
Abstract
Abstract
Aims:
This study evaluated the safety, feasibility, and short-term outcomes of laparoscopic extralevator abdominoperineal excision (laparoscopic-ELAPE) with primary suturing for low rectal cancer.
Materials and Methods:
Consecutive patients who underwent laparoscopic-ELAPE with primary suturing for low rectal cancer at our institution between September 2013 and January 2015 were retrospectively identified from a prospectively maintained database. Short-term outcomes, including intraoperative complications, postoperative morbidity, and oncologic adequacy of surgical specimens, were evaluated.
Results:
Laparoscopic-ELAPE was successful in all 33 included patients, with no patient requiring conversion to an open approach. Mean operation time was 200 minutes, and mean intraoperative blood loss was 90 mL. Except for bowel perforation in 2 patients (6.1%), there were no intraoperative complications. Two patients (6.1%) had positive circumferential resection margins. Median length of hospital stay was 7 days. The 30-day morbidity and mortality rates were 15.2% and 0%, respectively. Postoperative complications within 30 postoperative days included perineal wound infection (2 patients, 6.1%), respiratory infection (2 patients, 6.1%), and chylous fistula (1 patient, 3.0%). Complications at a median follow-up time of 12 months (range, 3–19 months) included local tumor recurrence (1 patient, 3.0%), perineal dehiscence (2 patients, 6.1%), perineal seroma (1 patient, 3.0%), bowel obstruction (1 patient, 3.0%), urinary retention (2 patients, 6.1%), and chronic perineal pain (2 patients, 6.1%). There were no instances of perineal hernia, persistent sinus, or peristomal hernia.
Conclusions:
Laparoscopic-ELAPE with primary suturing appears to be a feasible and safe treatment approach for low rectal cancer, with acceptable short-term outcomes.
Introduction
T
To address this problem, the extralevator abdominoperineal excision (ELAPE) technique was introduced. 9 This technique requires wide excision of the entire pelvic floor and the anorectum but uses less radical dissection of the perianal skin or ischioanal fat compared with sAPE. 9 A series of studies found that ELAPE is associated with lower risks of bowel perforation and CRM involvement, as well as improved cancer-specific outcomes, compared with sAPE.10,11 However, ELAPE poses a difficult challenge for surgeons regarding reconstruction of the perineal defect. Although various solutions have been proposed to deal with this defect, there is no consensus about the optimal method. 12
An option for ELAPE would be a laparoscopic approach. Although laparoscopic surgery is considered safe and effective for the treatment of rectal cancer, 13 there are few published reports on ELAPE completed by the laparoscopic approach. In our department the abdominal portion of ELAPE is routinely performed by a laparoscopic approach, and the perineal defect is conventionally reconstructed with primary suturing. The aim of this study was to evaluate the safety, feasibility, and short-term outcomes after laparoscopic-ELAPE with primary suturing.
Materials and Methods
Patients
Consecutive patients who underwent laparoscopic-ELAPE at the West China Hospital (Sichuan University, Chengdu, Sichuan Province, China) between September 2013 and January 2015 were identified retrospectively from a prospectively maintained database. Institutional review board approval was obtained, but there was no need to obtain informed consent. Patients were included in the study if they had a tumor within 5 cm of the anal verge that was staged as T3 or T4 by magnetic resonance imaging (MRI). Patients who had undergone an emergency surgery, sphincter-preserving procedure, or multivisceral resection, as well as patients with synchronous distant metastases, recurrent cancer, intestinal obstruction, stage T1/T2 tumors determined by MRI, or surgical contraindications, were excluded. Data collection included patient demographics, American Society of Anesthesiologists classification, and MRI results, as well as data on primary tumors, neoadjuvant chemo/radiotherapy regimens, surgical records, histopathological records, morbidity, mortality, and disease recurrence.
Rectal cancer was diagnosed on the basis of blood tests, a full colonoscopy, thoraco-abdominal computerized tomography (CT) scanning, and MRI. Tumor height was determined with use of a rigid proctoscope as the distance from the anal verge to the lower margin of the tumor. The seventh edition of the American Joint Committee on Cancer TNM Classification System was used. Neoadjuvant chemo-/radiotherapy regimens were planned by a multidisciplinary team. Patients with cT3–cT4 and/or node-positive rectal lesions were encouraged to receive neoadjuvant chemo-/radiotherapy. Neoadjuvant treatment was administered as a preoperative short course of radiotherapy (25 Gy in five consecutive daily fractions) or a long course of chemo-/radiotherapy (50.4 Gy in 28 fractions, combined with capecitabine). Usually, surgery was performed 3–5 days after the short course of radiotherapy or 10–12 weeks after the long course of chemo-/radiotherapy. All operations were performed by an experienced surgeon who was fully trained in laparoscopic surgery.
Surgical technique
An experienced colorectal surgeon performed all procedures in this study. Patients were placed in a modified lithotomy position. The chief surgeon stood at the patient's right side and the first assistant at the left. A second assistant held the camera at the patient's head. The monitor was placed at the patient's feet. In our department, a five-trocar technique is conventionally used. First, a 12-mm superumbilical port was established to create a pneumoperitoneum with a pressure of 12–15 mm Hg, and the laparoscopic camera was introduced through this trocar (trocar A). Under direct laparoscopic visualization, the other four trocars were inserted, as shown in Figure 1. Trocar E was the planned site for the sigmoid colon stoma.
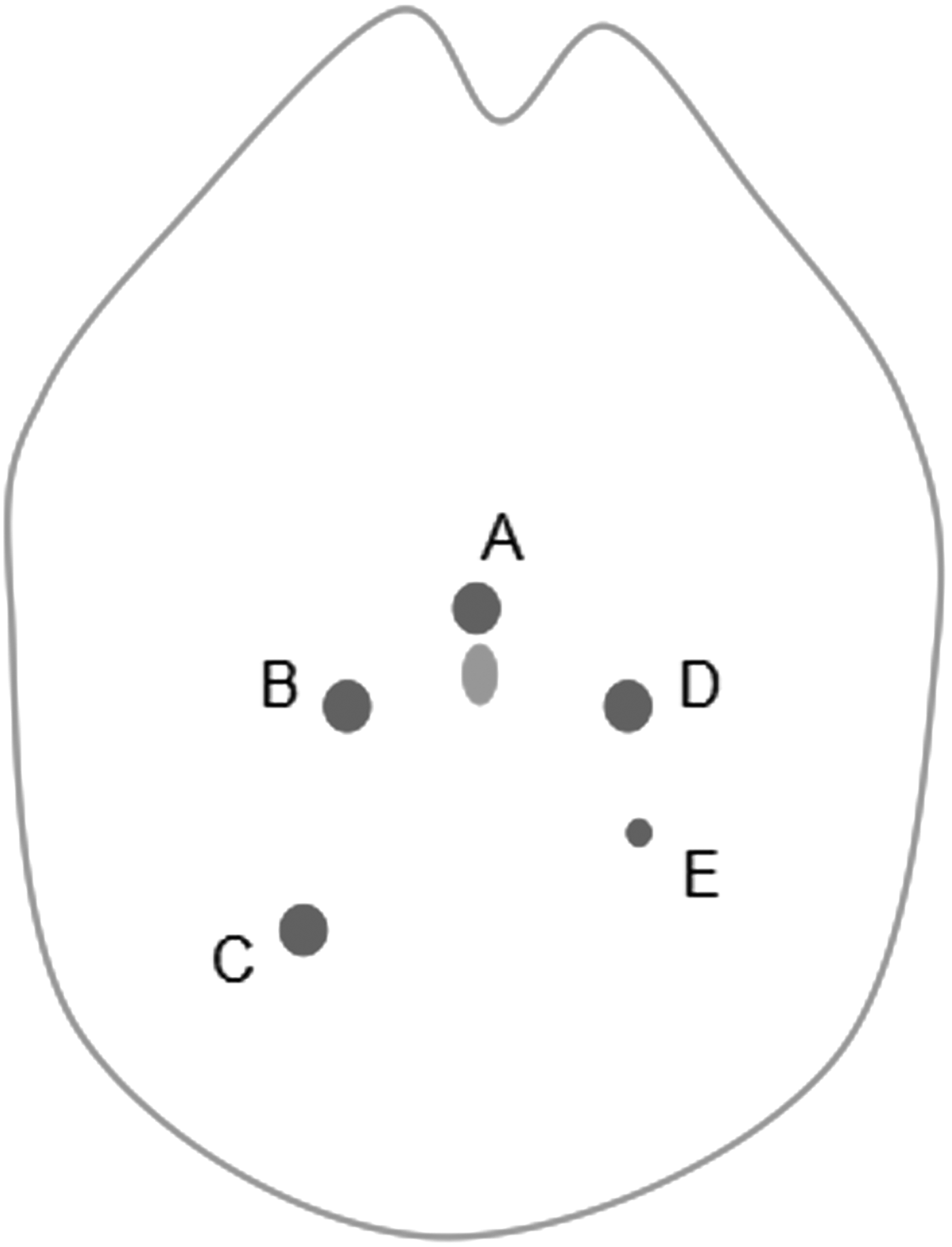
Trocar placement for laparoscopic extralevator abdominoperineal excision surgery: trocar A, 12 mm; trocars B–D, 10 mm; and trocar E, 5 mm.
ELAPE was performed in accordance with the principles described by Holm et al., 9 except that the abdominal phase was performed as a regular laparoscopic rectal surgery (Fig. 2). The mesorectum was opened along Toldt's space by an electric knife. During the procedure, the left ureter was identified and protected so that the inferior mesenteric artery could be exposed. This artery was ligated with a Weck® Hem-o-lok® (Teleflex Medical, Morrisville, NC) and cut by an ultrasonic knife at about 1 cm from its origin. Lymph nodes around the root of the inferior mesenteric artery were removed. During the abdominal portion of the surgery, the mesorectum was continually mobilized toward the origin of the levator ani muscles under direct laparoscopic visualization. This level was defined posteriorly by the apex of the coccyx bone. It was defined anteriorly by the lower edge of the prostate (for male patients) or the superior border of the anal aperture (for female patients), together with the neurovascular bundle laterally. Ureter and pelvic autonomic nerves were carefully protected during the entire procedure. After mobilization, the bowel was transected proximally with a laparoscopic linear stapler, and the proximal end of the colon was pulled out to make a colostomy at the trocar E site. Finally, all other trocar sites were closed.
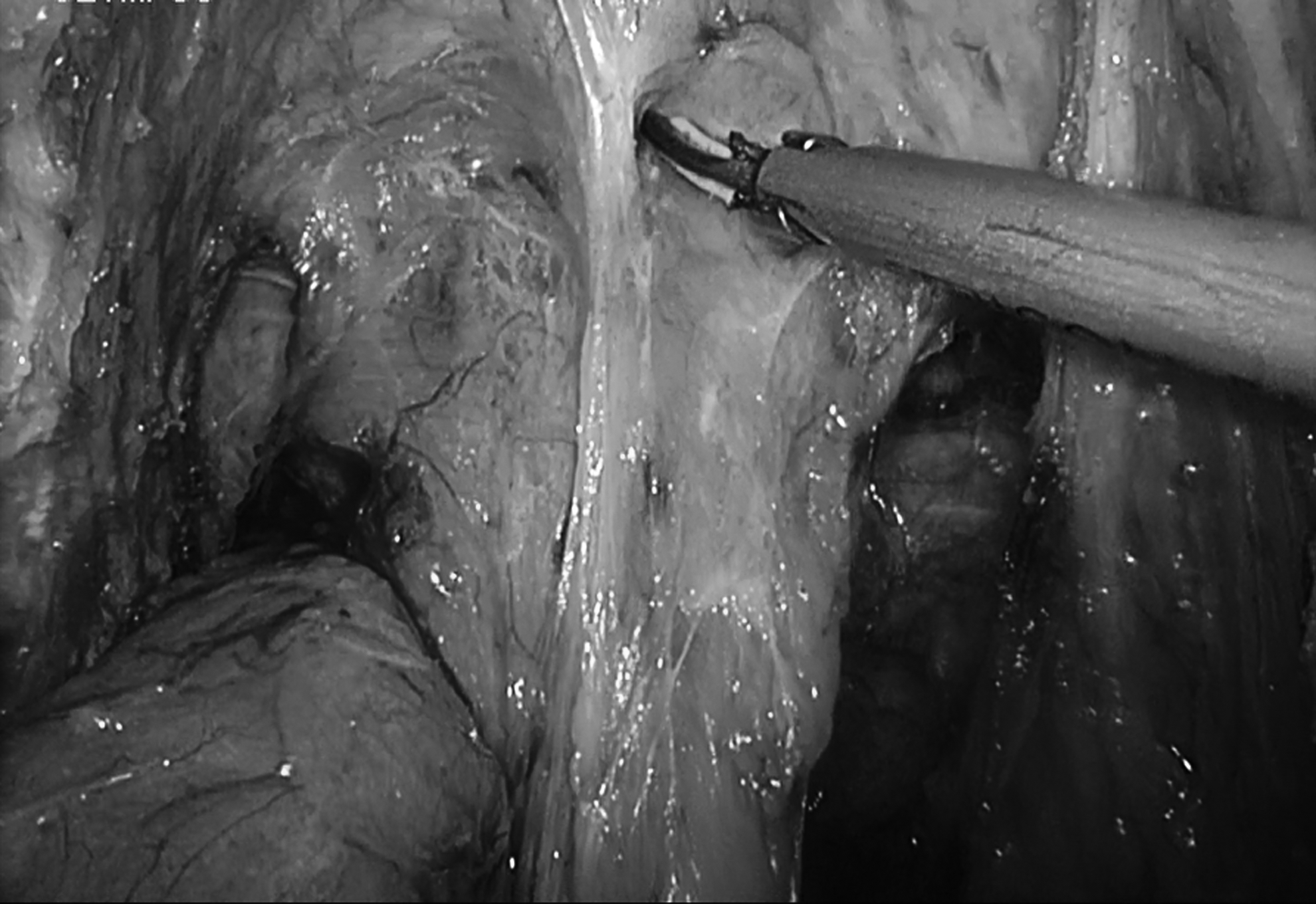
Laparoscopic approach for the abdominal phase of extralevator abdominoperineal excision.
Patients were turned to the prone jack-knife position and underwent perineal dissection. The perineal phase differed from that in sAPE. First, the anus was closed by sutures to secure against leaking, and an elliptical incision was made around the anus. Anal dissection continued outside the external anal sphincter, with preservation of the perianal skin and ischiorectal fat. Dissection continued laterally along the inferior surface of the levator muscles to the level where the muscles originate from the pelvic side wall on both sides, just inferior to the point where the abdominal and perineal dissections meet. To improve visualization of the dissection and facilitate specimen retrieval, the coccyx was routinely removed. If the posterior wall of the vagina or prostate was invaded by the tumor, then these structures were also dissected. Cylindrical specimens were removed from the perineal incision (Fig. 3).

Specimen obtained from laparoscopic extralevator abdominoperineal excision.
Our technique differs from those described in previous studies in that myocutaneous flaps or biologic meshes were not used to reconstruct perineal defects. The uterus (female patients) or peritoneum covering the surface of the bladder (male patients) was secured on the anterior surface of the sacrum with nonabsorbable sutures at a level where the anatomic structure obliterated the pelvic “outlet” (Figs. 4 and 5). Two tubes were placed in the pelvis for negative pressure drainage. The perineal wound was closed by suturing the residue of ischiorectal fossa fat, as well as perianal skin (Fig. 6).

For female patients, the uterus was secured to the anterior surface of the sacrum.

For male patients, the peritoneum covering the surface of the bladder was secured on the anterior surface of the sacrum.

The perineal wound was directly closed.
Follow-up
All patients were followed up every 3 months for the first 2 years and then annually thereafter. Exams included physical examination and blood tests, including serum tumor markers (carcinoembryonic antigen and cancer antigen 19-9). Chest and abdominal CT scans were performed every 6 months. Colonoscopies were performed 1 year after surgery and were repeated every 3 years if no lesions were found. Data were collected prospectively through telephone interview and outpatient clinic visits.
Results
Thirty-three patients underwent laparoscopic-ELAPE for low rectal cancer between January 2013 and January 2015 and were eligible for this retrospective study. Table 1 reports the demographic and preoperative clinical characteristics for patients. The median tumor distance from the anal verge was 2.5 cm. All patients had stage T3/T4 tumors on MRI. Neoadjuvant chemo-/radiotherapy was administered to 15 patients: 10 patients (30.3%) received a short course of radiotherapy, and 5 patients (15.2%) received a long course of chemoradiotherapy.
Data are median (range) values or number (%) as indicated.
ASA, American Society of Anesthesiologists; BMI, body mass index; MRI, magnetic resonance imaging.
Table 2 shows the intraoperative and postoperative information for patients. Laparoscopies were performed in all 33 patients. No patient required conversion to open surgery. The median operative time was 200 minutes (range, 115–345 minutes). The median intraoperative blood loss was 90 mL (range, 50–300 mL). There were no intraoperative tumor perforations. Bowel perforations occurred in 2 patients (6.1%), both of whom had undergone a long course of preoperative chemo-/radiotherapy. Histopathologic examinations of specimens revealed no histological evidence of tumor perforation.
Data are median (range) values or number (%) as indicated.
CRM, circumferential resection margin.
Tumor staging was pT2 in 16 patients (48.5%), pT3 in 16 patients (48.5%), and pT4 in 1 patient (3.0%). The median distance from the CRM was 8 mm (range, 0.5–17 mm). Two patients (6.1%) had tumors within 1 mm of the CRM. A median of 15 lymph nodes (range, 1–32) was harvested.
The median postoperative hospital stay was 7 days (range, 5–15 days). The median time to first postoperative flatus was 80 hours (range, 48–120 hours), and median preoperative fluid intake was 84 hours (range, 48–120 hours).
No deaths were observed within 30 days of surgery, but 5 patients (15.2%) suffered postoperative complications during this time period. Two patients (6.1%) had perineal wound infections requiring vacuum-assisted closure therapy. Two patients (6.1%) developed respiratory infections requiring intravenous antibiotics. One patient (3.0%) had a chylous fistula that did not require intervention. Two patients (6.1%) had urinary retention due to benign prostate enlargement. These patients required indwelling Foley catheters.
Table 3 reports the short-term outcomes during the follow-up period after primary suturing. The median follow-up was 12 months (range, 3–19 months). During the follow-up period, 2 patients (6.1%) had perineal dehiscence that did not require surgery. One patient (3.0%) had a perineal seroma on CT but required no drainage. One patient (3.0%) developed a bowel obstruction that only required conservative therapy. Two patients (6.1%) had chronic perineal pain requiring drugs. No case of perineal hernia, persistent sinus, peristomal hernia, or cancer-related death was observed. One patient (3.0%) did have signs of a local recurrence but had no distant metastases on a 12-month postoperative CT scan.
Discussion
The results of this study indicate that the laparoscopic-ELAPE technique is a safe and effective procedure for patients with low rectal cancer. Postoperative recovery was enhanced by the laparoscopic approach to the abdominal phase of ELAPE. With regard to short-term outcomes, primary suturing of the perineal defect after ELAPE was feasible, with an acceptable risk of perineal wound complications.
Total mesorectal excision has become the accepted surgical technique for upper and middle rectal cancers, with its use resulting in improved local recurrence and survival rates. In contrast, the surgical treatment of choice for low rectal cancer, APE, is associated with worse outcomes compared with low anterior resection in terms of local recurrence and overall prognosis. 14 Improved surgical techniques in APE are clearly needed for low rectal cancer. Recent case studies of the more radical ELAPE technique with various perineal defect reconstruction approaches have generally reported low rates of CRM involvement and improved oncological outcomes. However, these studies used an open approach to the abdominal portion of the operation.9–11,15,16 To date, ELAPE with a laparoscopic abdominal portion and reconstruction of the perineal defect by primary suturing has not been thoroughly described, and the short-term outcomes remain unclear.
Laparoscopic rectal cancer surgery has many short-term benefits, including less blood loss, faster postoperative recovery, and shorter length of hospital stay. 17 In our series these short-term benefits were confirmed when compared with ELAPE with an open approach to the abdominal portion of the operation.18–20 The large reduction in median operative time (200 minutes) was mainly the effect of using primary sutures to repair the perineal defects rather than myocutaneous flaps or biologic meshes.20,21 No laparoscopic-ELAPE procedure required conversion to open surgery. We observed no cases of tumor perforation. The incidence of bowel perforation was low compared with previous reports11,18,22 and was restricted to patients who had completed a long course of preoperative chemo-/radiotherapy. No other intraoperative complications were found. Compared with previously published results, 23 our 15.2% rate of postoperative complications not requiring re-operation can be considered as acceptable. No deaths were observed within the first 30 days after surgery. One patient (3.0%) developed a local pelvic recurrence after a median follow-up of 12 months. Histopathological examination of the lesion revealed a poorly differentiated ypT4N1 tumor with evidence of neural invasion. Two of the patient's 24 lymph nodes were positively excised, and the patient received radiotherapy to treat the local recurrence.
Compared with sAPE, ELAPE has been proposed to be associated with less CRM involvement or intraoperative perforation.4–8 Our findings confirm these observations. Pooled data from previous studies suggested that the risk of CRM involvement was 10.6% in patients who underwent sAPE. 24 In contrast, only 2 patients (6.1%) in our study had CRM involvement. West et al. 11 found that patients who underwent ELAPE, compared with those who underwent sAPE, had a significantly greater median distance from the CRM (4.0 versus 1.5 mm) and a significantly lower intraoperative perforation rate (6.4% versus 20.7%). In our study the median distance from the CRM was 8 mm, and bowel perforation was only observed in 2 patients (6.1%). Patients with low rectal cancer classified as T3 or T4 by MRI were eligible for ELAPE in our study. The 16 stage T2 tumors (48.5%) that were observed on histopathologic examination may be due to misclassification by MRI or, more likely, down-staging after the long course of preoperative chemo-/radiotherapy.
Biologic meshes and flaps have been proposed as reconstruction approaches for the perineal defect. However, the optimal method has not yet been determined. Previously described flaps have included rectus abdominis, gluteus, gracilis, and inferior gluteal artery flaps.9,25 With the myocutaneous flap approach, healthy, nonirradiated tissue is used to reconstruct a large defect after wide excisions of ischioanal fat and perineal skin. This approach has a low infection rate and tolerable risk of wound healing problems. 20 However, flap techniques require the presence of a plastic surgeon and are related to high rates of hernia development, donor-site morbidity, and flap necrosis, increased operating time, and prolonged bed rest. 20
Options for biologic meshes include cross-linked acellular porcine dermis (Permacol™; Covidien, Mansfield, MA), human acellular dermal matrix, and acellular porcine small intestinal submucosa (Surgisis® Biodesign™; Cook Biotech, West Lafayette, IN). 26 Biologic meshes have been demonstrated to be safe and effective approaches for pelvic floor repair.20,23 The techniques needed to apply biologic meshes are easy to learn, and mesh application has a shorter operating time compared with plastic surgery techniques.20,23 However, the use of biologic meshes has been limited by reports of high rates of wound infection and perineal hernia after loosening over time, bowel obstructions, latent re-admission for intraabdominal abscess drainage, and fistulae.20,23,27 Additionally, meshes are substantially more expensive than other options.
In our department, laparoscopy-ELAPE is conventionally performed with primary closure of the perineal defect. In contrast, a study found that only 20% of patients in the United Kingdom underwent a similar procedure. 28 Some authors have argued that primary closure of the perineal defect after sAPE is related to a high perineal complication rate, especially after preoperative radiotherapy. 29 This high complication rate may be because primary closure after sAPE requires tension on the sutures. Compared with sAPE, ELAPE leaves more intact perianal skin and ischiorectal fossa fat after dissection in the extrasphincteric plane. To our knowledge, the pelvis of Asian individuals is smaller than that of Western people. For these reasons, we chose to use closures with minimal tension on the primary suture.
Only 2 patients (6.1%), both of whom had received a long course of preoperative chemo-/radiotherapy, had perineal wound infections within 30 days after surgery. Although re-operation was not needed, these patients required vacuum-assisted closure therapy. During the follow-up period, 2 patients (6.1%) developed perineal wound dehiscence involving only the skin and subcutaneous tissue. Neither patient required surgery. Another patient (3%) who had not undergone preoperative therapy had a local perineal seroma that resolved on its own. One patient (3%) developed an incomplete bowel obstruction due to bowel adhesions at 16 months after surgery, which was successfully treated by conservative therapy.
One other study reported an incidence of perineal hernia after sAPE of less than 1% and proposed that this incidence was likely to be greater after ELAPE. 26 However, another study found that this rate was as high as 7% when determined by radiological screening, suggesting an underestimation of asymptomatic hernia incidence. 30 We found no cases of perineal hernia, peristomal hernia, or persistent sinus during the follow-up period.
Chronic perineal pain was reported by 2 patients (6.1%), which is an acceptable rate for this complication compared with previous studies. 23 Both patients with chronic pain required medication for pain relief and had difficulty sitting for extended periods of time. One of the 2 patients primarily complained of pain in the sacrococcygeal region, which was found to be due to local tumor recurrence. Other reasons for pain included extensive excision, coccygectomy, neuropathy, or mesh fixation to the pelvic wall.23,26
Our study has some limitations. First, this study involved a retrospective analysis of a prospectively maintained database. Thus, the study has some drawbacks due to its retrospective nature. Second, our results only reflect experiences at one institution, and the number of cases investigated was small. Multicenter prospective studies should be performed to determine the feasibility, safety, and effectiveness of the laparoscopic-ELAPE procedure.
Footnotes
Acknowledgments
We thank Wanbin He, Qingbin Wu, and Yazhou He for editing the scientific English.
Disclosure Statement
No competing financial interest exist.
X.Y., C.J., X.D., and Z.W. designed the research. X.Y., C.J., and X.D. performed the research, collected and analyzed the data, and wrote the first draft. M. Wang, Y.Z., M. Wei, and W.M. analyzed the data and edited scientific English.