
Abstract
Abstract
Purpose:
Several studies have demonstrated that laparoscopic colonic resection has significant benefits in comparison with open approaches in patients with benign and malignant disease. The proportion of colonic and rectal resections conducted laparoscopically in Austria is not currently known; the aim of this study was to evaluate the current status of laparoscopic colonic surgery in Austria.
Materials and Methods:
A questionnaire was distributed to all general surgical departments in Austria. In collaboration with IMAS, an Austrian market research institute, an online survey was used to identify laparoscopic and open colorectal resections performed in 2013. The results were compared with data from the National Hospital Morbidity Database (NHMD), in which administrative in-patient data were also collected from all general surgical departments in Austria in 2013.
Results:
Fifty-three of 99 surgical departments in Austria responded (53.5%); 4335 colonic and rectal resections were carried out in the participating departments, representing 50.5% of all NHMD-recorded colorectal resections (n = 8576) in Austria in 2013. Of these 4335 colonic and rectal resections, 2597 (59.9%) were carried out using an open approach, 1674 (38.6%) were laparoscopic, and an exact classification was not available for 64 (1.5%). Among the NHMD-recorded colonic and rectal resections, 6342 (73.9%) were carried out with an open approach, and 2234 (26.1%) were laparoscopic.
Conclusions:
The proportion of colorectal resections that are carried out laparoscopically is low (26.1%). Technical challenges and a learning curve with a significant number of cases may be reasons for the slow adoption of laparoscopic colonic surgery.
Introduction
T
Laparoscopy for colonic resection was introduced in 1991.13,14 Initial concerns (which included, for example, the length of the learning curve, the possible development of port-site metastases, and the possibility of inadequate oncologic resection) subsequently proved unfounded.15–18 In recent years, several studies have confirmed the adequateness of the laparoscopic approach and have also shown that it has several short-term functional benefits, with equivalent long-term results. A recent meta-analysis by Lorenzon et al. 19 provided evidence supporting the use of laparoscopic procedures in relation to several short-term outcomes, including less blood loss, earlier recovery of bowel function, an earlier return to oral intake, a shorter hospital stay, and a lower morbidity rate.
Despite these well-documented advantages, there has been relatively slow progress in translating the scientific evidence into clinical practice. A survey in Britain and Ireland in 2009 revealed that 25% of 12,077 procedures in 1 year were performed with laparoscopic assistance. 20 Data on adoption rates, regional variations, and factors determining whether laparoscopic colorectal surgery is being incorporated into routine practice are not available in the literature. The extent to which laparoscopic colonic and rectal resections are performed nationally throughout Austria is not currently known. The aim of the present study was therefore to evaluate the current status of laparoscopic colonic surgery in Austria in 2013.
Materials and Methods
In collaboration with the Institut für Markt-Sozialanalysen (IMAS), an Austrian market research institute, an online survey was used to identify laparoscopic and open elective colon and rectal resections performed in Austria from January 1 to December 31, 2013. IMAS is a company engaged in market and social analysis.
IMAS carried out the data collection, processing, and analysis for the present study. The questionnaire was sent to 99 surgical departments in Austria; contact data for them were provided by the Second Surgical Department at the General Hospital in Linz, Austria. The participating departments were standard hospitals for primary care (general public hospitals for primary care) and private hospitals, as well as teaching hospitals and university hospitals, in addition to hospitals run by the church with public care.
The study was initially conducted online, but the Department in Linz also sent out direct links to the respondents, who completed the questionnaire from January 7 to 23, 2014. To increase the response rate, a reminder was sent out by e-mail, and potential respondents were also contacted through computer-assisted telephone interviews for participation in the study. Finally, a written survey (with a paper and pencil questionnaire) was sent out from March 26 to April 15, with the deadline extended until April 28, 2014. The data returned were input into the database by IMAS. After the online survey, we started with telephone querying in all missing clinics. Furthermore, IMAS provided support to make the acquisition of the data as easy and comfortable as possible.
The questionnaire was designed by the Second Surgical Department at the Johannes Kepler University Hospital in Linz, and IMAS included eight questions and three demographic inquiries on the numbers and types of colonic and rectal resection carried out in Austria in 2013, with a special focus on open versus laparoscopic operations. Colonic and rectal resections were divided into ileocecal resection, right hemicolectomy, left hemicolectomy, sigmoid resection, rectal resection, Hartmann procedures, and “others.” No distinction was made in the survey between acute and elective indications for colonic resection.
Statistical analysis
IMAS reviewed and analyzed the data using internal software for analysis, with a binary-column data format. Standard descriptive statistics such as absolute counts and calculation of means, minimums, maximums, and standard deviation were used.
In addition to the questionnaire survey, data were obtained from the National Hospital Morbidity Database (NHMD), which annually collects administrative in-patient data from all general surgical departments in Austria. Data extraction was restricted to patients who had undergone colonic and rectal resection; no information was collected in connection with indications.
No data capable of identifying (or re-identifying) any individual patients or hospitals were provided. The NHMD extracted data on the basis of an individual medical procedure code (Medizinischer Einzelleistungs [MEL] code), the code used for reimbursement purposes in Austria for various medical procedures, given in the MEL catalog (a listing of all reimbursed medical procedures).
The results of the survey were then compared with the data from the NHMD. This comparison showed the information value of the survey and the extent to which laparoscopic colonic surgery has currently been adopted.
Results
Fifty-three of 99 surgical departments in Austria took part, representing a response rate of 53.5%. Colonic and rectal surgery was performed in 50 of the participating surgical departments (94%). Three departments (6%) did not provide any exact details regarding colonic and rectal surgery. The total number of colonic and rectal resections carried out in the participating departments was 4335, representing 50.5% of all MEL-coded colonic and rectal resections (n = 8576) conducted in Austria from January 1 to December 31, 2013. Of these 4335 colonic and rectal resections, 2597 (59.9%) were carried out using an open approach, 1674 (38.6%) were performed laparoscopically, and no exact classification was available for 64 (1.5%) (Fig. 1). Among the MEL-coded colonic and rectal resections in Austria, 6342 (73.9%) colonic and rectal resections were conducted using an open approach, and 2234 (26.1%) were performed laparoscopically in 2013 (Fig. 2).
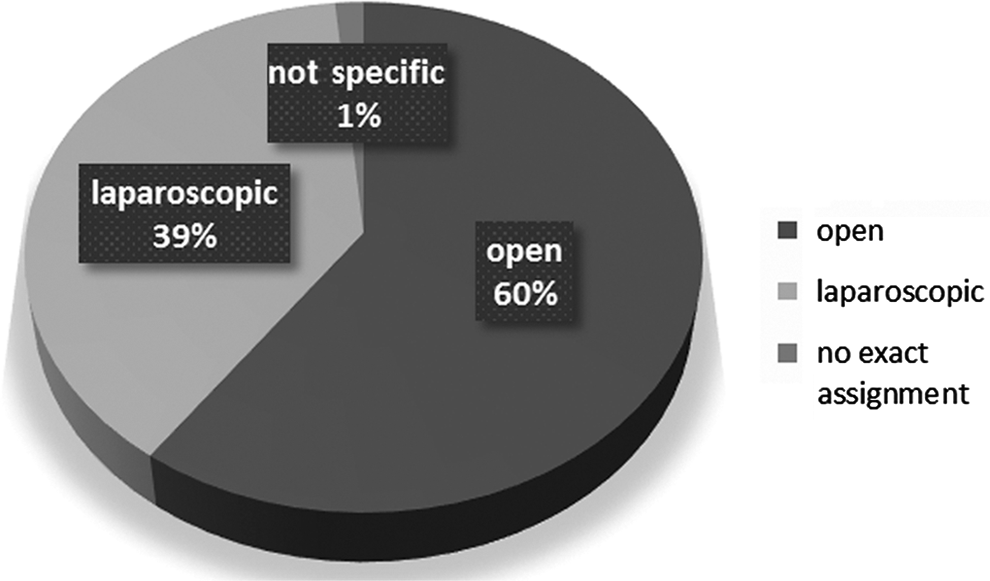
Percentages of colonic resections conducted laparoscopically and with an open approach in Austria in 2013, among the departments participating in the survey.

Percentages of colonic resections conducted laparoscopically and with an open approach in Austria in 2013: data from the National Hospital Morbidity Database.
The survey found that 2597 colonic and rectal resections were primarily carried out as open procedures, including 217 ileocecal resections, 630 right hemicolectomies, 352 left hemicolectomies, 269 sigmoid resections, 416 rectal resections, 298 Hartmann procedures, and 415 others (Table 1 and Fig. 3). The term “others” includes oversewing, conditioning of a coecostomy, or transversostomy.
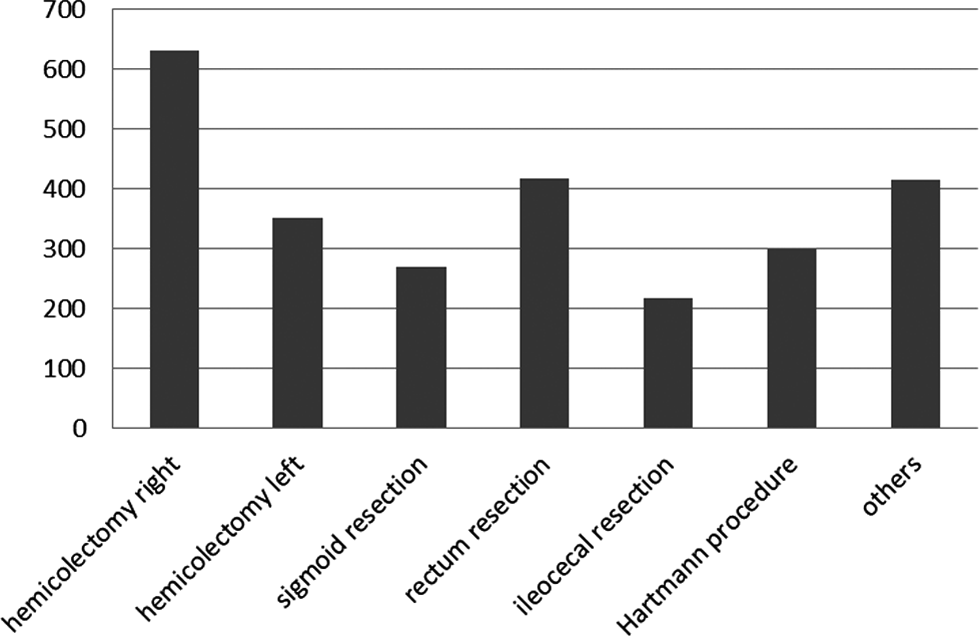
Open colonic and rectal resections in the survey. The term “others” includes oversewing, conditioning of a coecostomy, or transversostomy.
Data are number (%). The term “Others” includes oversewing, conditioning of a coecostomy, or transversostomy.
In comparison with the data from the NHMD, 6342 MEL-coded colonic and rectal resections were primarily carried out as open procedures, including 1810 right hemicolectomies, 287 resections of the transverse colon, 1578 left hemicolectomies, 316 subtotal colectomies, 41 proctocolectomies, 43 rectopexies with resection, 308 rectal resections without mesorectal excision, 759 rectal resections with mesorectal excision, 230 abdominoperineal rectum amputations, and 970 Hartmann procedures (Fig. 4).
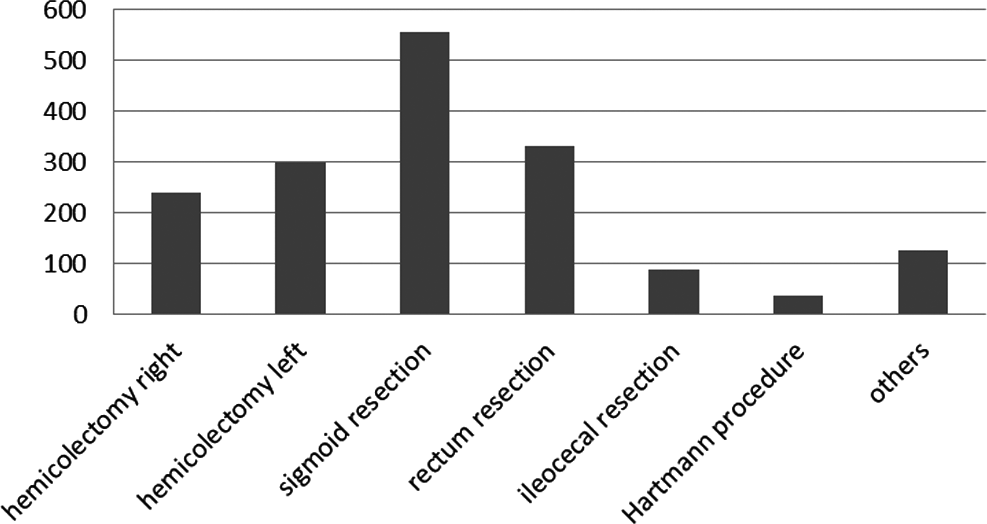
Laparoscopic colonic and rectal resections in the survey. The term “others” includes oversewing, conditioning of a coecostomy, or transversostomy.
The findings from the questionnaire showed that 1674 colonic resections were performed laparoscopically, including 88 ileocecal resections, 239 right hemicolectomies, 300 left hemicolectomies, 554 sigmoid resections, 330 rectal resections, 38 Hartmann procedures, and 125 others (Fig. 5). Conversion to an open approach was required in 122 cases. Table 2 shows the number of conversions relative to the different procedures; conversion rates are given as percentages.
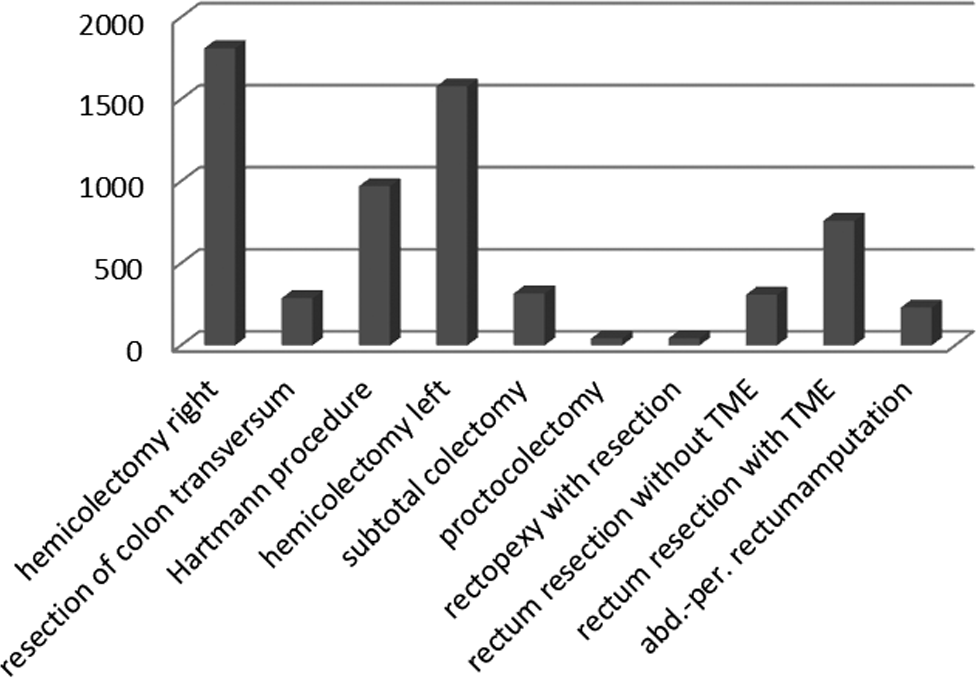
Medizinischer Einzelleistungs–coded open colonic and rectal resections in the survey. abd.-per., abdominoperineal; TME, total mesorectal excision.
The term “Others” includes oversewing, conditioning of a coecostomy, or transversostomy.
In the data extracted from the NHMD on laparoscopic colonic and rectal resections, there were 2234 MEL-coded laparoscopic colonic and rectal resections, including 250 right hemicolectomies, 23 resections of the transverse colon, 1239 left hemicolectomies, 58 subtotal colectomies, 17 proctocolectomies, 36 rectopexies with resection, 219 rectal resections without mesorectal excision, 317 rectal resections with mesorectal excision, and 17 abdominoperineal rectum amputations (Fig. 6). Table 3 lists the MEL codes for all of the procedures.
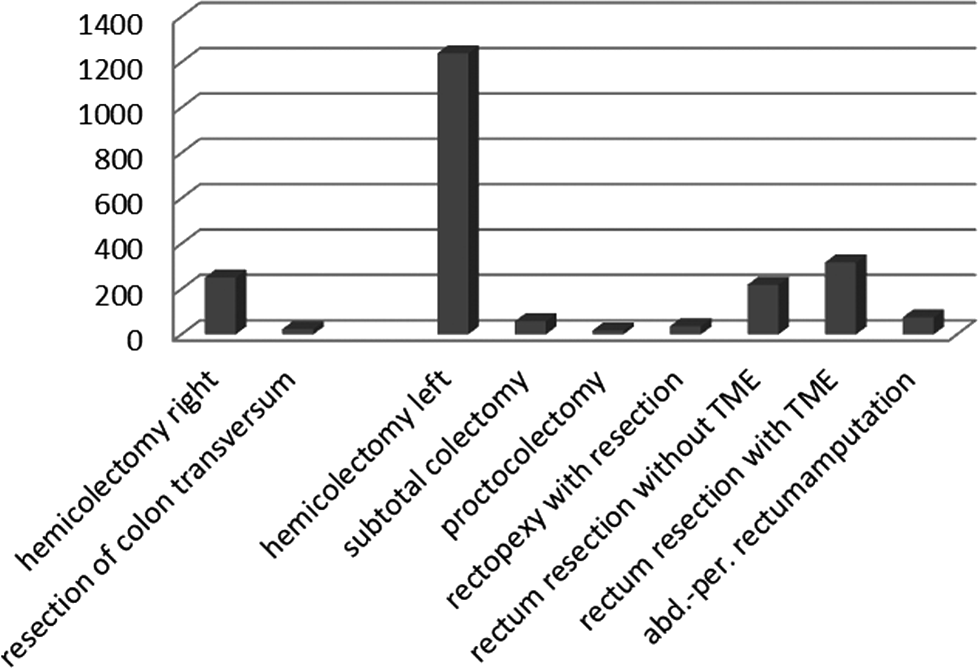
Medizinischer Einzelleistungs–coded open colonic and rectal resections in the National Hospital Morbidity Database. Abd.-per., abdominoperineal; TME, total mesorectal excision.
Medizinischer Einzelleistungs code (national code for different procedures, for reimbursement purposes).
In patients with malignant carcinoma, 46 departments (92%) would not exclusively choose a primary open approach, whereas 2 departments would choose a primary approach. Two surgical departments did not respond. In response to the question “What were the reasons for an open procedure?,” 40% of the departments stated that it was carcinoma, 3% adenoma, 21% inflammation, 3% higher costs, and 15% lack of training, whereas 18% gave other reasons (Fig. 7).
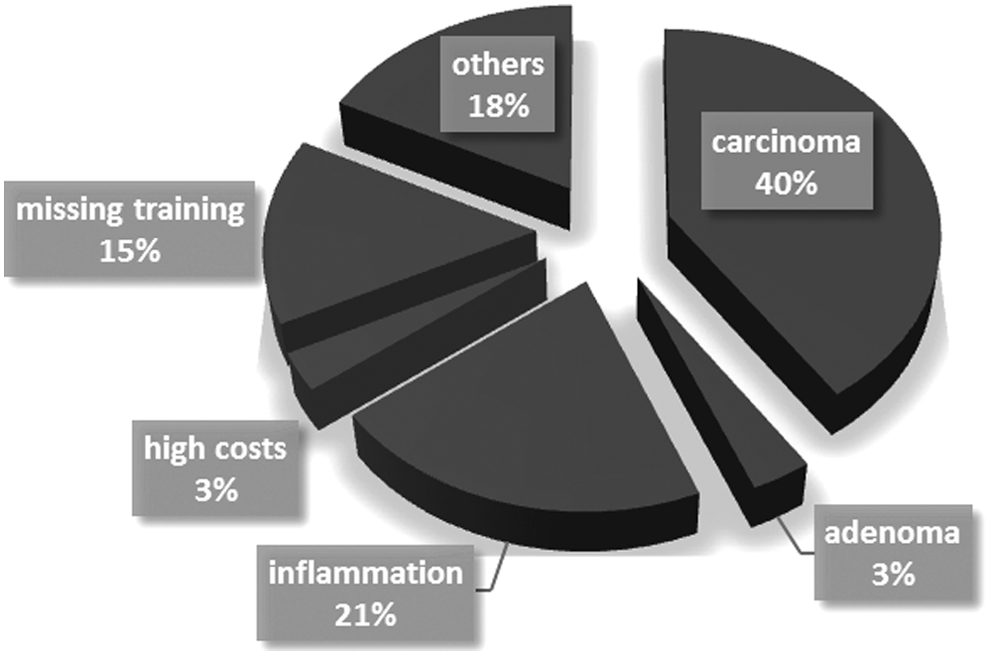
Reasons for colonic and rectal resections being conducted by the openprocedure.
Thirty surgical departments (60%) stated that laparoscopic colonic surgery was also appropriate as a teaching operation, 14 departments (28%) considered that it was not, and 6 departments (12%) did not specify a response.
Single-incision laparoscopy operations were carried out in 21 surgical departments (42%), 27 departments (54%) said that such operations were not carried out, and 2 departments (4%) did not specify a response.
The participating departments were standard hospitals for primary care in 50% of cases, whereas 21% were in specialist hospitals, 3% were in private hospitals, and 26% were in religious hospitals.
A total of 320 consultant surgeons (range, 1–17; standard deviation, ±3) and 125 residents (range, 1–5; standard deviation, ±1) worked at the participating departments.
Discussion
The survey, with a response rate of 53.5%, included 50.5% of all colonic and rectal resections carried out laparoscopically and as open procedures in Austria in 2013. The proportion of laparoscopic colonic and rectal resections in the survey was 38.6%. By contrast, the data from the NHMD showed that 26.1% of colonic and rectal resections were performed laparoscopically. Although the real percentage of laparoscopically performed colonic and rectal resections was lower than the results of the survey, the percentages of operations carried out laparoscopically or as open procedures were similar in the survey results and in the data from the NHMD. The most commonly performed laparoscopic procedures in the survey were left hemicolectomy (33.1%) and sigmoid resection (17.9%). In the MEL-coded colonic and rectal resections for Austria, the proportion of laparoscopically performed left hemicolectomies (including sigmoid resection) was 55.5%.
Certain barriers to laparoscopic colonic resection were identified in the study. The main reason given was carcinoma, although 92% of the respondents stated that they would not exclusively choose a primary open approach in case of carcinoma. This result was unexpected in a country in which there are advanced laparoscopic skills such as Austria. Recent data show that laparoscopic procedures for colon cancer resection are oncologically safe. 21 A meta-analysis by Morneau et al. 22 in 2013 showed that laparoscopy is not inferior to open surgery for the curative treatment of colon and rectal cancer in relation to overall survival, disease-free survival, and recurrence rates. In addition, laparoscopic surgery also has short-term advantages over open surgery—in particular, shorter hospital stays, a reduced need for analgesics, faster recovery of intestinal function, and an earlier return to activities of daily life. 22
A lack of training was mentioned by 15% of the survey respondents as a reason for carrying out an open procedure. Technical challenges and a learning curve with a significant number of cases led to slow adoption of laparoscopic colonic surgery. A systematic review by Miskovic et al. 23 suggested that the learning curve may involve 88–152 cases.
The survey showed that costs were not a reason for choosing an open procedure. Recent studies have reported that laparoscopic resection for colon and rectal cancer leads to lower costs, with an equivalent quality of life. 24
A survey on the use of laparoscopic surgery among colorectal surgeons in Britain and Ireland in 2004 found that only 45 of 200 surgeons were performing any laparoscopic colorectal surgery; the response rate in the survey was 37% (200/540). 25 Five years later, a survey of accredited colorectal surgeons in Britain and Ireland showed that 25% of 12,077 procedures in 1 year were performed with laparoscopic assistance and that 53% of colorectal consultants were using laparoscopy. 20 Comparing these results with our survey, there is still a low adoption rate of laparoscopic colonic surgery. The rate of laparoscopic colonic resections had not increased in the last 5 years.
Conclusions
On the basis of evidence-based medicine, the majority of elective colonic and rectal resections should be performed laparoscopically. Unfortunately, this is not the case. Even in a laparoscopically advanced country such as Austria, the proportion of laparoscopically performed colonic and rectal resections is low (26.1%). It can be assumed that the percentage of laparoscopically conducted colonic and rectal resections is above 50% only in a few specialized hospitals in Austria; 94% of the respondents in the present survey offer laparoscopic colonic surgery.
Technical challenges and a learning curve with a significant number of cases may be one of the reasons for the slow adoption of laparoscopic colonic surgery. The proportion of laparoscopically conducted colonic and rectal resections can be increased.
Footnotes
Acknowledgments
Support for the statistical analysis was provided by the Medical Society of Upper Austria (Medizinische Gesellschaft für Oberösterreich).
Disclosure Statement
No competing financial interests exist.