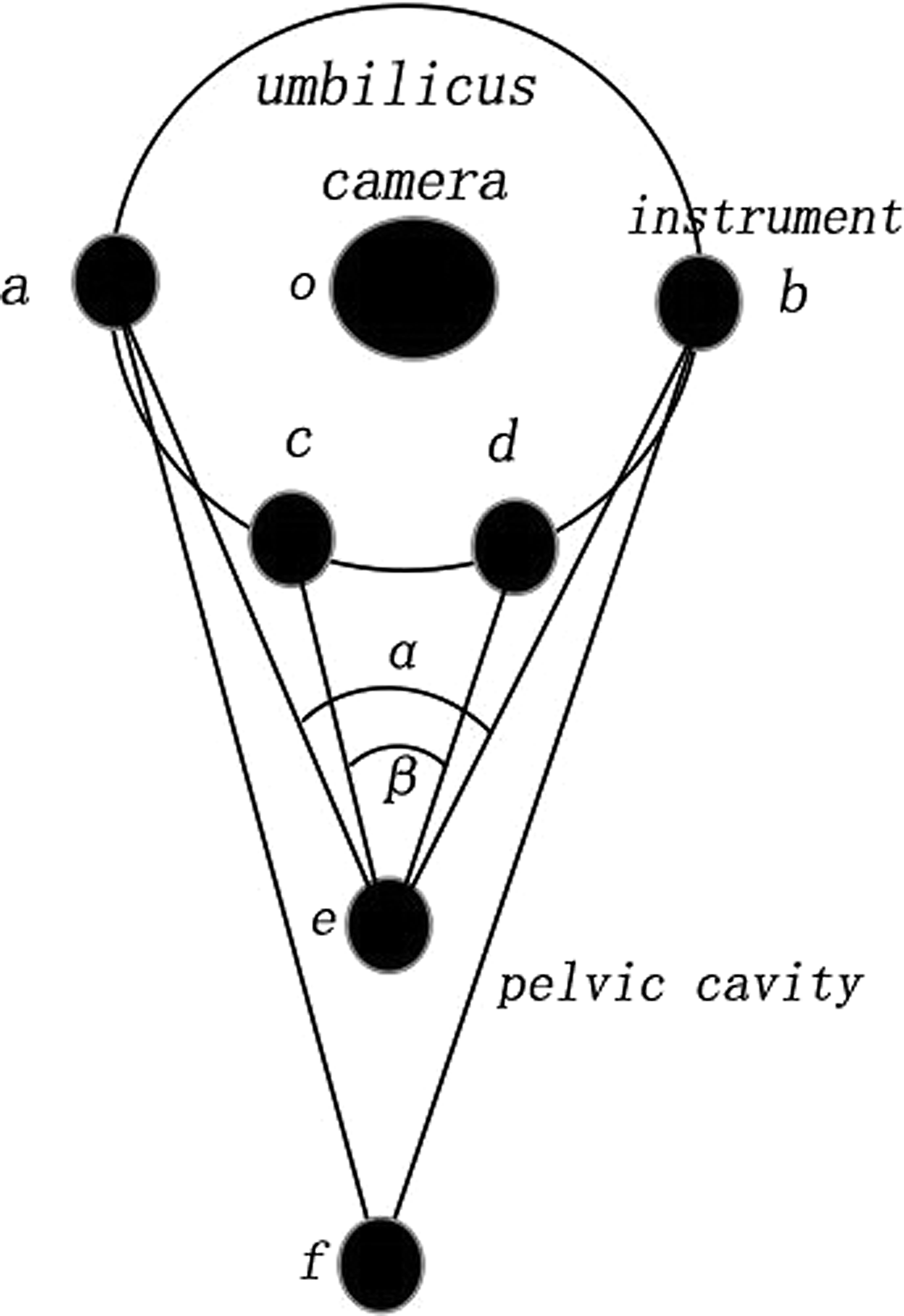
Schematic of the location of the three ports. We placed trocars in a line through the incision, with the 5-mm middle port (o) for the camera and two 3-mm lateral ports for instruments (a and b), instead of placing all trocars to form an inverted triangle (o, c, and d) in the umbilicus. With this placement, the freedom of motion with conventional instruments is increased (α > β), so that the operation is easily carried out, especially when dissecting the rectal fistula in the lower pelvis (o–f > o–e).
There were several drawbacks in our study. First, the indications for our technique were limited to selected patients. For patients who had a low rectum level, laparoscopy was not required. Second, we have just received clinical evaluations for functional results in the follow-up; other objective evaluation methods were not used because most of the children in this series were younger than 3 years of age. Third, there was only a preliminary result of SILAARP. Postoperative bowel function of some patients might be ameliorable in the future. These patients will be followed up in a very long period. A larger series will be necessary for definitive conclusions.
Our result indicates that the repair of all three components can be simultaneously performed in patients with persistent cloaca. SILAARP provides a viable option as a surgical management of persistent cloaca.
Footnotes
Acknowledgments
The work was supported by the Department of Pediatric Surgery, Capital Institute of Pediatrics, Beijing, People's Republic of China. The authors would like to thank Dr. Li Long and Dr. Cheng Wei for their support and mentorship.
Disclosure Statement
No competing financial interests exist.
C.W., L.L., and W.C. designed the research. C.W. prepared the manuscript. W.C. reviewed the manuscript. S.L., Z.C., M.D., L.X., and J.Z. are responsible for data collection.