
Abstract
Abstract
Introduction:
Despite leakages remaining a worrisome complication, laparoscopic sleeve gastrectomy (LSG) has become the preferred choice for most bariatric surgeons in Italy. In light of the emerging trend to discharge patients on postoperative day (POD) 1 or to consider LSG as an outpatient procedure, we felt it useful in selected cases to define a treatment protocol aimed to manage patients presenting with an acute postoperative leakage.
Patients and Methods:
Starting from 2007, 295 LSGs have been performed at our institution. Six patients, including 5 from our series (1.6%), were treated for a leak. The first patient presented a leak on POD 3, whereas the next 2 patients were re-admitted on POD 11 and 12, respectively. They all underwent a conservative treatment. The last 3 patients, according to a suggested algorithm, underwent a prompt surgical repair.
Results:
The conservatively treated patients were discharged following 22 ± 7.7 days, whereas patients treated by surgery were discharged following 10 ± 0.8 days (P = .09). By not considering the cost of primary LSG, which is about 5600 € in our region, the expense for every patient treated by re-intervention was about 2500 €. The cost for each patient treated by stenting was about 4700 €. The cost for each patient treated conservatively was about 5700 €.
Conclusions:
According to our series and in agreement with published data, it is reasonable in selected cases to consider a wider role for early surgery. A timely surgical approach following an appropriate algorithm may offer a resolutive and cost-effective answer to the management of acute leaks following LSG.
Introduction
L
Several aspects have made this procedure appealing, with the first one being the possibility to be performed rather quickly, even in superobese patients. It is reasonably easy to complete, and, according to several authors, it achieves results comparable to standard laparoscopic Roux-en-Y gastric bypass, 2 which is by far a more demanding procedure to be performed, even in skilled hands. 3
Despite the several interesting advantages offered by LSG, leakages, following this surgery, remain one of the most worrisome complications reported by bariatric surgeons. Leaks are commonly classified depending on several factors, including time of onset, clinical presentation, site of leak, radiological evidence, or a mixture of these aspects. 4 Several procedures have been investigated to prevent leaks, and although a recent meta-analysis on 8920 patients has shown a significant efficacy of the absorbable polymer membrane used as a reinforcement of the staple line, 2 the issue remains controversial. 5 On the other hand, the management of leaks following LSG remains in general a debated argument, and different algorithms have been suggested throughout the years to approach this problem.4,6–8
Although a high level of consensus has been reached by several experts about the need to treat by surgery leaks in unstable patients presenting with fever, leukocytosis, and tachycardia, 9 we felt it was useful to define a treatment protocol aimed to manage patients presenting with an acute leakage in the early postoperative period regardless of their hemodynamic conditions. This seems a particularly relevant clinical issue in the light of the emerging trend to discharge patients on postoperative day (POD) 1 or to consider LSG as an outpatient procedure in selected cases.10,11
Patients and Methods
A retrospective analysis of our prospectively maintained database of morbidly obese patients treated in our unit was performed. Starting from 2007, 295 LSGs have been performed at our institution. As this is a retrospective study, for this type of study ethical formal consent is not required.
A standard technique, extensively described elsewhere,12,13 has been routinely performed to model the gastric sleeve. As a technical detail it must be remarked that starting approximately from 2011, it is mandatory for every staff or resident surgeon in our unit to leave approximately 2 cm of gastric tissue lateral to the angle of His. Patients in our unit are allowed a liquid oral diet on POD 3, and they are routinely discharged from the hospital on POD 5. Following a 2-week period a semiliquid diet is then started. One month following surgery a semisolid diet begins. A solid diet is routinely allowed 40/45 days after primary surgery.
During this period, 5 patients from our series (1.6%) developed a leak (Table 1). According to the United Kingdom Surgical Infection Study Group, a gastric leak was defined as the leak of luminal contents from a surgical join between two hollow viscera or the loss of gastrointestinal content through a suture line, which may collect near the anastomosis or may exit through the wall or the drain. 4
False-negative.
CT, computed tomography; F, female; GE, gastroesophageal; M, male; POD, postoperative day; RX, diagnostic X-ray; TPN, total parenteral nutrition.
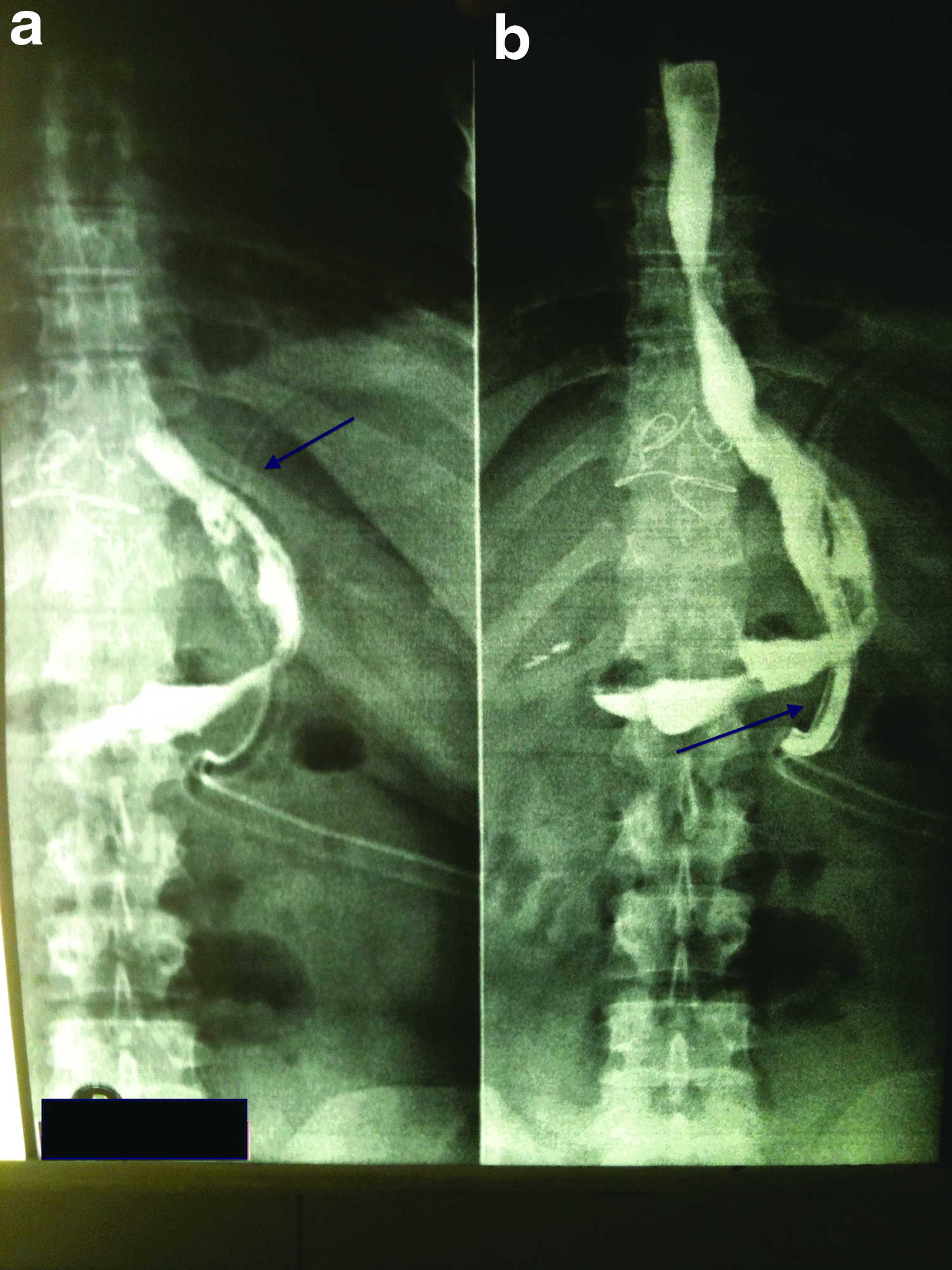
The first patient presented with a small acute 9 postoperative leak on POD 3 that was entirely evacuated by the drain tube without generating any intraperitoneal fluid collection (Fig. 1). The next 2 patients were re-admitted due to nausea, vomiting, epigastric pain, fever with a temperature of >38.5°C, and leukocytosis 6 days after discharge on POD 11 and 12, respectively. Following a computed tomography (CT) scan they received a conservative management as described elsewhere. 14 The last 2 patients, together with a patient coming from another surgical unit, presented with early-onset fever with a temperature of >38.5°C, leukocytosis, tachycardia, abdominal pain, and drain amylase level of >400 IU/L (Table 1). All 3 of these patients, according to our algorithm (Fig. 2), following a CT scan positive for leak, were scheduled for early surgery. The procedure is described below.

Algorithm of diagnosis and management. *By stapler if not located at the gastroesophageal junction. Apollo, OverStitch™ endoscopic suturing system from Apollo Endosurgery; CT, computed tomography; LSG, laparoscopic sleeve gastrectomy; OTSC, over the scope clip (OTSC®; Ovesco Endoscopy); POD, postoperative day; RYGBP, Roux-en-Y gastric bypass; stenting, Megastent from Taewoong Medical Industries.
Operative technique
An explorative laparoscopy begins by placing the patient and the trocars in the same position of primary surgery. Following a careful isolation of the greater gastric curvature, which is technically easier if carried out early after primary surgery (within 48 hours in our experience), a methylene blue test is performed by gently pushing a 36 French bougie into the gastric sleeve (Fig. 3).

A methylene blue test is performed by pushing a 36 French bougie into the gastric sleeve.
A mild degree of inflammation was present in all cases, allowing a quick separation of the omentum from the staple line. A tear size of 2.2, 2.0, and 1.8 cm, respectively, was detected, whereas an abscess cavity of 3.0, 3.1, and 4.0 cm, respectively, was found.
As the tear is identified, a series of three to four stitches is then passed to achieve an optimal traction on the edges of the leak (Fig. 4).
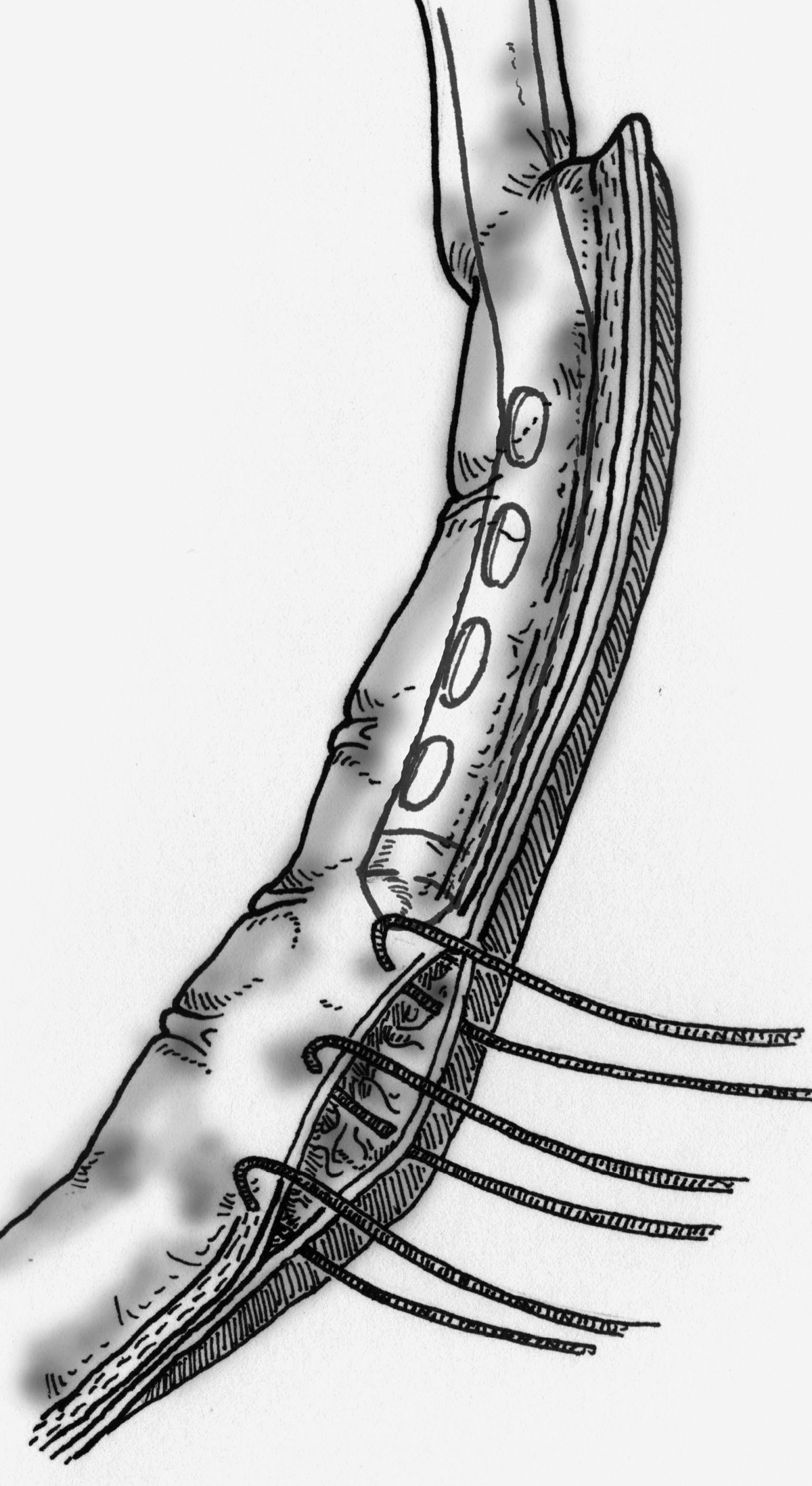
A series of three to four stitches is then passed to have an optimal traction on the edges of the leak.
Following this step, as the bougie is pushed down to avoid postoperative strictures (Fig. 5), a stapler is placed across the tear. Then, while a grasper holding the stitches is gently moved toward the left flank of the patient, the stapler goes in the opposite direction before being closed and fired (Fig. 6). This is to encompass the undamaged staple line, above and below the tear, within the stapler bite. In all three cases a linear stapler (Echelon Flex™ 60 Endopath®; Ethicon®, Cincinnati, OH) loaded with a “gold” cartridge (staple height of 3.8 mm) was used. No buttressing material has been ever used for primary or revision LSG.

As the bougie is pushed down to avoid postoperative strictures, a stapler is placed across the tear.

While a grasper holding the stitches is gently moved toward the left flank of the patient, the stapler goes in the opposite direction before being closed and fired.
A new methylene blue test is then performed; subsequently, the repair is completed by a thorough washout of the abdominal cavity and by the placement of two drain tubes, one aligned to the staple line and another one surrounding the spleen, below the diaphragm. A nasogastric tube is left into the stomach for the first 24 postoperative hours.
Results
Our series included 6 patients overall. The first patient recovered following 25 days of total parenteral nutrition; she never developed, fever, leukocytosis, or septic intraperitoneal collection and remained relatively asymptomatic. At the end of this period she was allowed an oral diet and discharged on POD 33. The second and the third patients were discharged from the hospital on POD 16 and 17 from primary surgery, respectively, following the endoscopic placement of a Megastent® (Taewoong Medical Industries, Kangseo-Gu Songjung-Dong, South Korea). They both fully recovered in about 8 weeks. Nevertheless, during this period they were allowed to assume an oral diet due to the presence of the stent. 14 Finally, the 3 patients treated by the above-described procedure were allowed an liquid oral diet 5 days following the second surgical repair and were discharged in good condition, on POD 9, 11, and 10, respectively, from primary surgery (Table 1).
By considering patients treated conservatively, the mean discharge period was 22 ± 9.5 days, whereas patients treated by surgery were discharged following 10 ± 1.0 days (P = .09, t test). If we do not consider the cost of primary LSG, which is about 5600 € in our region, the expense for every patient treated by re-intervention was about 2500 €. The cost for a patient treated with a Megastent was about 4700 €. The cost for a conservatively treated patient was about 5700 €.
Discussion
LSG has become a mainstream operation in the treatment of morbidly obese patients.2,3 Although it is usually considered a mere restrictive procedure, some other advantages have been reported when compared with other interventions. The hormonal effect produced by the decreased levels of ghrelin and glucagon-like peptide 1, the accelerated gastric emptying, the absence of implanted material, the persistence of normal gastrointestinal continuity, the avoidance of malabsorption, and, finally, the opportunity to convert LSG into either a laparoscopic Roux-en-Y gastric bypass or a biliopancreatic diversion–duodenal switch if needed 13 have led many experts to consider LSG as a valid stand-alone procedure.3,9
Despite the appealing features of this surgery, postoperative complications following LSG, and especially leaks, remain a major concern. The mortality rate for LSG is about 0.3%, and its morbidity is lower than 15% in qualified centers, 2 decreasing to 5.6% if we consider the strict perioperative period. 13 Conversely, the staple line leak rate may reach 7%,2,15–18 increasing up to 18% if we consider leaks located at the gastroesophageal junction; however, even in these latter cases, a decreasing trend is being reported, 19 with a leak-related mortality of 0.1%. 2 Although the debate is still open on which diagnostic modality is the most sensitive and specific to detect a post-LSG leakage, most surgeons agree that early identification is associated with better outcome. 20 According to a wide panel of experts, leaks may be classified depending on the time of occurrence following surgery as acute, early, late, and chronic. Acute leaks in particular are those seen within the first 7 days postoperatively. 9
Our algorithm of leak detection and management (Fig. 2) aims to define both the ideal diagnostic approach and the eventual surgical timing for those lesions observed before patient discharge from the hospital, within POD 5 in our experience.
The starting point remains the clinical suspicion4,20 of a leak. The vast majority of these complications present with clear findings: 81.1% with fever and 75% with leukocytosis of >10,000 mm3 according to Csendes et al., 6 although both findings appeared in 100% in our smaller experience. At present, when a leak is suspected we have abandoned swallow upper gastrointestinal contrast diagnostic X-ray with diatrizoate meglumine and diatrizoate sodium solution (Gastrografin®; Bayer, Leverkusen, Germany), due to the high rate of false-negative results (33% in our experience; Table 1). These data are widely supported by published series. In fact, Mittermair et al. 21 and Wahby et al. 22 reported an alarming 100% (50% in the experience of Sakran et al. 20 ) rate of false-negative diagnostic X-ray following LSG, confirming the proposal that the upper gastrointestinal study is useless, especially when it is performed within POD 2.6,23,24
Conversely, CT scan of the abdomen with intravenous and water-soluble contrast, even at a very early stage, remains the best noninvasive approach for detection and confirmation of a gastric leak in our experience and most other series.4,6,18,20
Although a common view about the management of leaks arising following patient discharge from the hospital, usually on POD 5–6, is still lacking, despite several reported experiences,4,7,25 a general agreement exists about the need to perform a surgical re-exploration in patients presenting with fever, leukocytosis, tachycardia, and abdominal pain in the suspicion of an acute leak.3,5,9 Different opinions are, however, reported in these patients as well; in fact, whereas some authors favor a conservative management of acute leaks if patients, although symptomatic, are in a stable hemodynamic condition,7,25,26 others suggest prompt surgery in these cases as well.4,6,27
The early surgical management of acute leaks is in our opinion warranted by some considerations coming from published studies. According to Baker et al., 28 leaks may be classified as early, appearing within POD 5–6, and late, presenting later. Early leaks are caused by mechanical faults or tissue injury, whereas late leaks arise on an ischemic basis. Because the vast majority of leaks occurred within POD 2, it has been concluded that most are due to mechanical/tissue issues.
It should be underlined that, although observations of Baker et al. 28 about true ischemic leaks being rare are well documented, these have been made before the wide diffusion of LSG. In fact, according to a more recent systematic review from Aurora et al., 18 79% of all LSG leakages are reported as late events occurring past POD 10, being located at the gastroesophageal junction in 89% of cases. If these data may appear in contrast with the conclusions of Baker et al., 28 on the other hand they seem to confirm the proposal that the majority of LSG leaks are late because they are arising on an ischemic basis, in a potentially dangerous area such as the gastroesophageal junction, at the level of the angle of His, as explained in a previous review study. 29 Results from the large series of Bellanger and Greenway 30 of 529 LSGs without any reinforcement of the staple line and without any postoperative leakage, where the technical concept to leave approximately 1 cm of gastric tissue lateral to the angle of His is strictly enforced, seem to support this view.
In light of these findings, we consider it correct to suggest a surgical approach in all those leak cases presenting within POD 2 because of the high probability that the leak would be successfully repaired when caused by mechanical faults or tissue injury. This is likely the consequence of the good tissue perfusion observed, 28 which provides a generally good response to suturing, regardless of the surgical technique being used.6,20,27,31 Furthermore, at this very early stage, the inflammatory response with subsequent tissue thickening is still low,4,20,32 thus allowing a good performance to surgery. By considering our series of 295 LSGs, 60% of leaks (3 out of 5 patients) have been diagnosed within POD 2, thus being classified as due to mechanical faults or tissue injury.
In our opinion this is due to the strict observation of two technical points of paramount importance thoroughly described. The first one is the compression for about 20 seconds of the gastric tissue with the stapling device, which promotes proper staple formation and reduces both serosal trauma and bleeding 28 ; the second is stapling about 2 cm away from the esophagus, in the area of the angle of His.9,30 If a 40% rate of late leaks (2 out of 5 patients) may appear in contrast with the data of Aurora et al. 18 of 79% of late leaks, it must be noted that starting from 2011 we only observed acute leaks.
Cost remains an issue. The expense for a single bariatric procedure is in our region about 5600 €, increasing by about 2500 € in the case of a re-intervention. 33 The cost for every single day of hospital stay exceeding POD 7 is about 220 €. The cost of an esophageal stent is about 2500 €. Although esophageal stenting is reserved for those patients presenting with late leaks and therefore not suitable for surgery,4,7,9,14 it is worth noting that in our series, leak-caused re-admissions were shorter, although not significantly, if patients were re-approached first by surgery. This is confirmed by other larger experiences. Sakran et al. 20 detected a trend for longer leak resolution in the patients managed nonoperatively (50 days) than in those who underwent an early operation (20 days).
Our algorithm, supporting a surgical approach in the suspicion of an acute leak following LSG, presents nevertheless some limitations. The first one is represented by the small number of patients treated in our series. It would be interesting to verify, in larger patient series, if an early surgical approach may significantly improve the outcome of patients presenting an acute leak following LSG. The second bias is represented by the fact that the proposed procedure, due to obvious technical limits, cannot deal with leaks presenting at the gastroesophageal junction.
The presently described algorithm is designed to cover the first 5–6 days postoperatively. Although among large patient numbers only 20% of leaks occur within the first 48 hours, whereas the remaining 80% of cases arise following POD 2, 20 this algorithm can be adopted both by surgeons opting for an early discharge in selected patients10,11,19 or by surgeons opting for a longer perioperative observational period, as usually occurs in countries where the national healthcare system covers all medical expenses. In conclusion, according to our series and in agreement with published data,4,6,20,27,32 it is reasonable in selected cases to consider a wider role for early surgery. A timely surgical approach following an appropriate algorithm may offer a resolutive and cost-effective answer to the management of acute leaks following LSG.
Footnotes
Acknowledgments
The authors would like to thank Prof. Maurizio Taglialatela for his valuable support in drafting this manuscript.
Disclosure Statement
No competing financial interests exist.