
Abstract
Abstract
Objectives:
Translumenal access site closure remains a major challenge in natural orifice translumenal endoscopic surgery (NOTES®; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and Society of American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]). We assessed the feasibility and safety of using reserved threads to close the bladder perforation during NOTES and analyzed this novel technique in a live porcine model.
Materials and Methods:
Five female pigs were used in this study. With the animal under general anesthesia, a self-made trocar was inserted into the bladder. Under ureteroscopic guidance, the anterior bladder wall was punctured by a needle into the abdominal wall, and two reserved lines were placed. The bladder perforation was closed with the reserved lines. Procedure time and effectiveness of the closure were recorded and evaluated.
Results:
We completed a total of 5 cases of animal experiments. The first case failed because the weight and size of the animal were too large. The remaining 4 cases were successful. The procedure times were 45, 30, 25, and 25 minutes, respectively. The perforations were closed completely.
Conclusions:
The novel method of using reserved thread to close the bladder perforation was safe and effective. Further large-scale survival studies are needed to prove its clinical potential.
Introduction
A
However, most studies of NOTES are still in the animal experiment stage because closure of the translumenal access site remains a major challenge. Reliable, complete closure of the access site is mandatory to safely introduce NOTES into clinical practice. Different endoscopic techniques for translumenal closure have been described in nonsurvival and survival animal studies. However, no adequate, safe, easy closure modalities have been reported to date. Based on the research of Lima et al. 3 and our earlier research in animal experiments, 4 we used two reserved lines to close a bladder perforation during NOTES.
Materials and Methods
Animals
Female pigs were used in this study. All animals were housed in a temperature-controlled room with a 12-hour light-and-dark cycle, with free access to food and water. The procedures were approved by the Institutional Animal Care and Use Committee of Changhai Hospital (Shanghai, China).
Surgical instruments
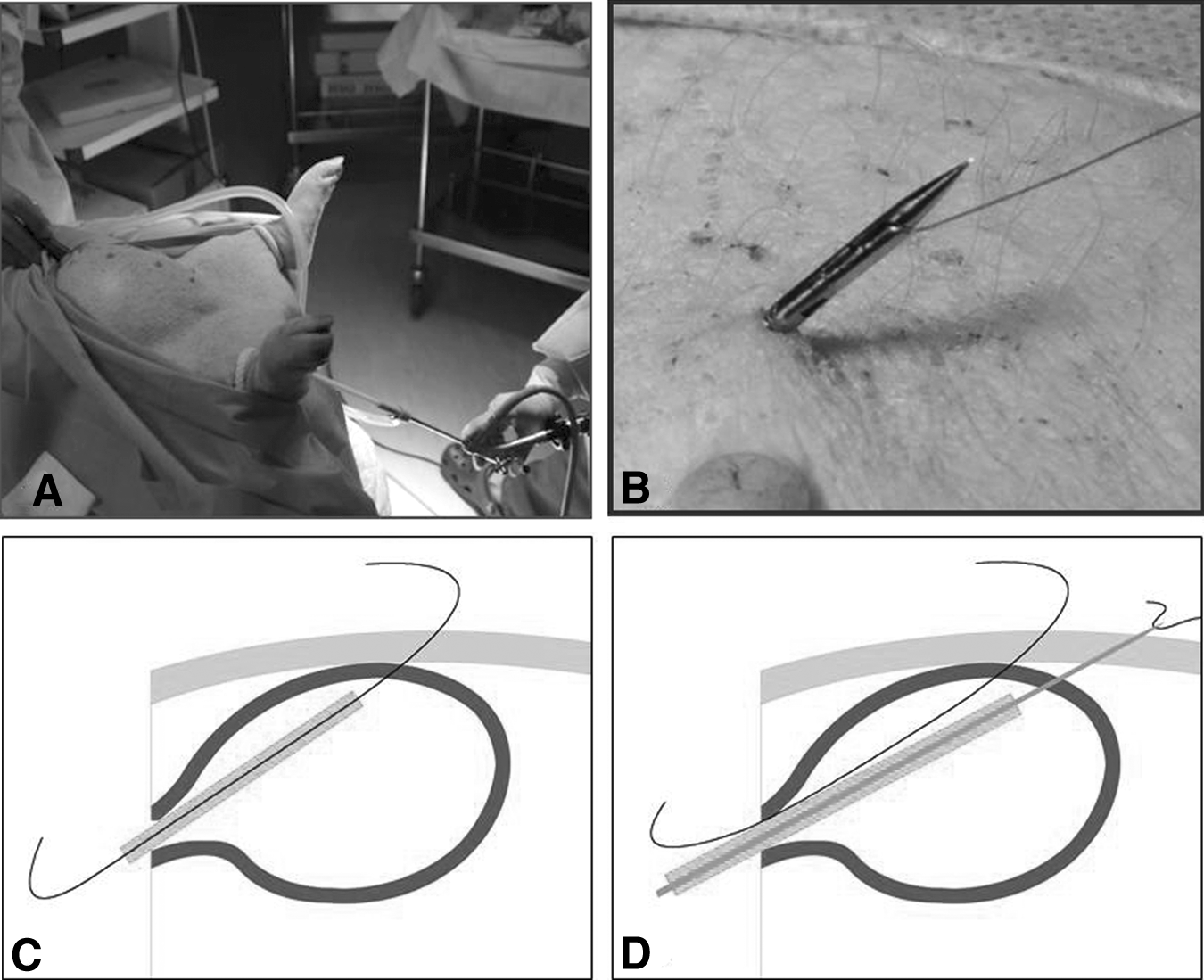
The following surgical instruments were used: a rigid ureteroscope (model A2942A; Olympus, Tokyo, Japan), a 0.035-inch guidewire, a self-made transvesical trocar (Fig. 1A), a ureteroscopic bladder needle and knot-pushing device (Fig. 1B and C), 3-0 violet poliglecaprone 25 (Monocryl™; Ethicon, Somerville, NJ) thread (90 cm in length), and an endoscopic needle electrode.

Device introduction:
Preoperative preparation
The study was completed in the Animal Experimental Center of Covidien in Shanghai. Five female pigs weighing 20–45 kg were selected. Under general anesthesia, animals were placed in the Trendelenburg position.
Techniques
A rigid ureteroscope was introduced through the urogenital sinus and urethra into the bladder. Urine was emptied, and the bladder was distended with CO2. The ureteroscope was then pushed to the anterior bladder wall and as closely as possible toward the abdominal wall. The light of the ureteroscope could be observed outside of the abdominal wall (Fig. 2A). Through the working channel of the ureteroscope, a self-made suture passer was advanced to perforate the anterior bladder and abdominal walls. A 3-0 violet Monocryl thread (90 cm in length) was loaded to the passer (Fig. 2B). The passer was then retracted from the body through the bladder and urethral orifice. As shown in Figure 2C, both ends of the thread were outside the body: one above the abdominal wall and one outside of the urethral orifice. Another thread was placed and reserved in the same way (Fig. 2D).
With an endoscopic needle electrode, a full-thickness longitudinal incision of 0.5 cm was made between the two reserve threads. A guidewire was inserted into the abdominal cavity through the incision, and a self-made trocar was introduced under guidance (Fig. 3A). Pneumoperitoneum was then developed through the transvesicle access. The ureteroscope was inserted into the abdominal cavity through the trocar. The two reserved threads could be easily found inside of the abdominal wall. A grasper was used to retrieve the two reserved threads from the abdominal cavity through the trocar (Fig. 3B). A knot was then made with the retrieved reserved threads (Fig. 3C). The free ends of the two reserved threads were pulled, so that the knot would be pulled back into the abdominal cavity (Fig. 3D).
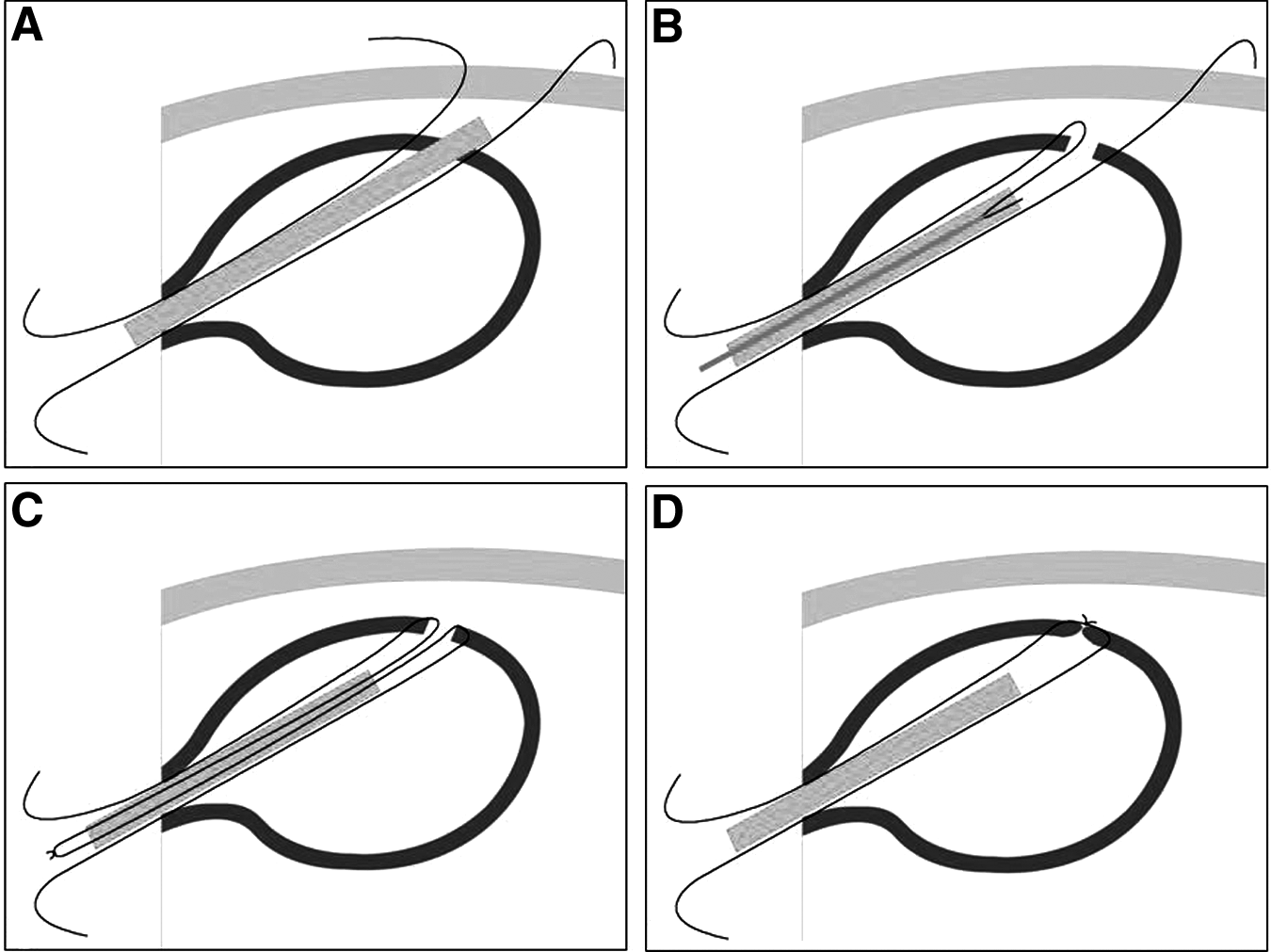
After the NOTES procedure, the trocar was retrieved. Another knot was made with the free ends of the two reserved threads (Fig. 4A). The knot was pushed onto the bladder wall with the knot-pushing device (Fig. 4B). The knot was tightened, and the bladder perforation was closed (Fig. 4C and D).

Evaluation of the closure
Under the direct observation of the ureteroscope and laparoscope, the state of the knot on the inner and outer wall of the bladder was observed. In 3 cases, the abdominal wall was opened immediately after the procedure to expose the bladder. Saline was then injected into the bladder to see whether there was any leakage. In the fifth case, we tried to keep the pig alive for 3 weeks and then opened the abdominal wall to see if any leakage existed.
Results
Five bladder perforation closures on five female pigs were performed. The first case failed because the pig weighed 45 kg, which was too large. In the remaining 4 cases, the pigs weighed 20–25 kg. Average procedure time was 45, 30, 25, and 25 minutes, respectively. No leakage was found after injecting saline into the bladder. For the fifth pig, the catheter was placed for 2 days after the procedure, and the pig was kept alive for 3 weeks. No complications were observed.
Discussion
Minimally invasive surgery that leaves smaller incisions and scars is one of the goals of surgeons. NOTES brings perfect cosmetic results. However, few human studies have been reported. The main technical barriers include, among others, the closure of hollow organs, abdominal organ infection, and the lack of effective instruments.
Translumenal closure remains challenging to surgeons, making it difficult introduce NOTES to human surgeries. Different endoscopic techniques, such as endoclips, 5 T tags, purse-string-modified T tags, 3 flexible staplers, 6 and other prototype suturing devices7,8 have been described for translumenal closure in nonsurvival and survival animal studies. Animal experiments showed that the visceral perforation could be closed by any of the above methods. But, they have their limitations. For example, we had to penetrate the bladder wall using T tags. It is easy to damage the abdominal organs. Endoclips are difficult to complete and are limited to the mucosa. 9 Until now, no adequate, safe, and easy closure modalities have been confirmed for use in humans. Among all these techniques, sutures have their advantages because they may withstand higher endolumenal pressure. 10
In this study, we successfully used the reserved line to close the bladder perforation. This method only used common vascular sutures, a ureteroscopic bladder needle, and a knot-pushing device to close the perforation under the guidance of a ureteroscope. The entire procedure was simple and safe. The effectiveness of the closure was good, and no leakage was found after injecting saline into the bladder. In the procedure, the following points must be noted.
First, the animal's size and weight are important. Compared with the human urethra, that in the pig is relatively long, and the bladder is an intraperitoneal organ. Therefore, the bladder is more mobile within the abdominal cavity. The first case failed because the pig weighed 45 kg. It was difficult to pierce the anterior wall of the bladder to reach the abdominal wall, which affected the closing process. Therefore, for further operations we chose miniature pigs that weighed 20–25 kg, and the other procedures were done successfully.
Second, the bladder puncture sites must be accurately positioned. The anatomy of the bladder in pigs is different from that in humans. Thus, we used a laparoscopic-assisted hole to observe the whole procedure in order to apply our current experience to future studies. We chose the top of the anterior bladder wall as the puncture site. This location was well exposed and easy to locate through ureteroscopy. Therefore, we could accurately place the in-dwelling reserve lines and maintain a distance of approximately 2–3 cm between the lines. When establishing transvesical access for the trocar, we could ensure that the trocar was placed between the two lines, which facilitated the closure of the perforation.
Third, when establishing the transvesical trocar, the best way was to use an endoscopic needle electrode, so that there would be less bleeding, and a clear surgical field could be achieved. The length of the incision should be 2–3 cm approximately.
Fourth, the reserved lines must be suture that is smooth, inelastic, and without lint. Simultaneously, the lines must be fully lubricated throughout the entire procedure. Working with the needle and knot-pushing device outside of the ureteroscope was easier than inside of the ureteroscope. The first line should be accurately in place and solidly knotted; then, the second line can be made.
Fifth, the diameter of the perforation may not exceed 3 cm. If the incision was too large or more than two perforations existed, it would be difficult to complete closure only using the two reserved lines.
Through our experiments, we demonstrated that the reserved line was easily and feasibly performed in vivo and could effectively close the translumenal access after NOTES. Our technology is innovative, the operation procedure is simple, the nonpatented surgical materials are easy to find, and the procedure does not require special surgical instruments. Throughout the four successful animal experiments, the perforation closure time was shortened from 45 minutes to 25 minutes, and the incisions were effectively closed. To understand the subsequent healing of the perforation, a long-term survival assessment of operated-on animals will be the focus of our next research.
Footnotes
Disclosure Statement
No competing financial interests exist.