
Abstract
Abstract
Introduction:
Surgically altered anatomy complicates endoscopic procedures of the pancreaticobiliary tree. Biliary strictures have been managed using percutaneous transhepatic techniques.
Materials and Methods:
In recent years device-assisted enteroscopy (e.g., double balloon enteroscope [DBE]) has been used to gain access to the common bile duct. The length of the scope and its narrow, 2.8-mm working channel limit the use of standard endoscopic retrograde cholangiopancreatography (ERCP) devices. Therefore, shorter enteroscopes for ERCP have been developed. A fully covered self-expandable metallic stent (fcSEMS) cannot be used through the narrow channel. In conventional anatomy, benign biliary strictures have been treated using fcSEMS, requiring fewer endoscopies compared with multiple plastic stenting.
Results:
Here we report the first case of fcSEMS deployment through the working channel of a novel, long DBE with a 3.2-mm working channel, and 2 cases with the conventional narrow-channel DBE, using the rendezvous technique, with fcSEMS insertion on a wire running along the enteroscope.
Conclusions:
These new techniques, here used on benign biliary strictures, are described in detail.
Introduction
S
In conventional anatomy, cases of benign biliary stricture have successfully been treated endoscopically by placing a multiple plastic stent or a fully covered self-expandable metallic stent (fcSEMS). Using fcSEMS limits the number of procedures needed. 4 In altered anatomy, repeated dilations through the PTC drain are usually needed, adding to patient discomfort. For DBE-assisted ERCP an fcSEMS has not previously been available.
We present 3 patient cases with surgically altered anatomy for whom fcSEMS devices were used. Two were performed with a standard DBE and the rendezvous technique deploying the stent over a wire running along the DBE. In the third case, a custom-made fcSEMS was deployed using a novel, commercially available 200-cm DBE with a 3.2-mm working channel.
Patients and Methods
In Cases 1 and 2, a Fujifilm DBE (model EN-450T) with a 200-cm working length and a 2.8-mm working channel (Fujifilm Corp., Tokyo, Japan) was used, whereas in Case 3, a Fujifilm double balloon endoscope (model EN-580T) with a 200-cm working length and a 3.2-mm working channel (Fujifilm Corp.) was used. In all cases, there was a 145-cm-long and 13.2-mm-wide TS-13140 overtube with a transparent hood attached to the tip of the scope. All procedures were performed using CO2 insufflation, with the patient in prone position, under conscious sedation controlled by an anesthesiologist and a nurse. The wires, catheters, and stents used are presented separately in each case.
Case 1
A 73-year-old male, with a Billroth II type gastric reconstruction, developed cholecystitis with a subphrenic abscess in January 2014. The abscess was drained, and the patient was treated with antibiotics. Due to a suspected bilioenteric fistula, a DBE ERCP was performed. The papilla was reached. There was air in the biliary tree on fluoroscopy. Despite several attempts being made, the common bile duct (CBD) could not be cannulated. As cholecystitis was established and a bilioenteric fistula was suspected, an open cholecystectomy was performed in May 2014. A T-tube was inserted into the CBD. One week later, a distal stricture of the CBD was identified on cholangiography.
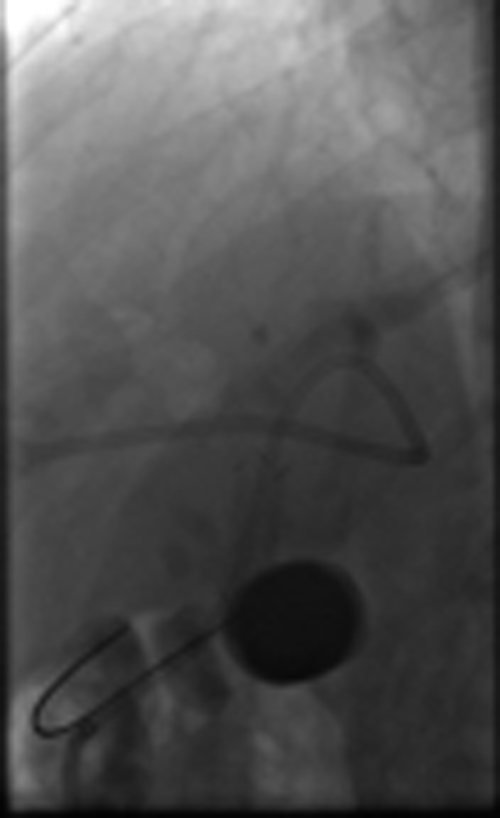
A DBE ERCP was performed in June 2014 with the intention to stent the CBD stricture. The DBE was introduced to the papillary site. A guidewire (HydroSteer™; St. Jude Medical, Minnetonka, MN) was inserted through the T-tube into the duodenum. Using a balloon catheter (triple-lumen extraction balloon; Endo-Flex GmbH, Voerde, Germany) on the guidewire, a Jagwire™ (Boston Scientific, Alajuela, Costa Rica) was inserted through the T-tube into the duodenum and again out of the mouth using a snare through the enteroscope. An fcSEMS (4 cm long, 10 mm in diameter; Niti-S™ biliary covered stent [Kaffes™; TaeWoong Medical Co., Ltd., Gyeonggi-do, South Korea]; 9 French, 180-cm introducer) was deployed into the CBD through the mouth, over the Jagwire running along the enteroscope, under fluoroscopic and endoscopic control (Fig. 1). The T-tube was removed. A DBE ERCP for stent removal was planned at 6 months from the procedure.

Fluoroscopic view of the deployed fully covered self-expandable metallic stent in Case 1.
Case 2
A 57-year-old female with primary sclerosing cholangitis had had a liver transplantation with an HJ in 1998. The patient also suffered from Crohn's disease. In the summer of 2013, the patient started having episodes of recurrent cholangitis, which were treated with antibiotics. Contrast-enhanced magnetic resonance imaging in October 2013 showed a short stricture of the HJ and slightly dilated intrahepatic bile ducts in segments II and III of the liver. As the changes were considered as minor, a prophylactic antibiotic was started. Six months later, the magnetic resonance imaging showed similar changes. The biopsy showed mild cholangitis and Stage I fibrosis around one bile duct, raising the suspicion of relapsed primary sclerosing cholangitis.
A PTC was performed in March 2014. A segmental duct was dilated with a 3-mm balloon, and the HJ was dilated with a 5-mm balloon. An 8 French internal–external drain was inserted. The drain did not work sufficiently, and, even though it was changed twice, first to a 10 French drain and then to a 12 French drain, there were problems with cholangitis and bile leakage at the root of the drain.
A rendezvous procedure using a DBE was performed in June 2014. The afferent jejunal limb could be reached only distally; thereafter the DBE was looped and did not proceed. A guidewire (Radifocus® nonvascular angled guidewire, 0.035 inch in diameter, 450 cm long; Terumo Europe NV, Leuven, Belgium) was inserted through the PTC drain, reaching the enteroanastomosis. The guidewire was exchanged for a longer Jagwire (Boston Scientific). Another Jagwire was inserted with the help of a cut Ramp catheter (Haber Ramp catheter; Cook Medical, Limerick, Ireland). Both wires were taken out through the mouth with the enteroscope. Using one wire, the enteroscope was drawn to the site of the HJ anastomosis. Using the second Jagwire, a 3-cm-long fcSEMS (Niti-S biliary covered stent [Kaffes]; 9 French, 180-cm introducer) was inserted and released under fluoroscopic (Fig. 2) and endoscopic (Fig. 3) control. The endoscopic view showed the stent snare to reach the bowel.
Fluoroscopic view of the deployed fully covered self-expandable metallic stent in Case 2.
Endoscopic view of the wired hepaticojejunostomy in Case 2.
As DBE would be unlikely to be managed without a guidewire, a clamped PTC drain was entered inside the stent to ensure later access. The intended stenting time was 1 year, but a check-up DBE ERCP was set up 3 months later.
At this check-up, it was noted that the fcSEMS had migrated into the bile duct above the anastomosis. The anastomosis was well checked with a 13-mm balloon (triple-lumen extraction balloon, 250 cm long; Endo-Flex GmbH), and it passed without difficulty. The stent was removed. As the HJ was well open, the stent was not replaced. The PTC drain was also removed.
Case 3
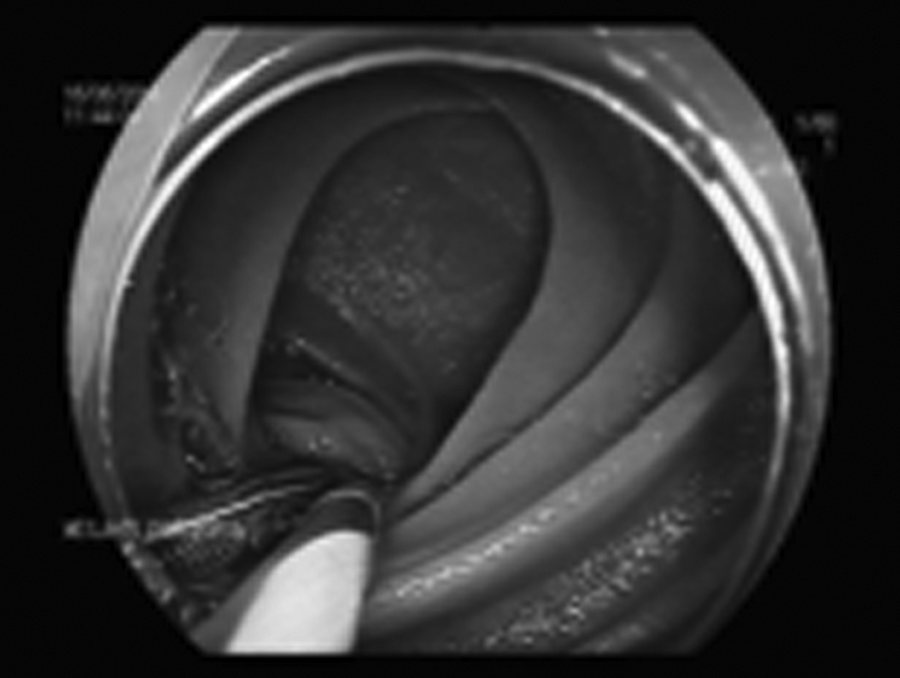
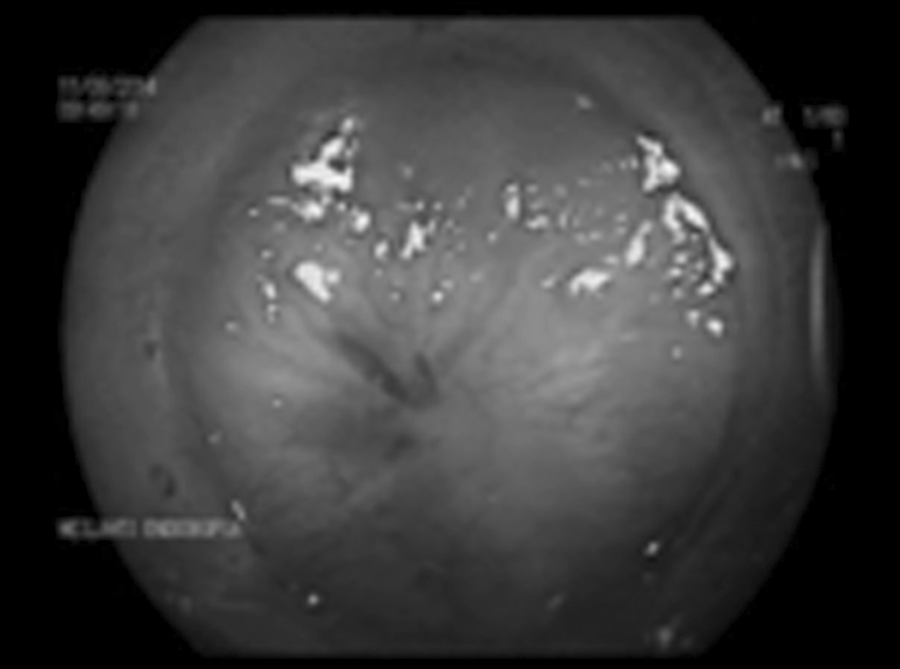
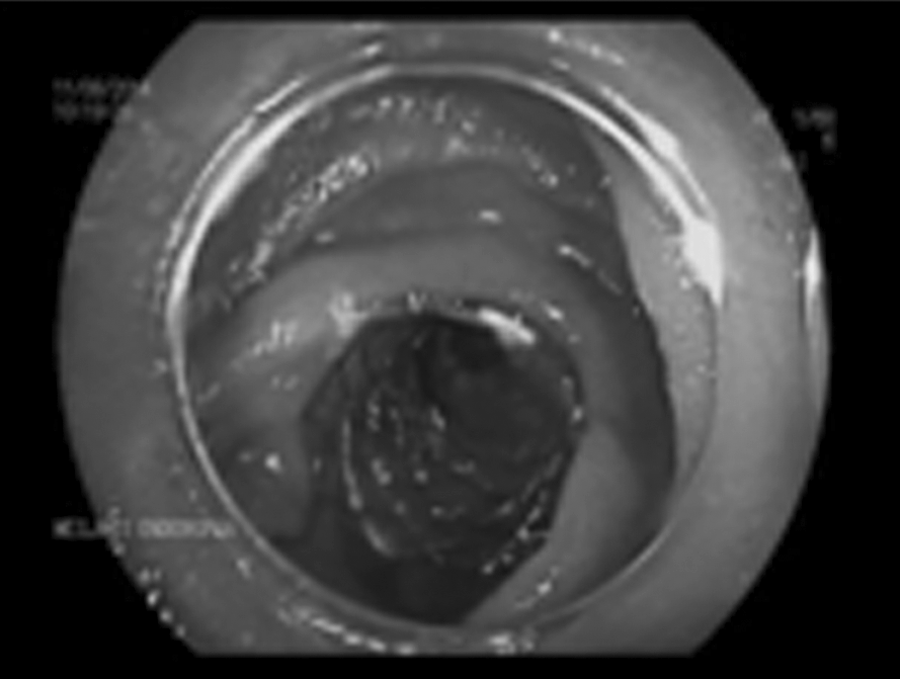
A 72-year-old female had had a pancreaticoduodenectomy due to a T2N1 neuroendocrine tumor of the head of the pancreas in August 2013. One year later, the patient suffered from relapsing episodes of cholangitis. There was suspicion of a stricture of the HJ anastomosis. A DBE ERCP was performed in August 2014. The HJ site was reached, and the anastomosis was found to be very tight (Fig. 4); it was hardly possible to pass with a guidewire (FTE-Wildcat; 0.035 inch in diameter, 650 cm long; pk endoskopie GmbH, Hannover, Germany) (Fig. 5). A precut using a needle knife (FTE-B2-papillotome; 250 cm long, 2.3/1.8 mm in diameter; pk endoskopie GmbH, Hannover, Germany) was performed. The anastomosis was dilated with a 10-mm dilation balloon (CRE™ wireguided dilatation catheter; 290 cm long; Boston Scientific, Natick, MA), and then a custom-made 2-cm-long Hanaro fcSEMS, expanding to 10 mm (Hanarostent™ fully covered biliary flap; 9 French, 230 cm long delivery device; M.I. Tech Co. Ltd., Gyeonggi-do, South Korea) with antimigration flaps, was deployed using the DBE working channel (Figs. 6 and 7).
The tight hepaticojejunostomy in Case 3.
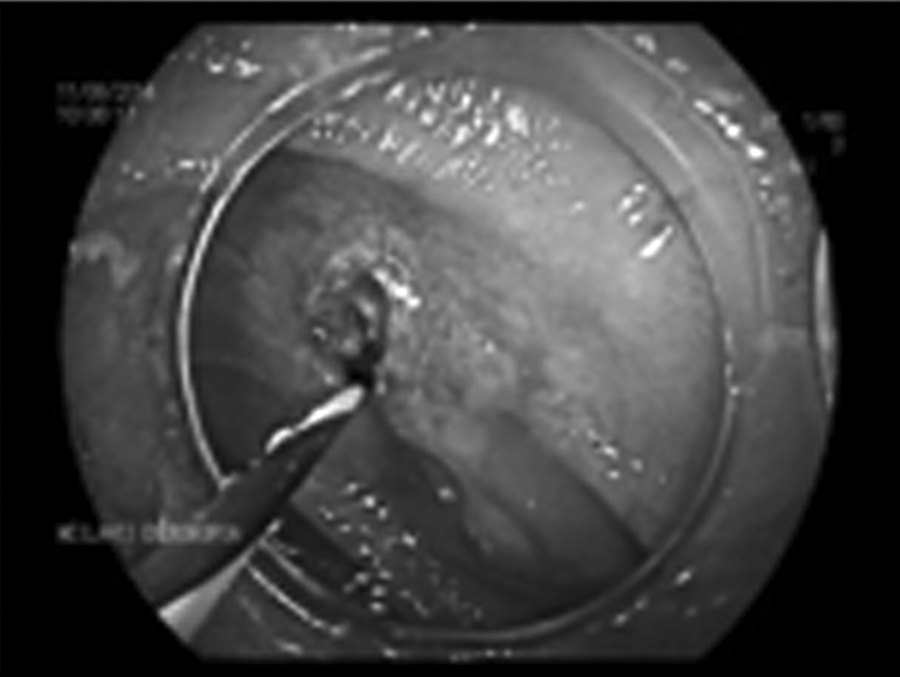
Guidewired tight hepaticojejunostomy in Case 3.
Endoscopic view of the deployed fully covered self-expandable metallic stent in Case 3.

Fluoroscopic view of fully covered self-expandable metallic stent deployment in Case 3.
A follow-up with a plain abdominal X-ray is planned at 6 and 12 months from the procedure to evaluate whether the stent has migrated or not. If the stent still remains in place at 1 year, it will be removed with a DBE ERCP.
Discussion
Until now, using long enteroscopes, through-the-scope placement of covered self-expandable metallic stents has not been feasible due to the limited diameter of the working channel and the inappropriate length of the stent deployment catheter. A thin working channel (2.8 mm) limits the use of accessories available. The narrow channel also causes stress for the endoscopist while the pushing-in and pulling-out action of the devices is very tight.
Rendezvous fcSEMS
In our 2 cases, the patients had transcutaneous routes when admitted for DBE. Naturally, when this route exists, this advantage should be used to perform a rendezvous procedure. In fact, the HJ site would not have been reached in Case 2 without the existing PTC route. Standard fcSEMS and delivery device can be inserted with the use of the transhepatic wire running along the endoscope. The advantage of using the rendezvous technique instead of a pure PTC technique is having the endoscopic view in addition to the fluoroscopic view.
Custom-made fcSEMS
Here we report the first case of fcSEMS deployment through the working channel of a long DBE. The stent was custom-made with a delivery device longer than those for a standard fcSEMS. The DBE used has a 3.2-mm working channel, which is wider than that of other commercially available balloon enteroscopes. The properties of both the endoscopes and accessories are evolving, improving the possibilities for endoscopic treatment of the pancreaticobiliary tract in patients with altered anatomy. A short prototype short balloon enteroscope with a 3.2-mm working channel 5 enables the use of standard ERCP equipment including standard self-expandable metallic stents. Still, gaining access to the blind end may be challenging using a short scope.
Future aspects
Even though there are crucial refinements regarding the endoscopes and the accessories for ERCP in altered anatomy, there are still obstacles compared with standard ERCP. The most notable differences are the lack of an elevator and the front- (instead of side-) viewing endoscope. The use of a side-viewing endoscope may be unfeasible, as advancement in the small bowel and through the afferent limb requires a front-viewing scope.
The number of bariatric patients is increasing quickly. Obesity surgery leads to rapid weight loss, which stimulates the formation of gallstones. A long enteroscope enables a high success rate in reaching the afferent loop also after Roux-en-Y gastric bypass with a long anatomic route from the mouth to the papilla. There is an urgent need to improve the accessories that can be used with long enteroscopes to overcome difficulties in these laborious procedures.
Treatment of a benign biliary stricture in altered anatomy is complex. Performing ERCP in these patients is laborious and time consuming. The new fcSEMS, which can be passed through the working channel of long enteroscopes, is a welcome accessory in limiting the need for repeated procedures. However, in cases of failed cannulation, PTC with planned rendezvouz-assisted stenting using fcSEMS is a good alternative.
Footnotes
Disclosure Statement
No competing financial interests exist.