
Abstract
Abstract
Background:
Obesity is a common disease affecting young adults and adolescents worldwide. This study aims to delineate the role of laparoscopic sleeve gastrectomy (LSG) in weight loss and associated comorbidities to adolescents and young adults.
Patients and Methods:
This study is a retrospective analysis of a prospective cohort of all young adults 16–22 years old who underwent LSG for morbid obesity and were followed up for 24 months. Demographic data, weight loss, and the status of several comorbidities, such as diabetes mellitus, hypertension, and dyslipidemia, were assessed at postoperative Months 1, 3, 6, 12, 18, and 24.
Results:
Overall, at baseline and after 24 months of close follow-up of 37 adolescents and young adults who had undergone LSG, the body mass index of the patients was 46.93 ± 6.07 kg/m2 versus 26.2 ± 3.6 kg/m2 (P < .001), and the body weight was 143 ± 29 kg versus 78 ± 15 kg (P < .001). From the first follow-up visit after operation to the last one at the 24 months, there was also a significant difference in percentage excess weight loss (22.40 ± 6.58% versus 81 ± 17%; P < .001), body mass index difference (−5.47 ± 1.69 kg/m2 versus −18.08 ± 4.38 kg/m2; P < .001), and percentage excess body mass index loss (26.06 ± 7.56% versus 96 ± 21%; P < .001). The percentage of the adolescents and young adults with diabetes mellitus, hypertension, and dyslipidemia were diminished gradually at 6 months postoperatively (P < .001).
Conclusions:
LSG represents a safe and attractive treatment strategy for morbidly obese adolescents and young adults with comorbidities. In this study group excellent resolution of excess weight and comorbid conditions is achieved 2 years after LSG.
Introduction
O
This phenomenon is much more disconcerting because the increased prevalence of obesity is accompanied by an increased frequency of obesity-associated comorbidities among children and adolescents, such as hypertension, diabetes mellitus type 2, and dyslipidemia. Now a clinician is facing these comorbidities in young adults, even adolescents and children, and most nonsurgical therapies for obesity are proving ineffective.3–6
Bariatric surgery is currently the most effective evidence-based method to obtain long-term weight loss in severely obese patients. The safety, efficacy, and substantial outcome of bariatric surgery are not well documented in adolescents and young adults. There are currently few reports in the medical literature regarding this population, and most of them are retrospective small single-institution studies.3,6–11 Most of these studies are showing a substantial weight loss of the pediatric and adolescent population. These results are comparable with the outcomes of the bariatric procedures in the adult obese population. It seems also that cost-effectiveness of adolescent bariatric surgery is recognized, when evaluated over a long period of time. 12
This study presents the experience of a single institution treating obese adolescents and young adults. Preoperative and 24 months of follow-up postoperative prospectively collected data results are presented regarding weight loss, dyslipidemia, hypertension, and type 2 diabetes mellitus in obese adolescents and young adults who underwent laparoscopic sleeve gastrectomy (LSG).
Patients and Methods
This study is a retrospective analysis of a prospective cohort of consecutive patients who underwent LSG for morbid obesity. All of the patients underwent LSG in a single institution from the same experienced minimally invasive surgical team. The patients were evaluated and followed up for up to 24 months. This study was approved by the Ethical Committee of the local institution.
Informed consent was obtained from all individual participants included in the study, and procedures followed were in accordance with the ethical standards of the responsible governmental committee on human experimentation.
Operative technique
The patient was placed in the supine position, with the legs apart, in a slight reverse Trendelenburg position. The pneumoperitoneum was established with the open technique, and four trocars were placed. The greater omentum was freed from the greater curvature of the stomach from a point 3–4 cm above the pylorus through the angle of His. This maneuver was accomplished with the aid of a laparoscopic shear using ultrasonic vibration. A bougie was placed to guide the gastric section (34 French). The vertical sectioning of the stomach was performed with two firings of the laparoscopic linear stapler with green cartridge loads and subsequently firings with blue cartridges. All the firings were performed in close proximity with the bougie. After the operation, nasogastric tubes were placed, and methylene blue was instilled to ascertain the integrity of the stomach.
This prospective cohort study enrolled consecutive overweight adolescents and young adults (16–22 years old) who fulfilled the criteria for bariatric operation. Prior to the operation, the morbidly obese young adults were questioned regarding their previous medical histories, comorbidities, and medications. Baseline demographic and anthropometric characteristics were collected at each visit.
Blood tests were performed to evaluate patient lipidemic profile and glucose levels. The fasting glucose, total cholesterol, and low-density lipoprotein cholesterol levels were measured. Moreover, glucose tolerance tests were performed in all patients. The blood pressure in all patients was also measured.
In cases of elevated levels of blood lipids, glucose, or blood pressure without previous history or medication, an expert consultation was performed. Subjects were followed up for 2 years at regular intervals (1, 3, 6, 12, 18, and 24 months) after the LSG. In these time periods, the medical team assessed body mass index (BMI) and calculated the BMI difference, the percentage of excess weight loss (%EWL), and the percentage of excess BMI loss (%EBMIL).
The %EWL was calculated as ([preoperative body weight – current body weight]/[preoperative body weight – ideal body weight]), where the ideal weight was estimated based on the Devine formula. The BMI difference was calculated as (current BMI – preoperative BMI). The %EBMIL was calculated as ([preoperative BMI – current BMI]/[preoperative BMI – 25]).
Arterial hypertension was defined by blood pressure exceeding 140 mm Hg. Diabetes mellitus was defined by abnormal glucose tolerance tests and elevated fasting glucose levels (>110 mg/dL). Dyslipidemia was defined by total cholesterol levels above 200 mg/dL and/or low-density lipoprotein cholesterol levels above 190 mg/dL.
During follow-up, possible alterations of blood pressure, diabetes mellitus, and dyslipidemia were assessed. The remission of these comorbidities was accepted when the patients' values returned to within the normal levels without medication (blood pressure, <140 mm Hg; total cholesterol, <200 mg/dL; low-density lipoprotein cholesterol, <190 mg/dL; fasting glucose, <110 mg/dL).
Statistical analysis
All variables were tested for normal distribution of the data. Continuous variables with normal distribution are presented as mean ± standard deviation values. Categorical variables are presented as valid percentages. The paired-sample t test was used to test for differences in mean values of continuous variables at the different examined days. Friedman's test was used to test for changes in continuous variables over time. Changes in the frequencies of arterial hypertension, diabetes mellitus, and dyslipidemia before and at the end of the follow-up period were tested with z-scores. All reported P values were based on two-sided tests. All statistical calculations were performed using SPSS software (version 18.0; SPSS Inc., Chicago, IL).
Results
Overall, 37 adolescents and young adults underwent LSG for morbid obesity in our institution from October 2009 to December 2012. Over half (62.1%) of the patients were female, and the rest (37.8%) were male. The mean age was 19 years (range, 16–22 years), and the mean BMI at presentation was 46.9 kg/m2 (range, 40.8–52.9 kg/m2). Subjects were followed up for a mean time of 23 ± 2 months. At presentation, of the 37 adolescents and young adults, 2 patients had arterial hypertension, 2 patients had diabetes mellitus, and 4 patients had dyslipidemia. All of these patients received medication for these comorbidities before operation. The baseline characteristics of the participants are shown in Table 1.
BMI, body mass index; SD, standard deviation.
BMI, BMI difference, %EWL, and %EBMIL over the 24-month follow-up are presented in Table 2. In Table 2 the comorbidities of the adolescents and young adults preoperatively and during follow-up are also given. Specifically, at the end of the follow-up period compared with baseline, there was a significant decrease in body weight (78 ± 15 kg versus 143 ± 29 kg; P < .001) and in BMI (26.2 ± 3.6 kg/m2 versus 46.93 ± 6.07 kg/m2; P < .001). From the first follow-up visit after operation to the last one at the 24 months, there was also an increase in %EWL (22.40 ± 6.58% versus 81 ± 17%; P < .001) and in %EBMIL (26.06 ± 7.56% versus 96 ± 21%; P < .001) and a significant decrease in BMI difference (−5.47 ± 1.69 kg/m2 versus −18.08 ± 4.38 kg/m2; P < .001) (Fig. 1).
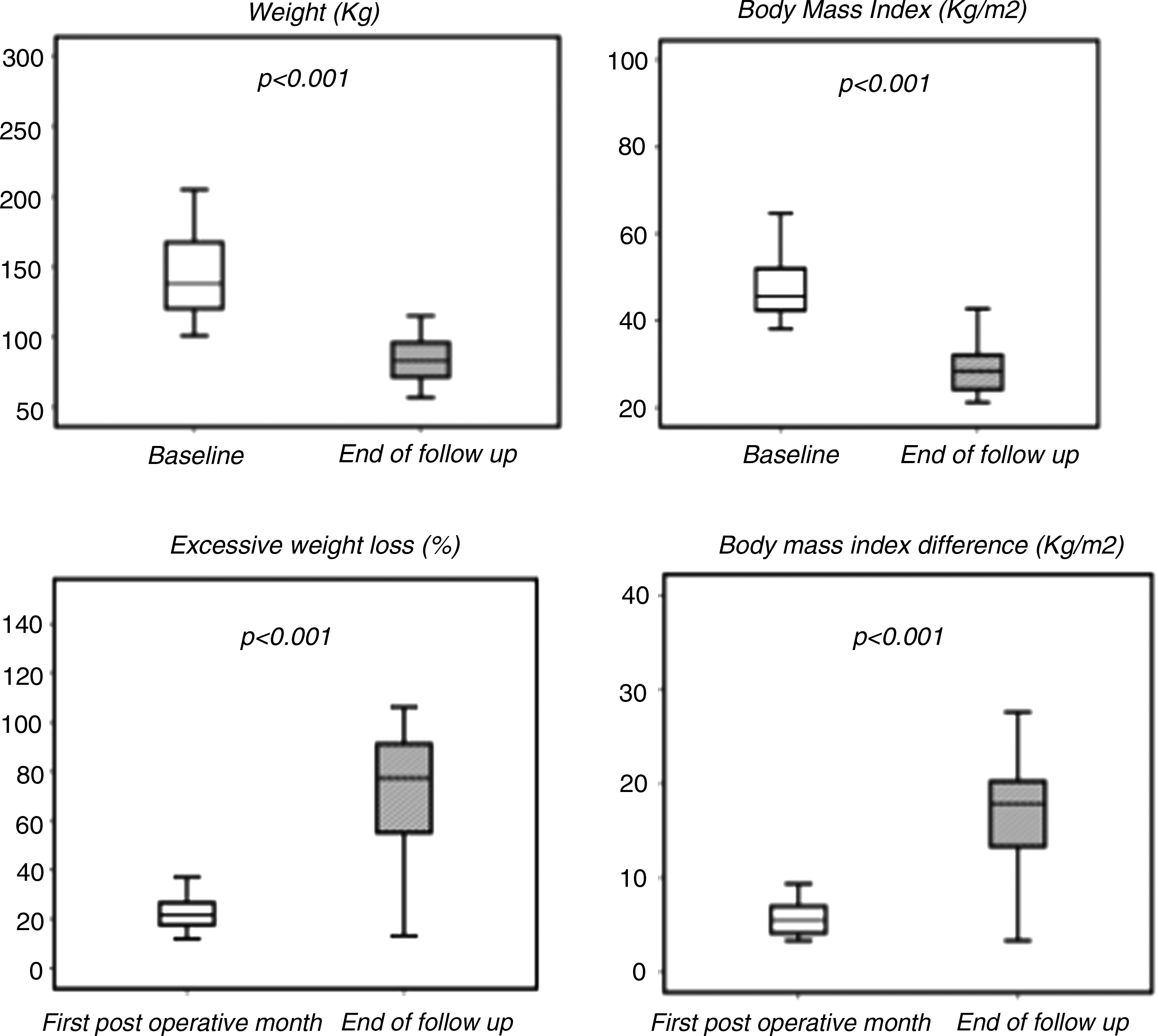
Stock charts with
Data are mean ± standard deviation values or number as indicated.
P values are based on Friedman's analysis of variance test.
%EBMIL, percentage excess body mass index loss; %EWL, percentage excess weight loss; BMI, body mass index.
Moreover, at Month 6 of the follow-up there was a significant decrease in the frequency of dyslipidemia compared with baseline (10.8% versus 0%; P < .05). All of the adolescents and young adults with hypertension before LSG (n = 2) normalized blood pressure during the first 3 months of follow-up (5.4% versus 0%; P < .05). The same phenomenon was observed also for the patients with diabetes mellitus in 3 months (5.4% versus 0%; P < .05). All of the adolescents and young adults discontinued their medication during the postoperative period.
Discussion
Obesity in adolescents and young adults is a worldwide scourge. A stepwise increase of childhood and adolescent obesity has been documented in the last 2 decades, and there is no trend declining. It is estimated that prevalence of obesity in adolescents is reaching as high as 16.5% in the United States, 18.3% in the United Kingdom, and 35.8% in Latin America. In China, in certain urban regions the prevalence of obesity in young children and adolescents is rising also very rapidly. The most concerning is that this trend is also followed by an increase of obesity-related comorbidities.1–4,6
In the past criticism about introducing bariatric surgery in adolescents and young adults population has been intense. Families of obese adolescents also have many concerns regarding performing operations that may have irreversible results, lasting their entire life, and regarding chances of major morbidity and death. Compliance of adolescents and young adults is also very weak and problematic, especially after an operation that imposes restrictions in their diet and their lifestyle.4,5,7 In contrast, adolescents and young adults are facing a lot of problems due to obesity. It is not only the metabolic syndrome and the several comorbidities affecting and diminishing their life expectancy, but mainly the psychosocial effects with bullying in school and college, poor self-esteem, depression, nonexistent sexual life, and unemployment.10,13
The studies now existing in the medical literature are not showing different results regarding the morbidity and mortality after bariatric surgery in adolescents and young adults. In fact, some studies show that the 30-day complication rate and mortality are lower than in the adult population undergoing bariatric operation. This population has the potential for better results because of the lesser comorbidities than the older population and their better physical status.3,5,8,14–16
There are some studies of centers placing adjustable gastric bands, but most centers are now performing sleeve gastrectomies and Roux-en-Y gastric bypasses.6,11,16–19 This ongoing shift in the type of procedure is based on the efficacy of gastric bypass and LSG in weight loss, lasting over time. The greater BMI reduction is recorded with laparoscopic Roux-en-Y gastric bypass in studies with 12 or 24 months of follow-up.16,20–22 On the other hand, gastric banding is considered to have lower recorded BMI reduction during the same follow-up periods.2,9,16,19,21,22
In this study the bariatric procedure that was performed was LSG. The main reason was that LSG has the advantage of avoiding any intestinal bypass and the implantation of a foreign body. The result of the operation was a steady weight loss for all the participants during the 24 months of follow-up. At 24 months of follow-up the %EWL reached 81 ± 17%, %EBMIL 96 ± 21%, and BMI difference −18.08 ± 4.38 kg/m2. These results are in accordance with the results in other studies treating obese adolescents and young adults with LSG,9,15,19,23–30 like in the studies of Al-Sabah et al. 30 and Nadler et al., 23 the retrospective data of Sugerman et al., 9 and the large meta-analysis of Black et al. 15 in 2013.
The existence of obesity-related comorbidities in adolescents and young adults is not as common as in the adult obese population. In this study initially only 5.4% had hypertension, 5.4% had diabetes mellitus, and 10.8% had dyslipidemia. It is interesting that after the operation there was a rapid recession of these comorbidities. In 3 months after the operation only 2.7% of patients had still dyslipidemia, and none of them had diabetes mellitus or hypertension. This result lasted during the 24 months of follow-up without any reappearance of these comorbidities. Resolution or improvement in the vast majority of comorbidities recently after LSG is revealed in other studies as well,3,15,26–30 like in those of Sachdev et al., 27 Alqahtani et al., 26 Pourcher et al., 29 and Al-Sabah et al. 30
The latter fact is revealing one of the beneficial characteristics of operative procedures for morbid obesity in adolescents and young adults. In particular, LSG also records high percentages of weight loss in this population. LSG is an efficacious treatment option for morbidly obese adolescents and young adults, especially with the presence of comorbidities. Recovering after surgery of the cardiovascular system should also be accompanied by a recovery in life expectancy and the psychological profile, allowing the adolescent and the young adult to confront life with greater hope and enjoyment of life. 31
The limitations of this study are many. The team is presenting the experience of a bariatric center treating adolescents and young adults. This is a single-institution retrospective review of prospectively collected data with a small sample size. The follow-up is 2 years after surgery. Multicenter studies with a more extensive follow-up period would prove the lasting effect of LSG in weight loss and treating comorbid conditions in adolescents and young adults.
Footnotes
Disclosure Statement
No competing financial interests exist.