
Abstract
Abstract
Objective:
To demonstrate the feasibility of intraoperative nerve monitoring (IONM) in total endoscopic thyroidectomy (TET) for high-risk thyroid cancer and to confirm its additional benefit on reducing surgery duration and protecting the recurrent laryngeal nerve (RLN).
Subjects and Methods:
One hundred twenty-three patients with or without autoimmune thyroiditis (AT) underwent TET using IONM or not were included in the study. The primary outcome measures were the time used on related surgery procedures and the prevalence of RLN injury.
Results:
IONM could effectively reduce the time for locating the RLN (9.91 ± 1.68 minutes versus 12.49 ± 1.63 minutes; P < .01) and thyroid lobectomy (21.10 ± 4.53 minutes versus 27.35 ± 5.38 minutes; P < .01) but not central compartment dissection or whole surgery with or without AT. Of 167 at-risk nerves (98 in the IONM group and 69 in the non-IONM group), 5 (5.10%) in the IONM group (2 with and 3 without AT) suffered from temporary injury, compared with 7 (10.14%) in the non-IONM group (4 with and 3 without AT). Only 1 in the IONM group (with AT) and 2 in the non-IONM group (1 with and 1 without AT) developed permanent vocal cord paresis. The prevalence of RLN paresis was slightly decreased in the IONM group without statistical significance.
Conclusions:
IONM could reduce the time needed for RLN localization and thyroid lobectomy and make it easier for novices in TET. IONM also may decrease the incidence of the RLN paresis, especially temporary, compared with visualization alone; this proposal needs more evidence to confirm it in the future.
Introduction
D
Apart from hypoparathyroidism, injury to the RLN is the most common complication of thyroid surgery,6,7 which could cause dysphonia, swallowing difficulty, and respiratory problems as a result of vocal fold paresis. Despite developments in the technique of routine nerve identification and the surgical instruments, the RLN injury rate still remains high at 5%–6% and 1%–2% for temporary and permanent palsy, respectively.1,8–10 In TET, surgeons only have one hand to operate with and to expose the RLN, as the other hand has to tract the thyroid. So it is difficult to absolutely avoid RLN injury as a result of the little permissible operation error.
Intraoperative nerve monitoring (IONM) of the RLN has been used to help surgeons to trace the anatomical pathway of nerves and to prevent unexpected injuries over years. 6 Although it is a well-described technique by many studies consisting of large cohorts and/or meta-analyses during thyroidectomy by OTS, it still remains controversial whether IONM could effectively reduce the incidence of RLN injuries and predict postoperative RLN function. Dionigi et al. 11 recently found that the use of IONM in open thyroidectomy could reduce temporary RLN injury when compared with nerve visualization alone in a randomized trial. But, in a recent meta-analysis of available studies, no statistically significant difference of RLN injury rates was found by comparing IONM versus nerve visualization alone. 12
In the endoscopic thyroidectomy field, experiences with IONM have been rarely described. There have been only a few reports on the use of intraoperative nerve stimulation or IONM in the cervical endoscopic approach. Dionigi et al. 11 have showed that IONM is feasible and safe in endoscopic thyroidectomy. Lang and Wong 13 applied intraoperative nerve stimulation to predict vocal cord paresis; they found that a conventional bipolar nerve stimulator probe with no special instrument in transaxillary endoscopic thyroidectomy and robotic-assisted thyroidectomy is feasible, and indirect stimulation via the vagal nerve is more accurate in predicting the function of RLN. But, there is no article describing IONM in breast-approach TET, especially for thyroid cancer surgery. Because of the difficulty in identifying RLN in TET, IONM should be more helpful here than in OTS. In this study we present the application of IONM in TET for thyroid cancer and have investigated its feasibility and benefit for reducing the risk of RLN injury and operation time control.
Materials and Methods
Patients and study design
We performed a consecutive case series review of thyroid cancer patients who underwent TET with IONM (IONM group) or without IONM (non-IONM group) at the Second Affiliated Hospital of Zhejiang University (Hangzhou, China) from January 2012 to September 2014. In this period, 123 patients with thyroid cancer who underwent TET were included, of whom 55.3% (n = 68) had IONM. The inclusion criteria and patient selection for TET were as follows: (1) female, younger than 50 years, or if male one who cared about the scar in the neck; (2) the suspected nodule was smaller than 2 cm in diameter; (3) the whole weight of the thyroid estimated by presurgery ultrasound examination was smaller than 60 g; and (4) no suspected metastasis of lymph node in the lateral cervical region was found by ultrasound or computed tomography scan before surgery. The scope of surgery was determined by the lesion location and distribution. In brief, if the lesions were concentrated in one lobe, thyroid lobectomy with same-side central compartment dissection (CCD) was performed; if the lesions were distributed to two lobes, thyroidectomy and CCD for both sides were performed. In these cases both sides of RLNs were exposed to the danger of injury.
Informed consent on the surgery approach and the use of IONM was obtained from every patient before surgery. All the patients were followed up for more than 6 months.
A standardized form was designed to collect specific information about each patient (detailed procedures of surgery and IONM application, voice abnormality, and follow-up data). Standard information, including diagnosis, operating time, and the length of hospitalization period after surgery, was recorded in the hospital information system.
Preparation before surgery for IONM
For each patient who would undergo IONM in the surgery, a 6.0-mm (for women) or 7.0-mm (for men) endotracheal tube connected to a 3-cm length of exposed electrodes (Medtronic, Jacksonville, FL) was placed well in contact with the true vocal cords under direct laryngoscopy after general anesthesia before surgery. A NIM-Response 3.0 monitor (Medtronic) was used for nerve stimulation and monitoring throughout the entire procedure. Before surgery the related parameters of IONM equipment were rechecked. The impedance of the electrodes should be <5 kΩ, and the impedance imbalance should be <1.0 kΩ, so then the monitor would present a normal baseline with waveform amplitudes of approximately 10 μV.
Surgery procedure
The time spent on every procedure of surgery (including the time for building the working space, locating the RLN, the first lobectomy, the same-side CCD, and the entire surgery) was recorded and analyzed, and every time point was labeled as shown in Figure 1.
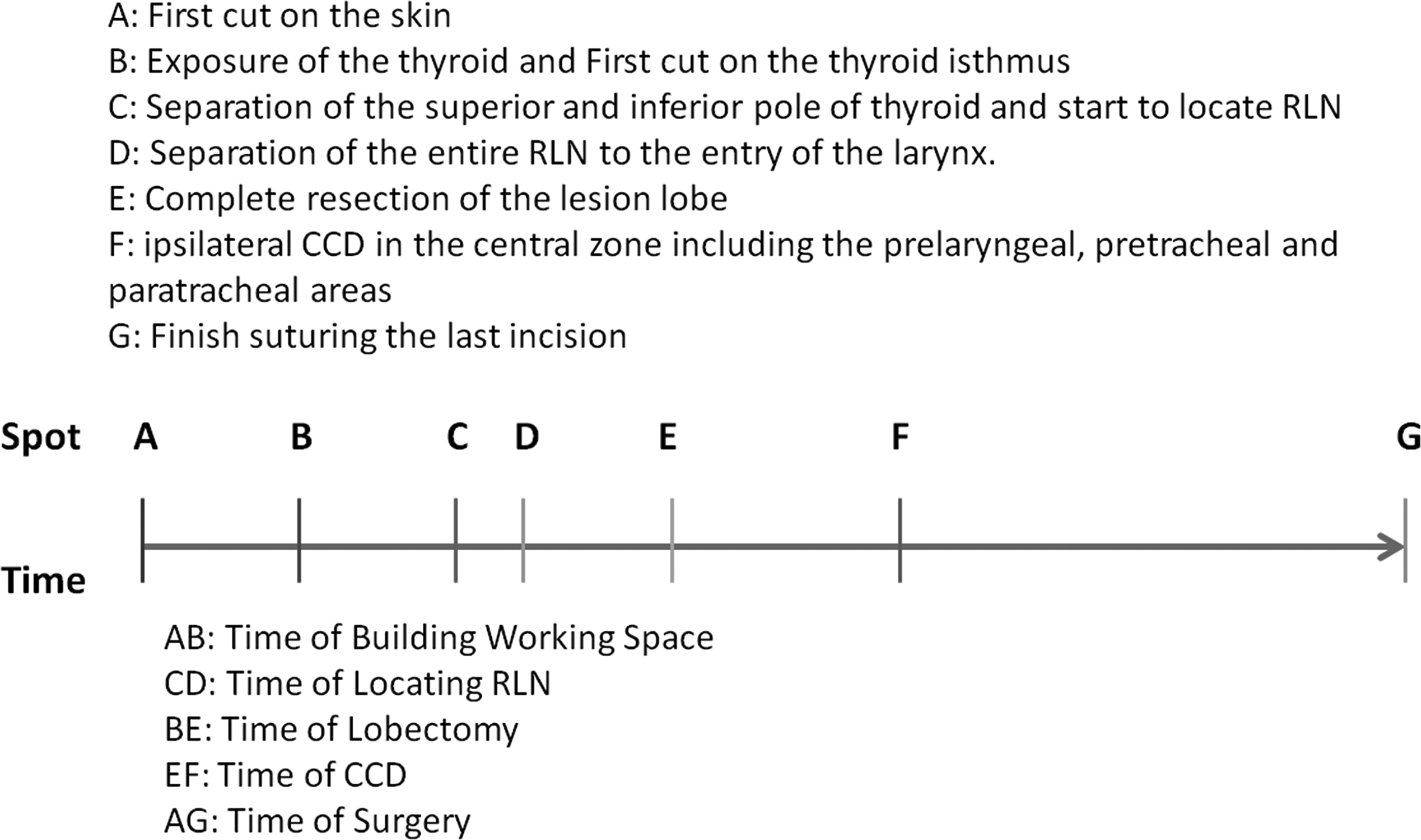
Time spent on every procedure, including building the working space, locating the recurrent laryngeal nerve (RLN), lobectomy, central compartment dissection (CCD) and the whole surgery was recorded according to these time-point marks.
The method of thyroidectomy and CCD was described previously. 11 In summary, a 10–12-mm incision was used for the observational video camera at the inner side of the right mammary areola, and two more 5–6-mm incisions were made at the upper margin of the bilateral mammary areolas for working instruments. The working space was built widely to the hyoid bone, as well as laterally to the medial edge of the sternocleidomastoid muscles on the normal side and to the lateral edge of the sternocleidomastoid muscles on the lesion side. For locating the RLN, after revealing the lobe by dissecting the isthmus and tracting over the ipsilateral strap muscle, the inferior and middle thyroid vessels were cut sequentially, and the lobe was pulled upward and to the middle. After that, the RLN was located in the tracheoesophageal groove with the help of IONM and exposed by blunt dissection with endoscopic forceps, or it was identified by the naked eye during the careful dissection. Subsequently the lobe was retracted downward, the superior vessels were cut by an ultrasound scalpel, and the lobe was resected completely. For total thyroidectomy, the contralateral lobe was resected in the same manner, and more attention should be paid to it if there is a signal loss of IONM in the former side.
CCD
Some patients had the malignancy confirmed by fine needle aspiration before surgery, and the rest were confirmed by intraoperative frozen section. Once the diagnosis of malignant thyroid papillary cancer was established, ipsilateral CCD was carried out in the central zone, including the prelaryngeal, pretracheal, and paratracheal areas. During the process, special attention was paid to protect the RLN from injury, and blunt dissection was always preferable around the RLN area. IONM was used to monitor the RLN at times or if needed to avoid unplanned damage.
Technique of IONM
Procedure of IONM for locating the RLN
After exposure and mobilization of the superior and inferior pole of the thyroid, the probe punctured the skin directly over the operation area in the neck and was placed on the nerve (Fig. 2A). The vagus nerve was routinely tested with a current of 3 mA to ensure the normal condition of the monitoring system on the outside of the carotid sheath in the middle neck. The evoked electromyographic signals were recorded as V1 signals (Fig. 2B). Then the lobe was pulled upward and to the middle, and the RLN was detected around the area beneath the inferior thyroid at the tracheoesophageal groove. Usually a current of 3 mA was used for stimulation, and it could be increased up to 5 mA if 3 mA failed to localize the RLN. The RLN can be located immediately and exposed easily on the spot with the strongest signal. The time needed for detecting RLNs and the success rates of early RLN localization and identification were recorded and analyzed. After localization and exposure, the electromyographic signals were obtained by direct RLN stimulation and were defined as R1 signals by a current of 1 mA (Fig. 2C), and then RLNs were dissected carefully to the entry of the larynx with blunt dissection. After the whole operation around the nerve, signals were obtained again by a current of 1 mA as R2 (Fig. 2D).
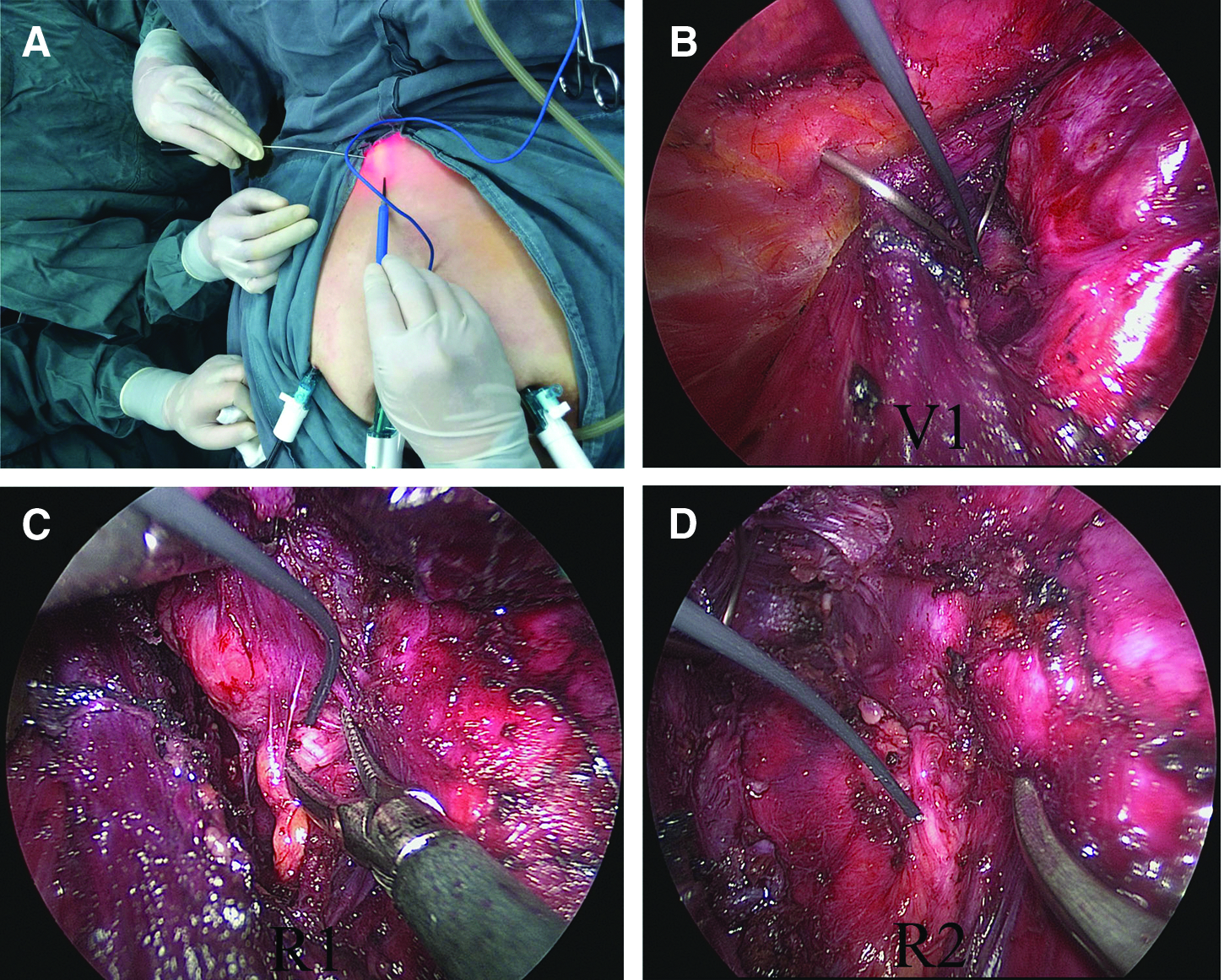
The position of the patient and the endoscopic view of the nerve stimulator are shown.
RLN monitoring during surgery
After separation of the entire RLN, IONM was used for detecting the signal of the RLN when necessary in the whole surgery process. If the signal decreased to less than 50% of R1, we believed the function of RLN had been damaged, and the surgery for another lobe should be paid more attention or sometimes might have to be delayed to some other day after confirmation of the function of RLN by flexible laryngoscopy when needed. The technique on the use of the nerve stimulator was previously described and standardized throughout the study period.5,14
RLN function assessment after thyroidectomy
Flexible laryngoscopy was used to examine the vocal cords 1–2 days before surgery for all cases. The voice complaints were recorded on postoperative Days 1–3, and direct laryngoscopy was applied within 2 weeks after thyroidectomy for the patients with voice complaints. Vocal cord paresis was defined as any hoarseness and combined by reduction in cord movement. Signal reduction of IONM was used to predict vocal cord paresis after thyroidectomy.
Statistical analysis
Mean ± standard deviation values were used to express the variables. Statistical analysis was performed by IBM-SPSS version 19.0 statistical analysis software (SPSS Inc., Chicago, IL). The significance of categorical variables was evaluated with the chi-squared test, and the unpaired Student's t test was used for continuous variables. Statistical significance was indicated by values of P < .05.
Results
The clinical characteristics between the IONM and non-IONM groups had no statistical differences.
In total, 123 TETs with or without IONM were included in this study from January 2012 to September 2014 (Table 1). The median age was 35.02 years old, and only 5 patients were male (2 in the IONM group and 3 in the non-IONM group). We compared the median age, gender distribution, surgical indications, scope of surgery, percentage of autoimmune thyroiditis (AT), and final pathology between the two groups. As shown in Table 1, the difference in median age and gender distribution had no statistical significance. For the indications of the surgery, 39.7% and 34.5% of patients in the two groups were diagnosed with thyroid carcinoma by fine needle aspiration before surgery. The rest were suspected as having malignancy by preoperative examination but were diagnosed after surgery. These data were in accordance with the final pathology. Most patients were papillary thyroid cancer, and only 1 was diagnosed as having follicular thyroid cancer after surgery. As 44 patients (30 in the IONM group and 14 in the non-IONM group) were suspected of having thyroid cancers in both lobes, whole thyroidectomy with CCD on both sides was carried out for these patients. In total, 167 RLNs were in danger in this study.
AT, autoimmune thyroiditis; CCD, central compartment dissection; RLN, recurrent laryngeal nerve.
IONM could effectively localize RLN with reduced time
All the 167 RLNs were finally separated successfully in the study. In the IONM group 98 RLNs were easily localized near the tracheoesophageal groove with the help of IONM, by a stimulation current of 3 mA or 5 mA. As shown in Table 2, the average time used to identify an RLN was statistically reduced in the IONM group (9.91 ± 1.68 minutes) compared with the non-IONM group (12.49 ± 1.63 minutes) (P < .01). AT could make the RLN identification more difficult and time consuming. But no matter whether AT was present or not, IONM effectively reduced the time compared with the non-IONM group (P < .01) (Table 2).
Time is given in minutes.
AT, autoimmune thyroiditis; CCD, central compartment dissection; IONM, intraoperative nerve monitoring; RLN, recurrent laryngeal nerve.
IONM could reduce the time for thyroid lobectomy
We recorded the time needed for all related surgery procedures, including RLN localization, thyroid lobectomy (the first side if total thyroidectomy was carried out), CCD, and the whole surgery. We found that lobectomy in the IONM group needed less time than in the non-IONM group whether with or without AT (P < .01). For patients with thyroid lobectomy and one-side CCD, the whole surgery time was also reduced: 94.23 ± 12.26 minutes in the IONM group versus 100.24 ± 11.7 minutes in the non-IONM group. However, we also showed that IONM has no effect on reducing the time for total thyroidectomy and for CCD, whether with or without AT.
Comparison of vocal cord palsy rate between the two groups
As mentioned above, there were in total 98 RLNs in the IONM group and 69 RLNs in the non-IONM group at risk. Five of the 98 RLNs (5.15%) in the IONM group (2 with AT and 3 without AT) suffered from temporary damage, compared with 7 of the 69 RLNs (10.14%) in the non-IONM group (4 with AT and 3 without AT). Regarding permanent vocal cord palsy, there were only 1 case in the IONM group with AT and 2 in the non-IONM group including 1 with AT and 1 without AT. All the differences were not statistically significant by the chi-squared test (Table 3).
Data are number (%).
AT, autoimmune thyroiditis.
Depending on the IONM monitor, all the 5 cases of temporary vocal cord palsies lost more than 50% of the stimulation nerve signal, and they recovered without any treatment in 2–3 months. However, the permanent case had no signal at the end of surgery, and palsy remained after 6 months. All the other 92 RLNs that lost signals less than 50% at the end of surgery had no vocal cord palsy.
Discussion
TET has been welcomed by young female patients with thyroid cancer because of its perfect cosmetic result and reliable treatment effects. Our department has carried out more than 1800 cases of TET, including thyroid cancer and benign tumor, since 2006. In TET, surgeons have to use one hand to pull the thyroid and thus do the dissection with only one hand in a limited working space without assistance. So even for experienced surgeons the process of locating and dissecting an RLN is more risky and difficult than in OTS. IONM act as an important adjunct technology to insure thyroid surgery safety and quality. 15
Although there are still some reports in which its role is suspected in reducing the incidence of RLN injury, in a randomized clinical trial with 1000 nerves in danger, Barczynski et al. 6 concluded that IONM may be of additional benefit in decreasing the incidence of transient but not permanent RLN paresis, especially in high-risk patients, when compared with nerve visualization alone. IONM may eventually become a surgical routine in thyroid disease, especially in thyroid cancer patients who need whole RLN exposure and the soft tissue around dissection. The application of IONM in OTS has been well documented, but the report of its use in endoscopic thyroidectomy, especially TET, remains scarce. Dionigi et al. 11 have successfully used IONM in video-assistant thyroidectomy. Lang and Wong 13 have reported the first research of technological feasibility on the use of IONM in gasless, transaxillary endoscopic thyroidectomy and robotic-assisted thyroidectomy.
We believe the current report is the first one on the applications of IONM in TET through the breast approach. We aimed to reveal the feasibility of IONM in TET and at the same time provide benefits for patients in reducing the surgery time and decrease the RLN injury probability. We retrospectively followed up 123 patients with thyroid cancer who underwent TET with (n = 68) or without (n = 55) IONM and compared the time spent on every related surgery procedure and the incidence of RLN paresis.
In this article we demonstrated that the application of IONM in TET surgery for thyroid cancer patients was feasible and reliable. There are several points for attention in the use of IONM. As mentioned previously, 11 there is a long distance between the skin incision in the chest to the surgery area. All the commercial available nerve stimulator probers were designed for open surgery and appear to be not long enough for TET. So we have to puncture the skin directly over the monitoring area in the neck with the probe (as shown in Fig. 2A). Every time when we changed the monitoring position, repeated puncture may cause a certain degree of skin damage. A specially designed long endoscopic probe is needed for the promotion of IONM in TET through the chest approach. Even with a long probe, frequent replacement between the probe and the operation forceps may be a waste of time and an impediment for real-time monitoring.
A special operation forceps directly connected to the nerve monitoring system with a special cable would be an ideal option. We have designed a multifunction forceps that has the function of separation, monitoring, and traction at the same time (data not shown). It is predicted to be commercially available soon.
During the IONM process, muscle-relaxant drugs were forbidden so it became more difficult to perform retraction during surgery, which caused poor exposure and more difficult surgery, especially in TET. As male patients usually have more developed muscles, we believe that the use of IONM for male patients, especially for strong ones, should be more carefully evaluated before surgery.
After confirming the feasibility of IONM in TET, we then evaluated whether IONM was helpful in reducing the time for thyroid surgery and therefore alleviating the potential injury caused by anesthesia. We divided the whole operation into several parts according to special events as time points (Fig. 1) and recorded the time used for the five representative procedures: building the working space, locating the RLN, the first-side thyroid lobectomy, same-side CCD, and the whole surgery. In order to reduce the errors induced by individual differences, for patients who need total thyroidectomy and both-side CCD, we only analyzed the surgery for the first side. As well, we exclude patients with tumors larger than 3 cm or with a huge thyroid volume. Thyroids with AT usually are hard tissues, and it could make the surgery more difficult. We also divided each group into two subgroups—with or without AT—and analyzed the time needed for every procedure and incidence of RLN injury correspondingly. As shown in Results, we found that IONM could effectively reduce the time needed for locating the RLN and then for thyroid lobectomy. For the time spent on building the working space, CCD, and the whole surgery, IONM has no dramatic influence. We thought it might be caused by the limited sample in this study, which should be improved in the future.
The major benefit of IONM is the assistance in nerve identification and protection, resulting in a decrease in the prevalence of RLN paresis (temporary and permanent). Previous studies on OTS applying IONM have confirmed that IONM could decrease the incidence of transient RLN paresis compared with visualization alone, especially in high-risk thyroid cancer patients who needed CCD.6,16 Although most of the studies found different degrees of decrease in prevalence of permanent RLN paresis with IONM, inadequate power to reliably indicate advances of IONM was found in all the studies.6,16 The same drawback existed in the present study. We found the decrease in permanent and temporary RLN paresis in both AT and non-AT groups with IONM. However, no significant difference was confirmed because of the inadequate sample. So a random control trial with a larger sample number may be needed to confirm its effect in TET in the future.
As an added bonus, the use of IONM makes more thorough our understanding of the intraoperative injury and protection of RLN. Visualization alone only can be used to estimate the integrity of anatomical structure of the RLN and is useless in predicting the function of the RLN after surgery. Especially in TET, visualization was carried out through the video displayed on the screen rather than as seen by the naked eye. So at the beginning of the IONM application, we found that 5%–10% of cases showed signal attenuation by more than 50%, although the anatomical integrity was kept well. This may be caused by (1) tractive injury—when separating the RLN near the throat, it is easy to cause nerve tractive injury by stretching the surrounding tissue, especially in patients with AT—or (2) thermal burn—overheating energy devices such as cavitron ultrasonic surgical aspirator were lethal for an RLN and could cause irreversible damage sometimes. It is helpful to place medical gauze near the nerve or to clean the device frequently with cold water. So we believe that IONM could help the surgeons to review their own operating errors and to improve surgical skill, thus avoiding accidental injuries as we mentioned above and decreasing the RLN palsy at the extreme. It may be especially useful for TET novices to improve surgical skills and shorten the learning curve period.
Footnotes
Acknowledgments
This work was supported by The Scientific Foundation of Zhejiang Province (grant LY14H160033).
Disclosure Statement
No competing financial interests exist.