
Abstract
Abstract
Background:
We aimed to compare the direct trocar insertion (DTI) and Veress needle insertion (VNI) techniques in laparoscopic bariatric surgery.
Materials and Methods:
Eighty-one patients scheduled for bariatric surgery at Inonu University, Malatya, Turkey, were included in this study. In 39 patients, a bladed retractable nonoptical trocar was used for DTI, and VNI was performed in 42 patients. Intraoperative access-related parameters were compared. Data were analyzed with Student's t and chi-squared tests. A P value of <.05 was considered significant.
Results:
Both groups had comparable demographic profiles. Laparoscopic entry time was shorter in the DTI group (79.6 ± 94.6 versus 217.6 ± 111.0 seconds; P < .0001). Successful entry rates in the first attempt, CO2 consumptions, failed attempt rates, and overall intraoperative complication rates were similar. However, in the DTI group, 2 patients had mesenteric injuries, and 1 of them required conversion to open surgery due to the mesenteric hemorrhage.
Conclusions:
DTI in obese patients significantly shortens the entry time, but there can be severe complications with DTI when a nonoptical bladed trocar is used blindly. Actually, neither method can be recommended for entry into the abdomen in this population based on our results. If the surgeon has to choose a nonoptical trocar in bariatric surgery, preference for the VNI technique instead of the DTI technique is safer.
Introduction
A
No matter which technique is used, insufflation is more difficult in morbidly obese patients due to the thickness of the abdominal wall and the peritoneum. Most of the randomized and controlled studies conducted for the comparison of laparoscopic entry techniques exclude morbidly obese patients, and there are only a few studies about abdominal entry techniques in morbidly obese patients.3–11 Increasing numbers of laparoscopic bariatric surgical interventions have prompted new studies to determine the best technique for accessing the abdomen in morbidly obese patients. As far as we know, there is no randomized study in the literature that compares the laparoscopic entry techniques for bariatric surgery.
The aim of the present randomized controlled study was to compare the DTI and VNI entry techniques in morbidly obese patients undergoing weight loss surgery.
Materials and Methods
This study was conducted at the Turgut Ozal Medical Center Gastroenterology Surgery Clinic of Inonu University, Malatya, Turkey. Ethics Committee approval was obtained (approval number 2014-104), and the study was conducted via CONSORT guidance. In the power analysis, in order to get a 6% difference between the DTI and VNI complication rates, the α = 0.05, 1 – β (power) = 0.80 was taken as the baseline, and at least 39 patients from each group were planned to be included in the study. Patients were randomized with the sealed envelope technique. Patients with a body mass index of ≥40 kg/m2 or those with a body mass index of 35–40 kg/m2 with comorbidities related with obesity were selected for surgery. Patients who failed to lose weight with diet and/or physical exercise, between 18 and 60 years of age, were included in the study. Patients with a history of abdominal surgery were excluded. All patients were informed about the operation, and detailed consent forms were taken before surgery. The data were collected in digital media, and intention-to-treat analysis was performed for all patients.
Patients were analyzed according to age, gender, height, weight, body mass index, American Society of Anesthesiologists score, comorbidity, and type of surgical procedure. During the operation, the number of entries, failed attempts (more than three attempts or the need to switch to another entry technique), laparoscopic entry time, CO2 amount used, and complications due to the entry were recorded. The entry complications were evaluated separately from the morbidities of the abdominal wall and the visceral injuries. Minor visceral injuries were accepted as small nonexpanding omental hematomas or retro-omental insufflations; major visceral injuries were gastric, intestinal, mesenteric, or vascular injuries.
Student's t and chi-squared tests were used for statistical analyses. A value of P < .05 was accepted as statistically significant.
Surgical technique
All patients were placed on the 0° tilted operating table in the supine position and given general anesthesia. In the DTI group, a 12-mm bladed retractable nonoptical trocar (Versaport™ Plus; Auto Suture, Covidien, Mansfield, MA) was used for the initial access from 4 cm left lateral of the midline and 20 cm down from the xiphoid process. The abdominal wall was lifted by two Backhaus clamps. The trocar was slowly inserted by rotational controlled movements until the second click sound was heard. Insufflation was begun and continued until the intraperitoneal pressure increased up to 14 mm Hg pressure. The laparoscope was then inserted through this trocar, and the abdomen was inspected.
In the other group, the Veress needle was inserted perpendicular to the abdominal wall 1 cm below the left subcostal margin on the midclavicular line. The saline drop test was performed after the second click sound was heard. After the positive test, CO2 insufflation was begun and continued until 14 mm Hg pneumoperitoneum pressure was obtained. After the creation of the pneumoperitoneum, the abdominal entry technique (type of trocar and access point) was identical to the previously mentioned DTI method. The laparoscope was inserted, and the abdomen and the VNI site were inspected. The time period between the skin incision and the laparoscope's insertion into the abdomen was recorded as the laparoscope insertion time. CO2 consumption was calculated from the beginning of insufflation until 14 mm Hg pneumoperitoneum pressure was obtained. In both groups, either the Roux-en-Y gastric bypass or sleeve gastrectomy procedure was performed according to the decision of the surgeon.
Results
This study was conducted with 39 patients in the DTI group and 42 patients in the VNI group. Two patients were excluded due to a history of previous abdominal surgery. There were no dropouts. In the DTI group, VNI was performed for 2 patients because of the failure in entry. Likewise, insufflation was managed for 1 patient in the VNI group by switching to the DTI technique (Fig. 1). Both groups were similar in age, gender, height, weight, body mass index, comorbidities, and American Society of Anesthesiologists score (Table 1).
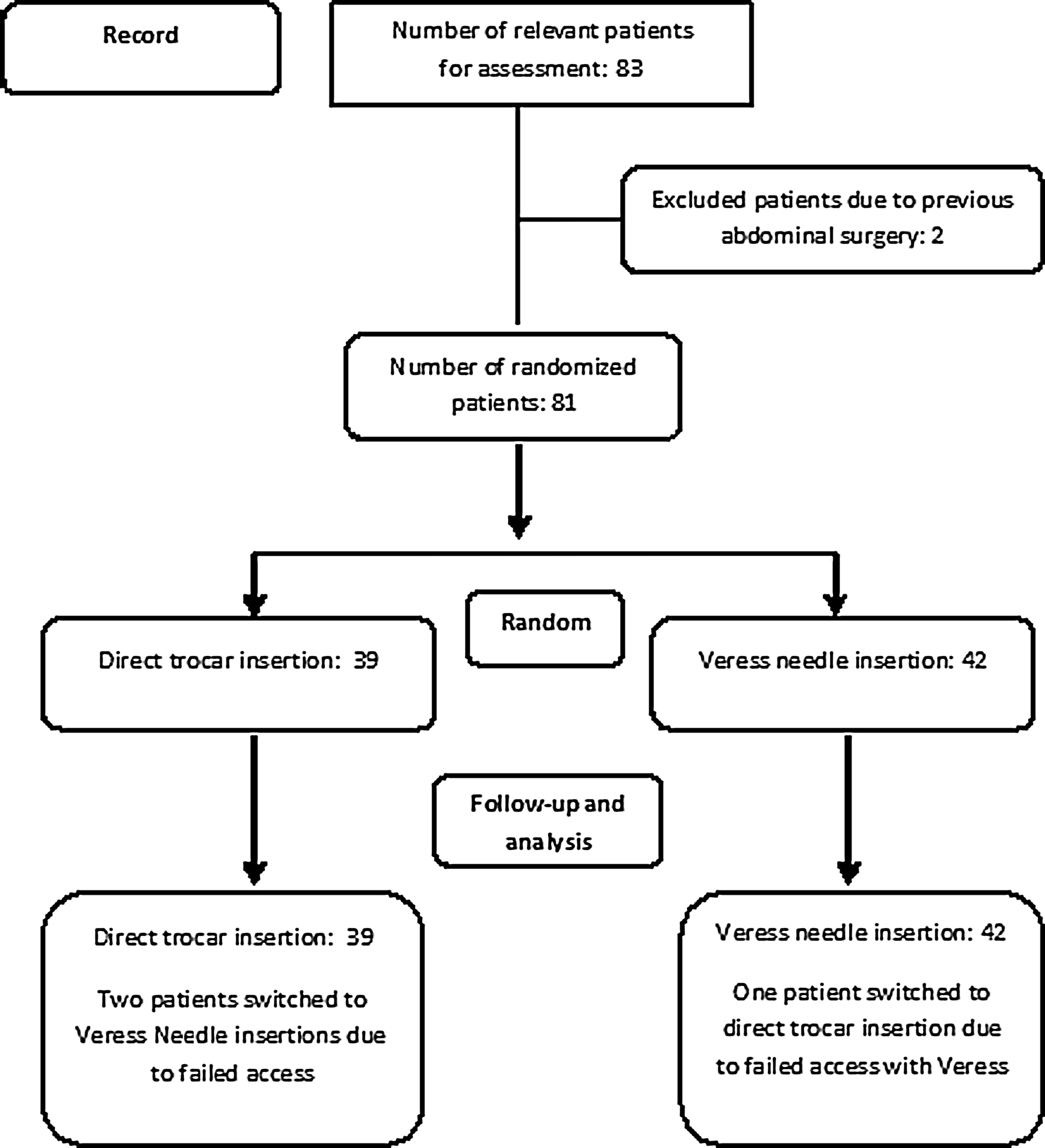
Flowchart of the study design.
Others included goiter, cholelithiasis, coronary artery disease, previous tonsillectomy, nepholithiasis, and hepatitis B carrier.
ASA, American Society of Anesthesiologists; BMI, body mass index; DM, diabetes mellitus; HT, hypertension.
Laparoscope insertion times were shorter in the DTI group compared with the VNI group (79.6 ± 94.6 versus 217.6 ± 111.0 seconds; P < .0001). There was no statistical significance for the difference in the number of entries and CO2 amounts used (Table 2). In the DTI group, the first time entry rate was 74.3% versus 54.7% in the VNI group (P = .13). Similarly, the CO2 used in the DTI group was lower (3.73 ± 1.39 L versus 4.26 ± 1.38 L; P = .09).
Others included tunneling from the stomach wall during gastrotomy and anastomosis, as well as liver bleeding.
Additional procedures included two gastroenterostomies that were performed by hand-sewn anastomosis and one synchronous uterine polyp excision that was added to the bariatric procedure.
RYGBP, Roux-en-Y gastric bypass, SG, sleeve gastrectomy.
In both groups, in total, four visceral injuries were seen as complications. There were four minor omental injuries in the VNI group, and 2 patients in the DTI group had similar minor omental injuries as well. However, in the DTI group, two more major injuries occurred: one was a transverse mesocolon injury that did not require any repair, but the other patient had an injury to the jejunal branch of the superior mesenteric vein that required emergency conversion to open surgery due to uncontrollable bleeding. This patient required repair of the bleeding vein and 7 units of red blood cell transfusions.
Discussion
The VNI and DTI techniques are the most common blind abdominal entry techniques, and morbid obesity by itself is a risk factor for abdominal entry injuries. 10 There are no evidence-based data demonstrating which abdominal entry technique is safer for morbidly obese patients in bariatric surgery. However, nearly all the randomized controlled studies conducted in nonobese population groups comparing VNI and DTI favored DTI as the safest technique.4–8 A meta-analysis pooling the seven randomized controlled studies demonstrated a total of four major complications (liver in 2 cases, small bowel in 1 case, and mesentery in 1 case), all of which were caused by the VNI technique. 12 However, the Cochrane analysis of the entry techniques suggested more randomized controlled studies are needed because of the low number of major complications. 13 In our study, there was no VNI-related major complication, unlike in the literature, and in the DTI group there was one mesocolon injury and one severe injury to the jejunal branch of the superior mesenteric vein that required conversion to open surgery. This severe complication obliged us to make an assessment of whether to stop the study. Because of the rarity of life-threatening complications during abdominal entry, we decided to go ahead and complete the study. Major complications like vascular and organ injuries during abdominal entry are rare, but we believe that reporting such injuries is crucial for evidence-based medicine.
Omental mass is much greater in morbidly obese patients compared with nonobese patients. Borgotta et al. 14 reported omental injury rates of 6.3% in the VNI group and 3.9% in the DTI group, with a total rate of 5.2% in nonobese patients. In our study, the omental injury rates of VNI, DTI, and in total were 9.5%, 5.1%, and 7.1%, respectively. The thick abdominal wall and peritoneum leading to the need for recurrent entries and the difficulty in lifting the abdominal wall effectively may increase the risk of injury to the omentum in morbidly obese patients. However, by the present study we cannot say that omental injuries are more frequent in morbidly obese patients. It can also be assumed that due to the thick omental mass in morbidly obese patients, deeper vascular and visceral injuries can be expected more rarely. We believe that more studies must be done to assess the protective effect of the thickened omentum for the deeper organs in morbidly obese patients.
Angioli et al., 5 comparing DTI and VNI in nonobese patients, reported higher rates of minor injuries in the VNI group. The most common minor injuries were extraperitoneal insufflations and omental injuries. Similar results were reported by Gunenc et al. 15 and Zakhera, 16 where the extraperitoneal insufflation was seen only as a complication of VNI. This is a result of insufficient and multiple attempts with VNI. In both of our groups, there were no cases of extraperitoneal insufflation and/or subcutaneous emphysema. This could be explained by not starting the insufflation without being sure about the abdominal access. The extraperitoneal insufflation can be described as a minor complication; however, there are reports of fatal pneumoembolism in the literature. 17
In the literature, the failed first attempt rates were generally reported to be higher in VNI than DTI (21.8% and 7.8%, respectively). 14 In our study, this rate was 35.8% overall. This higher rate in our study may be due to the morbid obesity of the patients and the different site of entry of the primary trocar other than the umbilicus.
Another important parameter in determining the efficacy of the abdominal access route is the laparoscope insertion time. There is a consensus that DTI is faster than the VNI technique. 13 Our study revealed similar results with the literature. The finding of increased time to full insufflation in the VNI group compared with the DTI group is likely merely a reflection of decreased insufflation flow rate through a needle versus a 12-mm port. However, it must be kept in mind that the time saved with the faster technique is not so important when the total time of the surgery is considered and that the most important aspect is the safety of the entry.
The results we obtained that differed from the previous randomized controlled studies could be due to the fact that (1) most of the studies performed previously were gynecological procedures where the umbilicus was the primary entry site, (2) the subcutaneous area, peritoneum, facia, and omentum are thicker in morbidly obese patients, (3) difficulty exists in traction and lifting of the abdomen in morbidly obese patients, and (4) our trocars used were not optic trocars. The limitations of our study are that it was not a blinded study, it was a single-center study, different sites of abdominal entries were used, and there was a low number of patients to demonstrate the rare major complications.
Conclusions
DTI shortens the laparoscope insertion time in morbidly obese patients compared with VNI. However, the time saved with the faster technique is not so important when the total time of the surgery is considered, and the most important aspect is the safety of the entry. Actually, neither technique can be recommended for entry into the abdomen in this population based on our results. But, if a surgeon wants to select one of these techniques in a morbidly obese patient, our finding of two major complications encountered in the DTI group encourages us to recommend the safer VNI technique in the first line and the DTI technique is offered as the alternative method.
Footnotes
Disclosure Statement
No competing financial interests exist.