
Abstract
Abstract
Background:
It is often difficult to perform percutaneous radiofrequency ablation (RFA) for hepatic tumors beneath the diaphragm. Diaphragmatic thermal damage is one of the fatal late complications of percutaneous transdiaphragmatic RFA. Our experience with laparoscopic transthoracic transdiaphragmatic intraoperative RFA (LTTI-RFA) for hepatic tumors beneath the diaphragm is reported.
Methods:
Ten patients who underwent LTTI-RFA from 2009 to 2012 were evaluated. Two cases had concomitant partial hepatectomy, and one underwent RFA for two tumors at the same time. The diagnosis was hepatocellular carcinoma in eight cases and metastatic hepatic tumors in two cases. Nine of eleven tumors were located at segments 7 and 8. Nine tumors were less than 20 mm in diameter. The patients were placed in the half left lateral decubitus position with single-lumen tube intubation. After placement of four abdominal ports, a 12-mm port was inserted in the fourth or fifth intercostal space into the diaphragm. The tumor was ablated by an RFA needle through the port. The routine follow-up consisted of laboratory tests and abdominal imaging every 3–6 months.
Results:
The median operation time for only one tumor was 137 minutes (range, 105–187 minutes). The median number of times for ablation was three. Severe postoperative complications (>Clavien–Dindo IIIa) were observed in one case (right upper limb paralysis). The median follow-up period was 35 months (range, 11–43 months). There was no local tumor progression. Recurrent hepatic tumor appearance occurred in other parts of the liver in 6 of the 11 patients.
Conclusions:
Laparoscopic transthoracic transdiaphragmatic RFA is an acceptable procedure with a low rate of local recurrence.
Introduction
T
Patients and Methods
Patients
Ten patients (5 men, 5 women) with histologically proven malignant primary and metastatic hepatic tumors who underwent LTTI-RFA from January 2009 to December 2012 were retrospectively reviewed.
Indications for LTTI-RFA
The following were the indications for LTTI-RFA: (1) patients in whom it would be difficult to perform percutaneous RFA and (2) hepatic tumor diameter was less than 30 mm and the tumor was located at the surface of the liver, or there were multiple resectable tumors for which laparoscopic liver resection and LTTI-RFA would be combined. For patients with resectable liver malignancies without previous therapy, various types of hepatectomy were performed. For patients with tumor diameter over 30 mm or with three or more tumors, conservative hepatectomy was the preferred option. Conservative hepatectomy was also performed for tumors with major vessel invasion.
Operative procedure of LTTI-RFA
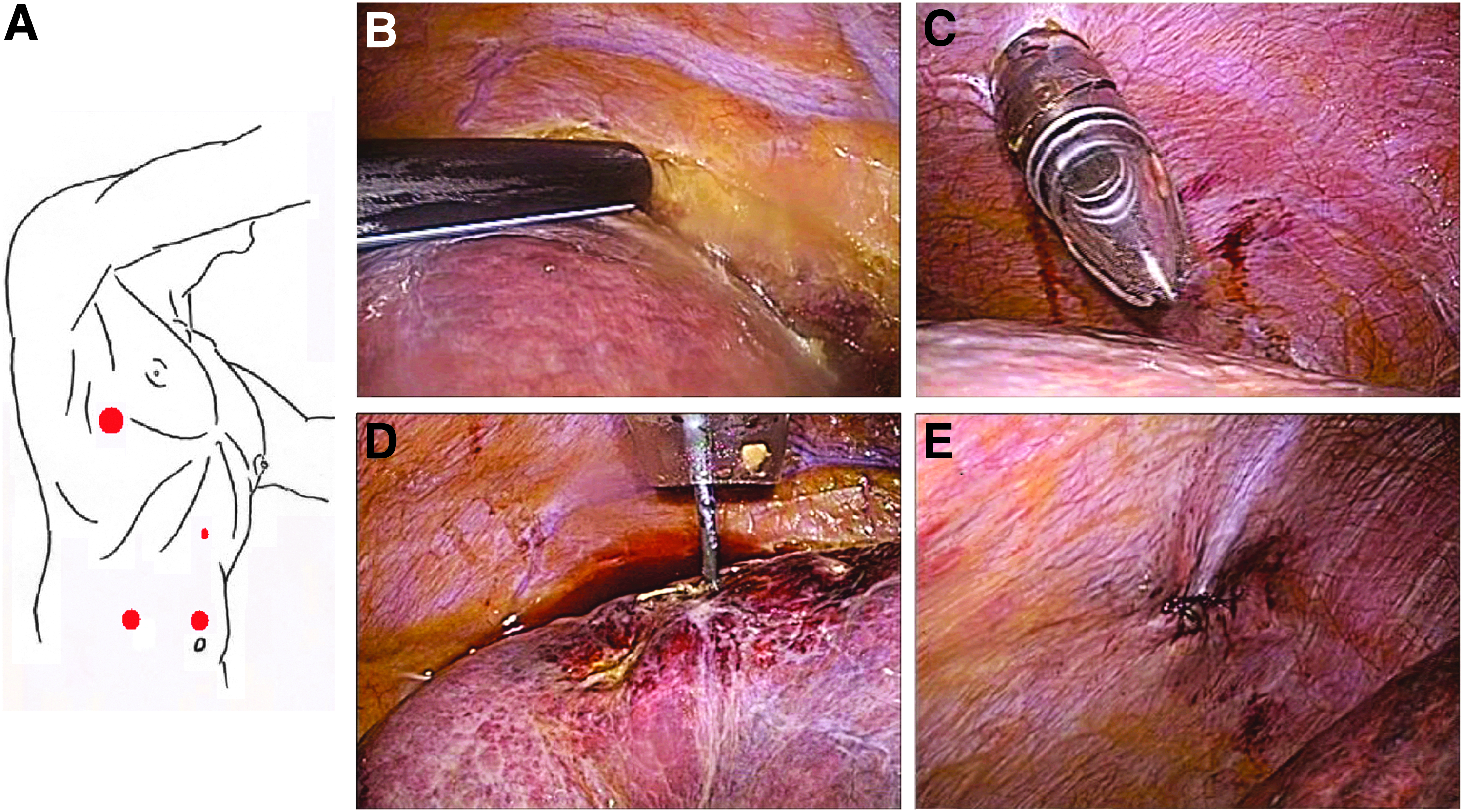
The operative procedure of LTTI-RFA was usually performed under general anesthesia with single-lumen tube intubation. The patient was placed in a half left lateral decubitus position. Four ports were placed in the abdomen as usual. Then, laparoscopic ultrasonography of the liver was performed to identify the liver lesions using a 7.5-MHz Aloka rigid, linear, side-viewing, 10-mm, laparoscopic transducer (Aloka Co., Ltd., Wallingford, CT). An electric device was used to burn a mark on the surface of the liver to show the position of the tumor on ultrasonography. The 12-mm port in the fourth or fifth intercostal space of the anterior axillary line was inserted just at the position of the tumor through the chest cavity under optical guidance (Optiview™; Ethicon Endo Surgery, Inc., Blue Ash, OH). The diaphragm was punctured through the intercostal port. The Cool-tip™ RF ablation system (Covidien, Boulder, CO) was used for intraoperative RFA, and thermal ablation was performed at 10–140 W. The fully opened electrode provided four pulses after the temperature of the electrode had reached 80°C or was maintained for 6 minutes. The Cool-tip RF Ablation Single Electrode Kit (Covidien) consists of a 460- to 480-kHz generator, a 17-gauge, 20-cm-long, internally cooled electrode with a 2.0- to 3.0-cm-long exposed metallic tip and a dispersive pad applied to the patient's skin. The tumor was ablated several times. The ablation lesion with RFA formed a triangle or square surrounding the tumor. Finally, the diaphragm was sutured using a laparoscopic suture technique. A chest tube was placed through the intercostal port (Fig. 1).
Postoperative complications and follow-up
The routine follow-ups consisted of clinical physical examinations, laboratory tests as appropriate, including tumor markers, and abdominal imaging (ultrasonography, magnetic resonance imaging, and/or computed tomography (CT) on a case-by-case basis) every 3–6 months.
The recurrence pattern was divided into two groups: local recurrence and remote recurrence. Local recurrence was defined as any new tumor within 2 cm of the ablation zone. Remote recurrence was defined as any new tumor more than 2 cm from the ablated nodule.
Statistical analysis
Recurrence-free survival (RFS) was defined as the time to the earliest local recurrence, measured from the date of ablation. The Kaplan–Meier method was used to estimate RFS. All analyses were performed with statistical software (Stat-View J version 5.0; SAS Institute, Inc., Cary, NC).
Results
Patient characteristics
Table 1 shows the patient characteristics. There were eight patients with HCC and two patients with colorectal metastases. The tumors were mainly located at segment 7 or segment 8. A total of 11 ablations were performed for 10 patients. Eight of 10 patients had a history of RFA treatment. The other patients had no history, but they would have had difficulty with surgical resection.
Numbers are medians, and numbers in parentheses show the range of each parameter.
ICG, indocyanine green; RFA, radiofrequency ablation.
Operative results
The median operation time was 137 minutes (range, 105–187 minutes). The median operation time was calculated using data from only seven patients who underwent RFA for only one tumor during the procedure. The median number of ablation times for one tumor was three (range, 2–7 times). All tumors could be detected by intraoperative ultrasonography or laparoscopy.
Severe postoperative complications (Clavien–Dindo classification ≥IIIa) were found in one case; the patient had right upper limb paralysis due to the intraoperative position. The postoperative courses of the other patients were uneventful. The median hospital stay was 16 days (range, 14–167 days).
Median survival and recurrence
The median follow-up period was 35 months (range, 11–43 months). No patient developed local recurrence. There was no case that had a diaphragmatic hernia and peritoneal dissemination recurrence during the follow-up period. Six patients had remote recurrence; all were thought to be multicentric recurrences, and four of them were recurrent within 1 year (Fig. 2).
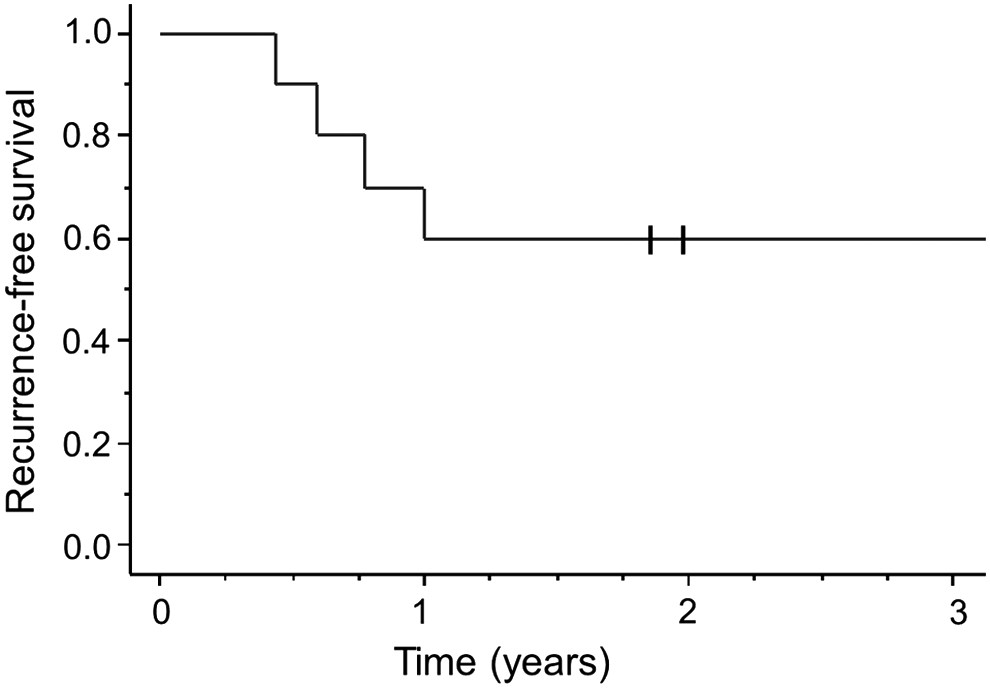
Kaplan–Meier curves showing recurrence-free survival rates after RFA. Four patients had multifocal recurrences within 1 year of the RFA. RFA, radiofrequency ablation.
Discussion
The results of this analysis suggest that LTTI-RFA is an acceptable procedure for small hepatic tumors located beneath the diaphragm, with some benefits. First, this procedure appeared feasible from the oncological perspective. No patients had local recurrence, and there were no peritoneal recurrences after the procedure. Second, this procedure can be performed safely because there were no cases of diaphragmatic hernia or bile leakage after the procedure.
Several therapeutic strategies have been used for hepatic tumors located beneath the diaphragm, including open hepatectomy, laparoscopic hepatectomy, RFA, and transcatheter arterial chemoembolization. The most common strategy is surgical intervention, such as open and laparoscopic liver resection. In general, open liver resection is thought to be a useful procedure for hepatic tumors, because open liver resection appears to have a low recurrence rate, but it is the most invasive procedure. 7 In contrast, previous reports showed that local recurrence rates after laparoscopic RFA were 8%–13%.8–11 Topal et al. 12 reported that accurate placement of the RFA cannula under laparoscopic ultrasound guidance into tumors, especially deep tumors in segments 6, 7, or 8, is technically demanding and at times impossible; successful laparoscopic RFA is highly surgeon dependent.
Possible alternative procedures would be RFA with artificial pleural fluid, CT-guided transthoracic percutaneous RFA, and laparoscopic 13 /thoracoscopic14–16 (dual-scope) RFA. However, these procedures can have some problems. One possible complication following the procedure is a fatal diaphragmatic hernia due to heat injury. There have been five reported cases of diaphragmatic hernia following the procedure. Diaphragmatic injury was not a common complication, but potentially fatal; two of five previously reported cases died.17–21 To prevent diaphragmatic heat injury, we try to insert the RFA needle through the thoracoscopic port and suture the diaphragmatic defect directly after the ablation. The other possible limitation is the difficulty to infuse the artificial saline in a case with adhesions associated with a history of thoracic or abdominal surgery or RFA. The laparoscopic RFA procedure has been reported to be safe for treating hepatic tumors22–27 and has the advantage of being able to determine the tumor stage exactly, using intraoperative ultrasonography.
The other complication of RFA was thought to be peritoneal dissemination. Kang et al. 13 reported that there may be a risk of tumor spillage into the peritoneum during the laparoscopic RFA procedure. Therefore, we tried to ablate a tumor several times from the circumference, and we selected a vertical route as the shortest distance to the tumor. We think that we were able to ablate with a high local control rate by ablating several times and thus preventing peritoneal metastasis. In the present study, 4 of 10 patients developed multicentric recurrence within 1 year. RFA is the suitable treatment for these patients who had already undergone locoregional treatment, because of the high rate of remote recurrence and less invasiveness.
Our review of the literature yielded only one report of a laparoscopic transthoracic transdiaphragmatic approach to hepatic ablation therapy. Kang et al. 13 performed percutaneous transthoracic transdiaphragmatic RFA by both thoracoscopic and laparoscopic approaches; theirs was a case report. The operation was performed with three abdominal ports, one thoracic port, and one puncture for a 1.5 cm metastatic tumor in the liver dome. The difference from the present cases was that the RFA needle punctured the diaphragm directly. The report did not discuss the long-term follow-up. The report mainly suggests that percutaneous transthoracic transdiaphragmatic RFA was successfully performed under the combined guidance of thoracoscopic and laparoscopic approaches. However, we think that the transthoracic transdiaphragmatic RFA procedure without thoracoscopy can be performed with only one thoracic wound of less than 5 mm, because it was easy to collapse the lung after insertion of the thoracic port in the cases with no thoracic adhesion.
Our procedure appears to have three limitations. With this procedure, it might be difficult to find small and highly differentiated tumors intraoperatively, because most tumors beneath the diaphragm could not be detected by preoperative percutaneous ultrasonography. Furthermore, it was especially difficult to access the tumors in patients with a prior laparotomy. Transdiaphragmatic RFA with thoracoscopy alone14–16 is similar to our method. Patients with dense intra-abdominal adhesions may be best approached using a transthoracic method, but this requires special equipment, such as an end-fire laparoscopic probe, 11 and the tumor cannot be directly confirmed visually using thoracoscopy. Finally, our procedure needs to be performed under general anesthesia. One of the patients developed right upper limb paralysis due to the intraoperative position. This complication caused a long hospital stay and decreased the patient's quality of life. Because this complication is rare with percutaneous RFA performed with the patient awake, LITI-RFA is considered to be useful in patients with tumors that are difficult to treat with conventional percutaneous RFA.
In conclusion, although the procedure was performed in a small number of patients, our laparoscopic transthoracic transdiaphragmatic RFA has a low recurrence rate and appears to be an adequate alternative therapy in patients with tumors located beneath the diaphragm.
Acknowledgment
This research received no funding or grant support.
Footnotes
Disclosure Statement
No competing financial interests exist.