
Abstract
Abstract
A 15-year-old girl was found to be hypertensive (230–270/140–170 mm Hg) without any subjective symptoms. Magnetic resonance imaging confirmed the presence of a well-defined 22 mm hypodense lesion in the lower pole of the left kidney, located close to the renal hilum. Plasma rennin activity was elevated (75 ng/mL/h), and reninoma was diagnosed. Retroperitoneoscopy-assisted nephron-sparing surgery was planned. The retroperitoneum was accessed through a 4 cm left pararectal upper abdominal incision. Following blunt dissection, the abdominal wall was elevated with a lifting bar and lifting retractor, inserted below the 12th rib in the anterior axillary line to create sufficient working space in the retroperitoneal cavity without the need for pneumoperitoneum. Three 5 mm trocars were introduced above the superior iliac crest for the camera and the assistant. Gerota's fascia was opened and the kidney exposed. The surgeon dissected the left kidney through the minilaparotomy incision under both direct vision and using the magnified view on the monitor, which was particularly effective for the lateral and posterior sides of the kidney. The posterior peritoneum was incised intentionally next to the diaphragm to allow further mobilization of the kidney. Diathermy was used to remove the tumor and a layer of surrounding normal parenchymal tissue at least 0.5 cm thick. The histopathologic diagnosis was reninoma. Ischemia time was 14 minutes. Postoperatively, both plasma rennin activity and blood pressure were normal (1.9 ng/mL/h and 90–110/70–80 mm Hg, respectively). After follow-up of 12 months, there is no evidence of recurrence.
Introduction
J
The conventional treatment for reninoma has been open nephrectomy, but in recent years, nephron-sparing surgery, specifically laparoscopic, has been recommended to preserve renal function and prevent complications,2,3 because the natural history of reninoma is generally benign.
We report a case of severe hypertension secondary to reninoma treated by retroperitoneoscopy-assisted nephron-sparing surgery in a 15-year-old girl. We describe and discuss the treatment, focusing on retroperitoneoscopy-assisted surgical techniques.
Case Report
A 15-year-old girl was referred for investigation of proteinuria detected during a routine school health checkup. She was asymptomatic. Her height was 148 cm, weight was 45 kg, and she had mental retardation, but no family history of hypertension. On admission, clinical assessment was unremarkable except for elevated blood pressure of 230–270/140–170 mm Hg. Serum electrolytes were normal, and plasma aldosterone was normal (249 pg/mL). However, the plasma rennin activity was elevated, (75 ng/mL/h) and renal function, as indicated by blood urea nitrogen and serum creatinine, was slightly compromised (BUN: 17 mg/dL; creatinine: 1.27 mg/dL). Ultrasonography (US) identified a hypoechoic mass in the left kidney. Computerized tomography (CT) and magnetic resonance imaging (MRI) confirmed a well-defined hypodense lesion, 22 mm at the greatest diameter in the lower pole of the left kidney, located close to the renal hilum (Fig. 1).
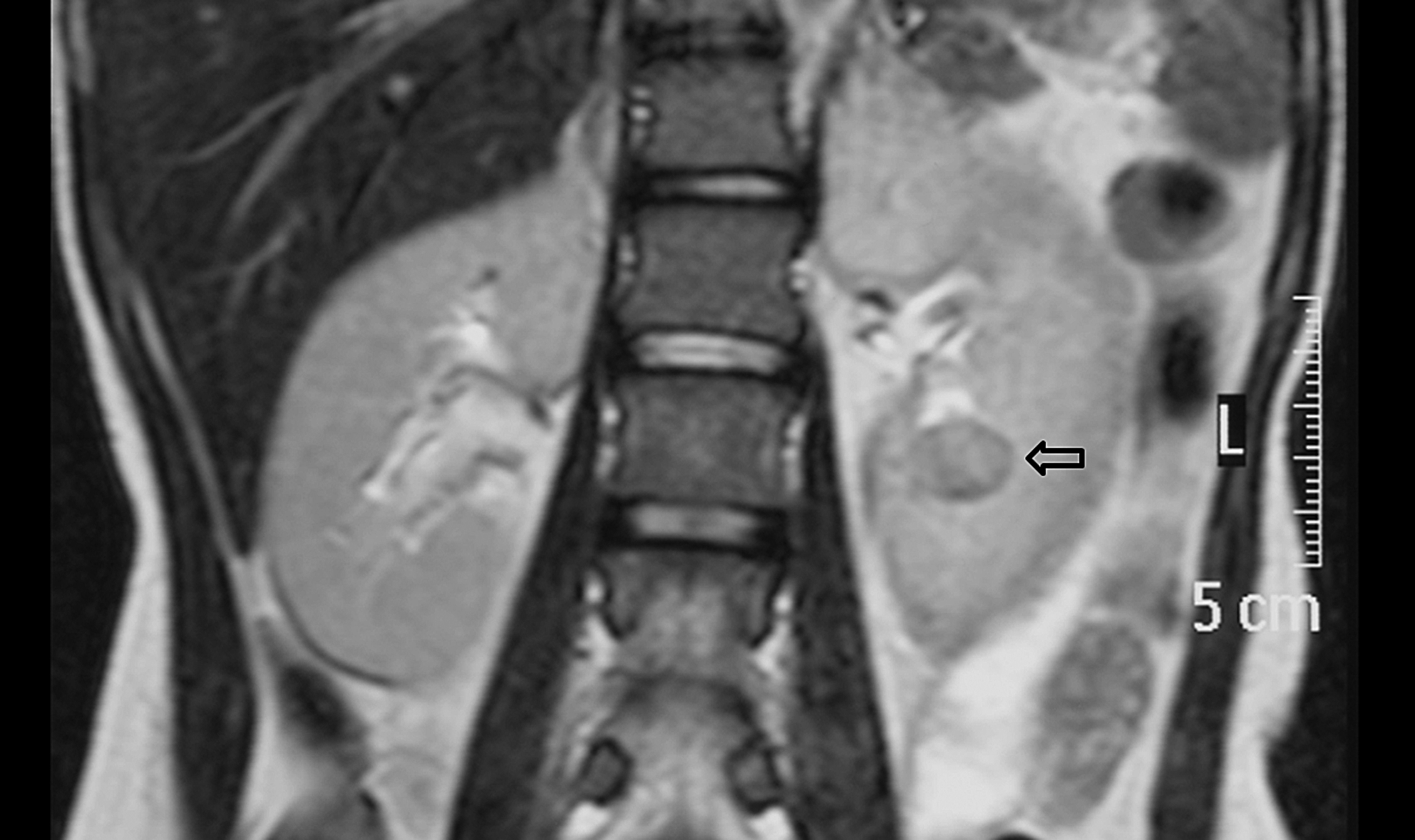
Magnetic resonance imaging (MRI) confirmed a well-defined hypodense lesion, maximum diameter of 22 mm in the lower pole of the left kidney, located close to the renal hilum.
Taking into consideration the small size of the mass and its proximity to the renal hilum, partial nephrectomy or lower pole heminephrectomy was considered and surgical resection was commenced under general anesthesia with the patient in a semilateral position. A 4 cm left pararectal incision was made in the upper abdomen and the retroperitoneal space accessed by blunt dissection. An Alexis wound retractor® (Applied Medical, Rancho Santa Margarita, CA) was placed in the pararectal wound and the abdominal wall lifted up with a lifting bar and metal plate lifting retractor to 1 cm below the 12th rib in the anterior axillary line that was attached to the abdominal wall inside (Fig. 2). Using this technique, sufficient working space could be created in the retroperitoneal cavity without the need for insufflation. Trocars were introduced under direct vision; a 5 mm trocar was inserted 1 cm above the superior iliac crest in the mid-axillary line as a camera port, and two additional 5 mm trocars were inserted in the anterior and posterior axillary lines slightly below the first camera port, for instruments to apply countertraction and suction.
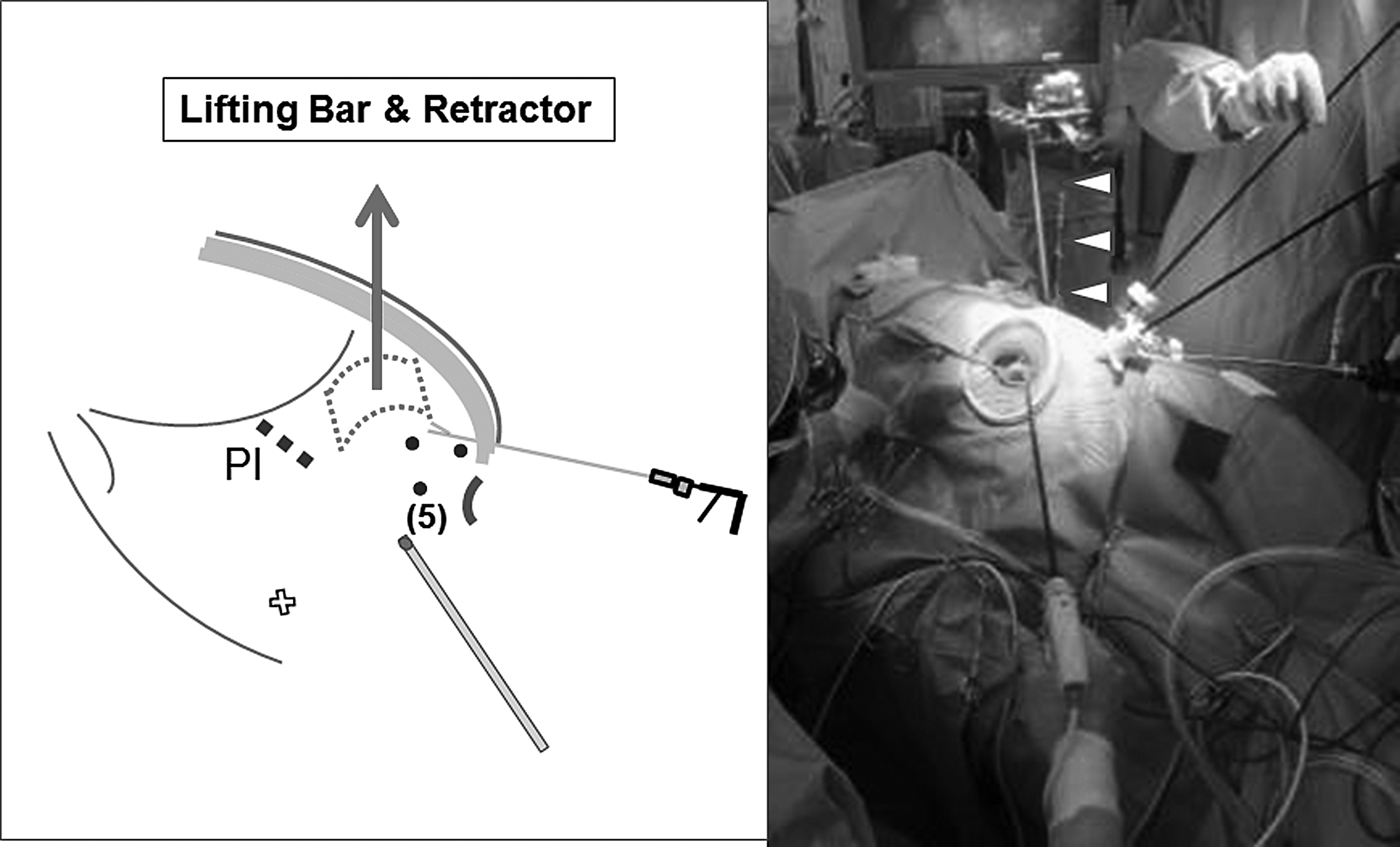
The abdominal wall has been elevated with a lifting bar and a lifting retractor (arrow [Lt], arrow heads [Rt]) comprising a metal plate inserted 1 cm below the 12th rib in the anterior axillary line and fixed to the abdominal wall internally. PI, pararectal incision; (5), three 5 mm trocars.
The operating table was then tilted so that the patient was more lateral, and Gerota's fascia was opened and the kidney exposed. The pararectal incision and trocar ports allowed us to use forceps and scissors used conventionally for open surgery, and the surgeon was able to dissect the left kidney through the pararectal incision under both direct vision and by referring to the magnified view on the monitor, which was particularly effective for dissecting the lateral and posterior aspects of the kidney. To facilitate safe dissection, especially between the tumor and the renal hilum, the peritoneum was opened intentionally using the cautery near the diaphragm (Fig. 3) to facilitate more meticulous dissection to mobilize the kidney to the surface (Fig. 4) through the pararectal minilaparotomy incision. The renal vessels were dissected free, and the renal artery clamped with a Satinsky clamp. A Harmonic Scalpel was used to remove the tumor with a margin of normal parenchyma of at least 0.5 cm (Fig. 5). Excision of the tumor was thus performed as an open procedure. Hemostasis was achieved by suturing with continuous 3-0 Vicryl® (Ethicon, Inc., Cincinnati, OH), and the renal parenchyma was further reconstructed with 3-0 V-Loc (Covidien, Cincinnati, OH) system continuous sutures, without injuring the caliceal system. Intraoperative blood loss was 70 mL. Ischemia time was 14 minutes. The tumor was well encapsulated and its cut surface was white. Histology and immunohistochemistry identified that the tumor cells had nuclear dysmorphism and numerous cytoplasmic renin granules (Fig. 6).
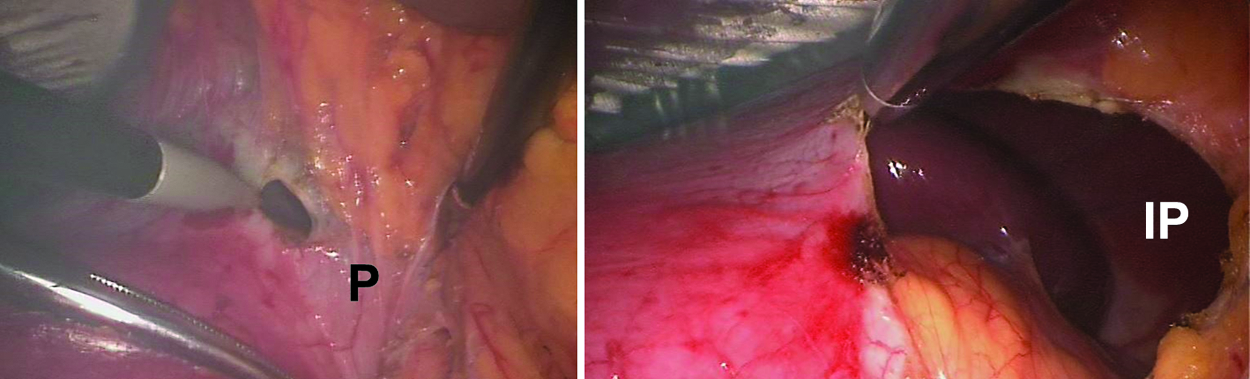
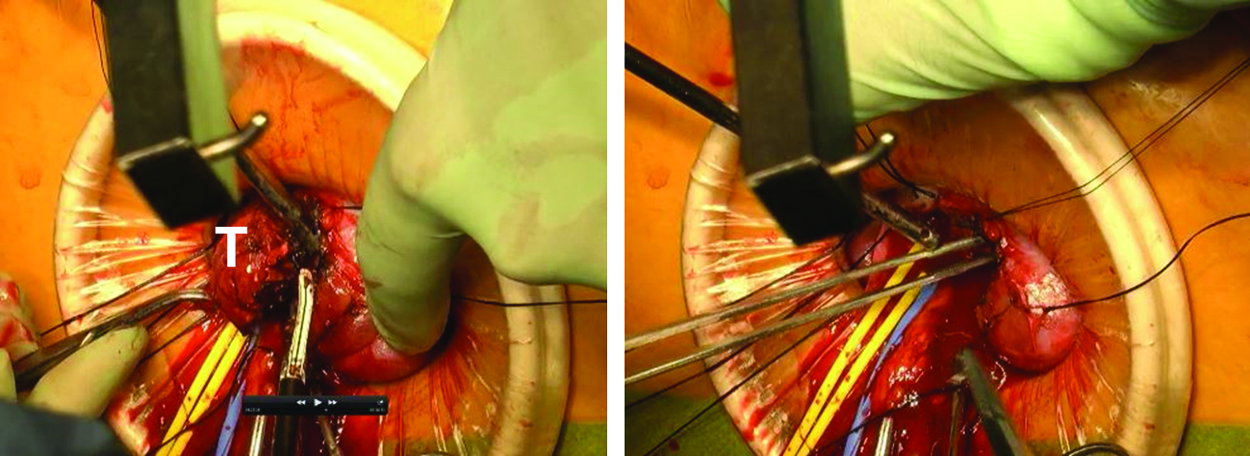
The posterior peritoneum opened intentionally using cautery next to the diaphragm to facilitate dissection of the tumor from the renal hilum. P, peritoneum; IP, intraperitoneal space.
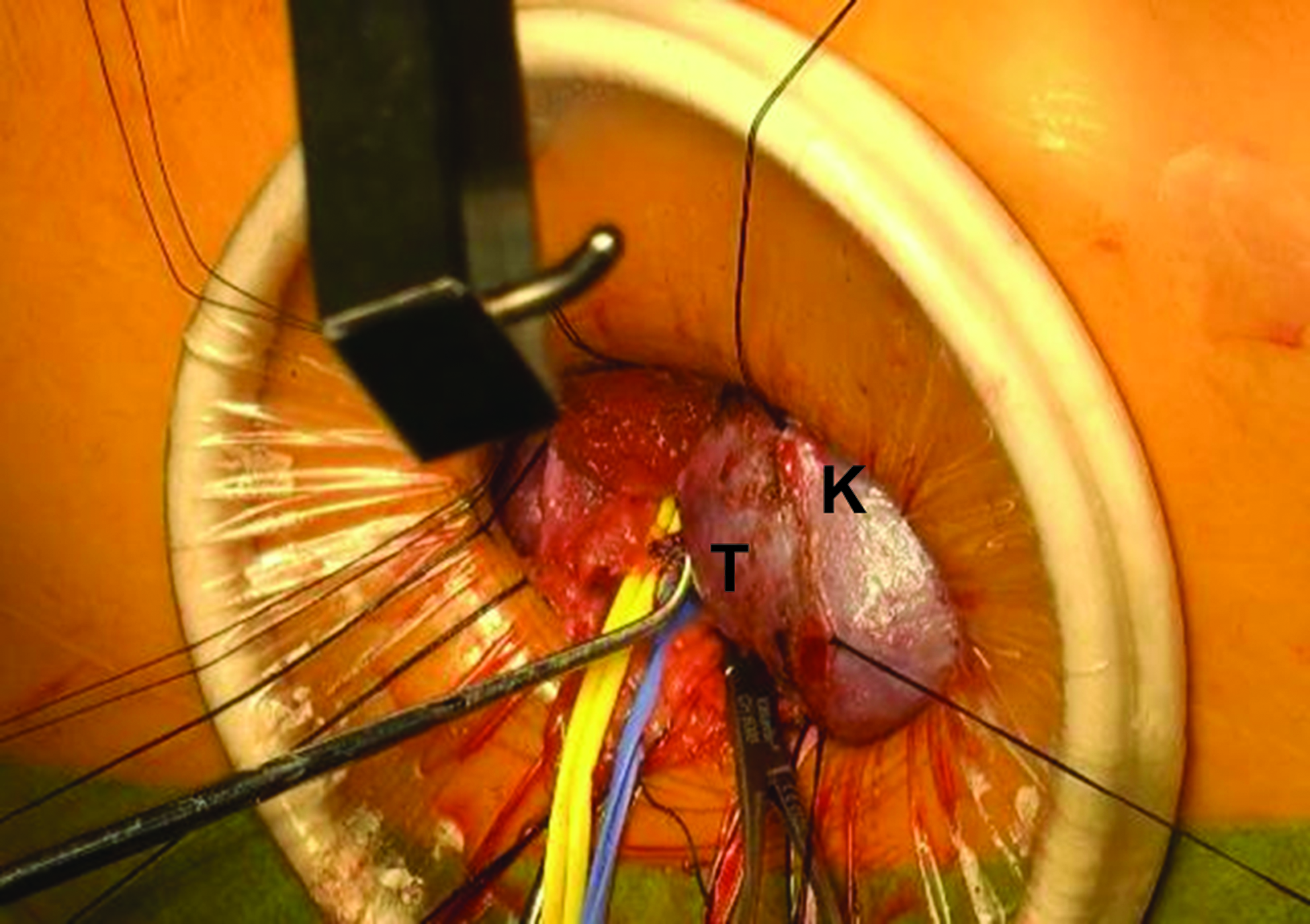
The kidney can be mobilized extracorporeally through the pararectal upper abdominal incision, because the peritoneum has been opened posteriorly. T, tumor; K, kidney.
A Harmonic Scalpel was used to remove the tumor with a 0.5 cm margin of normal parenchyma. T, tumor.
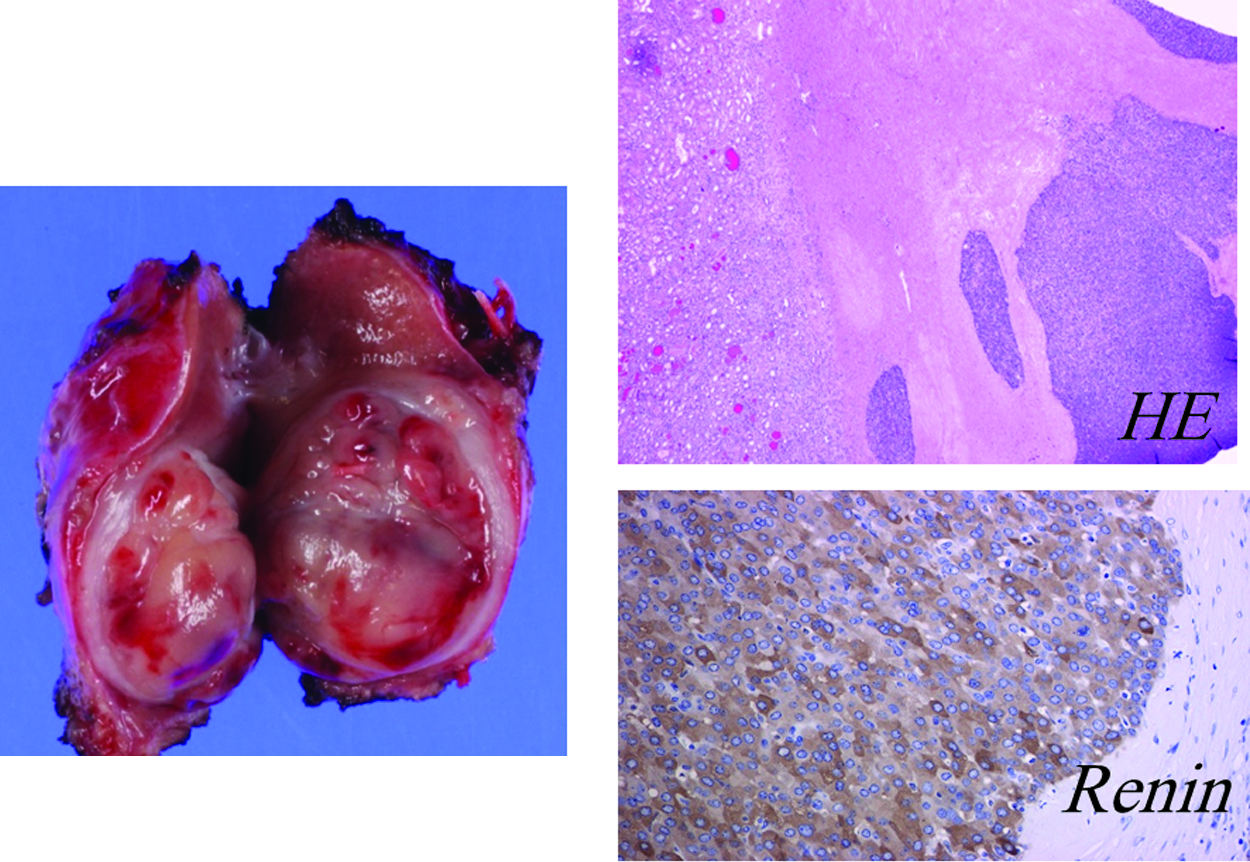
The tumor was well encapsulated and its cut surface was white (Lt). On histopathology, tumor cells were rich in cytoplasmic renin granules, typical of reninoma.
Postoperatively, plasma rennin and plasma aldosterone were 1.9 ng/mL/h and 18 pg/mL, respectively, on day 1. Blood pressure decreased to 90–110/70–80 by day 7. The patient was well enough to be discharged on day 4. At follow-up, kidney function was found to be well preserved bilaterally (Rt 51%, Lt 49%; split renal function) and her blood pressure and potassium levels have been normal for 12 months without any medication, and there is no evidence of recurrence or metastasis.
Discussion
Reninoma is a rare benign cause of hypertension in children. To date, ∼90 cases have been reported in the English literature.2,4,5 Reninoma patients are most likely to present with symptoms related to hypertension or may be asymptomatic and diagnosed incidentally. Typical biochemistry findings include hypokalemia, hyperaldosteronism, and the high rennin activity. In our case, proteinuria was detected during a routine school checkup, and on follow-up assessment, our case was found to be hypertensive. Accurate diagnosis can be difficult in children with mental retardation and proteinuria could easily have been disregarded. On CT or MRI, reninoma appears as a well-circumscribed isodense or hypodense mass without invasion of adjacent renal parenchyma 6 in contrast to renal cell carcinoma. However, a definitive diagnosis of reninoma is often difficult using imaging investigations alone as in our case where CT findings were actually typical of reninoma, but reninoma was not diagnosed. In our case, a 22 mm diameter mass was identified in the lower pole of the kidney; since the mass was located close to the renal hilum, it was overlooked initially leading to misdiagnosis. Doctors must be constantly aware that the cause of hypertension in children could be reninoma and be on the alert for any irregularity on renal US.
Reninoma is conventionally treated by surgical intervention to prevent possible long-term risks of cardiovascular and kidney diseases caused by hypertension. 7 Nephron-sparing surgery or partial nephrectomy is preferred for small tumors not associated with metastases. Laparoscopic partial nephrectomy is less invasive than open partial nephrectomy and usually performed transperitoneally. From experience, we prefer a retroperitoneal approach rather than a transperitoneal approach, because there is no need to mobilize the bowel and access to the kidney and renal hilum is more direct. 8 However, retroperitoneoscopy is extremely challenging; complicated by risk for tumor rupture and spread of malignant material, as well as being demanding technically, requiring expertise for en bloc hilar clamping, tumor excision, and renal reconstruction. Not to mention an adequate margin of the normal parenchyma must also be excised and the cut surface of the partial nephrectomy must also be sutured meticulously all during limited occlusion time.
In our retroperitoneoscopic partial nephrectomy, the same forceps, scissors, and retractors that are normally used in open surgery can be used under direct vision through the pararectal upper abdominal incision, making the operation far easier than if attempted using only laparoscopy or retroperitoneoscopy. 9 There are also none of the adverse hemodynamic or ventilator effects related to pneumoperitoneum, because surgery is performed without intraperitoneal carbon dioxide insufflation. In our case, there was no remarkable local bleeding, with only a total of 70 mL blood loss during tumor excision, which we attribute to adequate management of coagulation, nephron-sparing surgery, the location of the tumor near the renal hilum, and meticulous attention to technique. We believe our approach is superior to standard laparoscopic or retroperitoneoscopic nephrectomy and we invite surgeons to consider our approach as a valid alternative in selected patients.
Footnotes
Acknowledgment
The authors express their sincerest gratitude to Dr. Geoffrey J. Lane who made a significant contribution to this article as a native English speaker.
Disclosure Statement
No competing financial interests exist.