
Abstract
Abstract
Background:
Chronic right iliac fossa (CRIF) pain in children is associated with repeated hospital attendance, inconclusive investigations, and missed school days. There is increasing evidence for the role of laparoscopic appendectomy for the management of CRIF pain. However, currently there is no substantial evidence to correlate histological changes identified in the appendixes removed with resolution of pain.
Method:
This study collected prospective data for a single surgeon's series of laparoscopic appendectomy performed for CRIF pain between 2003 and 2014.
Results:
Forty patients with a median age of 13 years (range 5–19 years) underwent laparoscopic appendectomy for CRIF pain. Twenty-nine patients (73%) had macroscopically normal appendixes, but histological changes were identified in 28 patients (70%). Other findings at laparoscopy included gynecological pathology (ovarian/para-ovarian cysts), unfixed mobile caecum, and a well-defined peritoneal band extending from the caecum to the anterolateral abdominal wall (caeco-peritoneal band). Patients were followed up for a median of 2 months (range 1–15 months). All patients reported resolution of CRIF pain.
Discussion:
Laparoscopic appendectomy appears to be an effective treatment for CRIF pain, while also providing the opportunity to diagnose and treat potential sources of CRIF pain other than the appendix. Consistent with the literature, a small number of patients appear to have resolution of pain, despite no histological change being identified in the appendix removed and no other pathology having been identified. The same histological changes commonly seen have also been demonstrated in appendixes removed incidentally. Caution therefore should be applied when interpreting the significance of histological changes seen.
Introduction
C
The advent of laparoscopy has provided both a diagnostic and therapeutic tool for the management of CRIF pain, with minimal associated morbidity. Appendectomy at the time of laparoscopy for investigation of CRIF pain has been associated with resolution of pain in 60%–98% patients.4–7 However, correlation between resolution of pain and the histological changes identified in the appendixes removed remains controversial. 5
The 6-year experience of the senior author of performing laparoscopic appendectomy for the management of CRIF pain in 11 children has been previously published. 2 The data are now presented for a separate cohort of 40 children managed over 11 years.
Method
This study collected prospective data over an 11-year period (2003–2014) for a single surgeon's series of laparoscopic appendectomy, performed for the management of CRIF pain. CRIF pain was defined as right iliac fossa pain lasting ≥1 month, with no identifiable cause, having been investigated with a minimum of routine urinalysis, serology, and an abdominal ultrasound. Data collection included patient demographics, duration of symptoms, comorbidities, macroscopic findings at the time of surgery, length of stay, histological findings, duration of follow-up, and outcome. All hospital episodes and case notes were reviewed for each patient to ensure that following surgical discharge, they did not present to other specialties with ongoing pain.
Results
Forty children underwent laparoscopic appendectomy for CRIF pain between 2003 and 2014. Twenty-seven (68%) patients were female, with a median age of 13 years (range 5–19 years). The median duration of CRIF pain was 6 months (range 1–36 months). Three patients had had previous laparoscopic gynecological procedures: two ovarian cystectomies and one aspiration of an ovarian cyst.
Seven children (18%) had a functional comorbidity, six of whom were female. Three children were under the care of child and adolescent mental health services (CAMHS) at the time of referral. Two of these patients had a history of self-harm and previous suicide attempts, with one of these children having been diagnosed with psychotic depression. Two patients had been diagnosed with chronic pain syndromes, with one child also under CAMHS for emotional abuse. Three patients had a diagnosis of chronic fatigue syndrome.
The senior author was the first surgeon in all cases. Three cases were performed using a single incision, with the remaining 37 laparoscopic appendectomies performed using a standard three-port technique. The median operative time was 40 minutes (range 20–90 minutes). There were no intraoperative complications or conversions to an open procedure. Median length of stay was 1 day. Seventeen (43%) children were discharged the day of surgery, 20 (50%) 1 day postoperatively, and three (7%) 2 days postoperatively.
Macroscopic and histological findings are summarized in Figure 1. Twenty-nine patients (73%) had macroscopically normal appearing appendixes at the time of surgery. However, in 16 (55%) of these patients, another potential source of CRIF pain was identified. Five children were noted to have a gynecological diagnosis (ovarian or para-ovarian cysts); three were noted to have a mobile, unfixed caecum; and eight were noted to have adhesions between the caecum and anterolateral abdominal wall (an entity that the senior author refers to as a caeco-peritoneal band [CPB]). Eleven patients (27%) were found to have macroscopic evidence to support a diagnosis of appendicitis, two of whom were also noted to have a mobile, unfixed caecum. The eight patients in whom a CPB was identified underwent adhesiolysis, and the four patients found to have a mobile, unfixed caecum had a concomitant caecopexy.
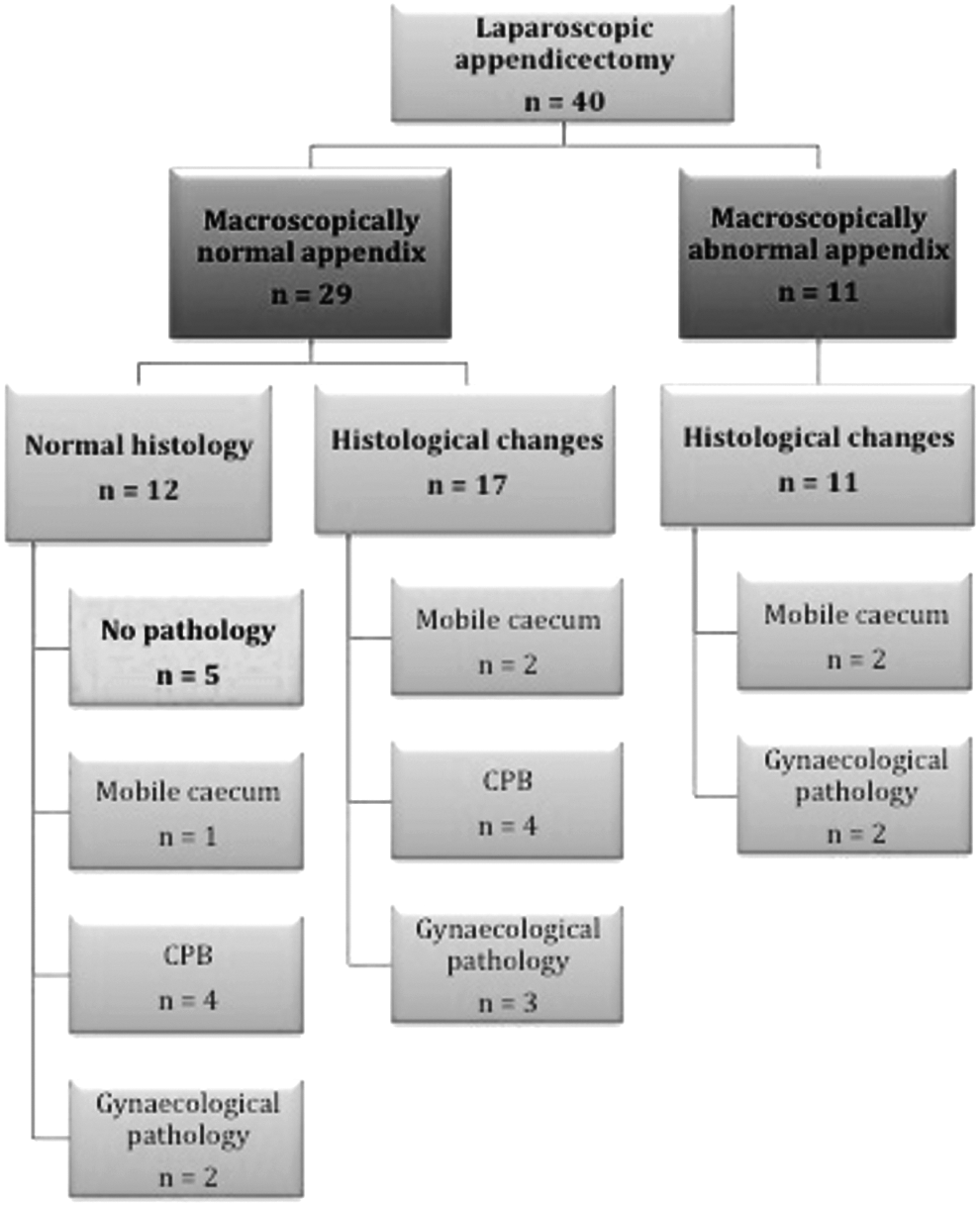
Summary of macroscopic and histological findings.
Histological changes were noted in 28/40 (70%) of the appendixes removed. The most common findings were prominent lymphoid hyperplasia, fecolith, pus in lumen, features of early suppurative inflammation, and distal luminal fibrosis. Of the 12/40 (30%) of patients who had a histologically normal appendix, only five patients had no other potential cause for their pain identified at the time of surgery. Four of the 12 patients with histologically normal appendixes were found to have a CPB, which was taken down at the time of surgery. Two were found to have a para-ovarian cyst, and one child was identified to have a mobile, unfixed caecum and underwent caecopexy.
Of the seven patients with a functional comorbidity, histological changes were seen in the appendixes of five. Two appendixes had features of early suppurative inflammation, one was noted to have prominent lymphoid aggregates and congested vessels, one appendix demonstrated distal luminal fibrosis, and a faecolith was identified in another. In the 2/7 patients with a functional comorbidity who were found to have a normal appendix, one was noted to have adhesions between the caecum and anterolateral abdominal wall, which were taken down at the time of surgery, and the other had a fimbrial cyst excised, which showed histological changes suggestive of torsion.
Follow-up was a median of 2 months (range1–15 months). The period covered by review of case notes and hospital episodes from time of surgery was a median of 5.4 years (range 7 months–11.4 years). All patients had reported resolution of pain prior to surgical discharge, and had been encouraged to contact the senior author if they subsequently developed pain. However, on case-note review, two patients were identified to have reported abdominal pain after surgical discharge. One patient who had been found to have a normal appendix but underwent caecopexy for a mobile, unfixed caecum was subsequently diagnosed with left pelvi-ureteric junction obstruction. This patient had resolution of their left-sided abdominal pain following pyeloplasty. The second patient identified to have ongoing CRIF pain had had macroscopic and histological features of appendicitis. She presented to a gynecologist 10 years following surgical discharge for investigation of ongoing CRIF pain.
Discussion
Chronic recurrent abdominal pain affects 1/10 school-age children. 8 If this pain is localized to the right lower quadrant, an appendiceal pathology should be considered. CRIF pain secondary to chronic appendicopathies remain poorly understood 9 and is thought to be the result of three main entities: appendiceal colic secondary to luminal compromise, chronic inflammation, and recurrent appendicitis.2,7
Diagnosis is difficult, as the pain is usually intermittent, and the child may therefore have a normal physical examination. 7 Currently, no accurate diagnostic test is available, and the role of imaging is limited. Diagnostic laparoscopy with appendectomy offers a means of diagnosing not only appendiceal pathology, but also other potential causes of CRIF pain, which can be treated laparoscopically. This study has demonstrated that laparoscopic appendectomy for the management of CRIF pain can be performed safely, with 43% of patients managed as a day-case procedure, and 50% able to be discharged on the first postoperative day.
The present series suggests that macroscopic assessment of appendiceal pathology at the time of surgery is not accurate. Seventy-three percent of patients were judged to have a normal appendix, but 70% were identified to have histological changes. The use of laparoscopy enabled other potential sources of CRIF pain to be identified and treated. Eight children underwent adhesiolysis for a CPB; five patients had a caecopexy performed for a mobile, unfixed caecum; seven patients had gynecological pathology identified; and one patient was found to have Actinomyces colonization of an otherwise histologically normal appendix.
Interesting findings at laparoscopy that it was thought may account for CRIF pain were a mobile, unfixed caecum in five patients in whom caecopexy was performed, and a well-defined CPB in eight patients. The term CPB has been used to describe a fan-shaped solitary peritoneal band extending from the anterior aspect of the caecum and ascending colon to the anterior abdominal wall. Division of the band resulted in symptom resolution in all patients. CPB has previously been suggested to be a cause of CRIF pain by the senior author. 10 Caecal adhesions have been described in other series of management of CRIF pain with laparoscopic appendicectomy.1,4,11 It is difficult to determine, however, whether these adhesions are an indication of previous appendiceal inflammation, or themselves represent a cause for CRIF pain.
All patients reported resolution of pain prior to surgical discharge. This is consistent with other series in the literature, which have reported resolution of CRIF pain following laparoscopic appendectomy in 60%–98% of patients.4–7 The two patients identified on case-note review to have persistent pain following surgical discharge appear to have had a separate pathology to account for their pain. The first child managed for CRIF pain was found to have a macroscopically and histologically normal appendix but a mobile unfixed caecum for which a caecopexy was performed. Following surgical follow-up review and discharge, the child presented with pain and was diagnosed with left-sided pelvi-ureteric obstruction, which was successfully treated with a left-sided pyeloplasty. The fact that the pathology was left-sided suggests that this is unlikely to have been related to the original presentation with CRIF pain. The second patient identified to have persistent pain was found to have a macroscopically and histologically abnormal appendix and was discharged from surgical follow-up after reporting resolution of pain. She presented to a gynecologist with CRIF pain 10 years after surgery, suggesting that the underlying cause is most likely gynecological in nature.
Perhaps some of the most convincing evidence to support the role of laparoscopic appendectomy in the management of CRIF pain is an adult randomized controlled trial performed in the Netherlands. 5 Forty patients with a minimum 3-month history of CRIF pain underwent a diagnostic laparoscopy. If no abnormality was identified, the patients were randomized to laparoscopic appendectomy or laparoscopic inspection alone. Eighteen patients underwent appendectomy, and 22 patients had laparoscopic inspection alone. A significantly higher proportion of patients undergoing appendectomy reported improvement in pain (14/18 versus 7/22; P = .005), with a 2.4-fold increased chance of improved pain following appendectomy. Of the appendixes removed, 11 (61%) demonstrated evidence of appendicopathy, and seven had no histological abnormality (although 6/7 appendixes classified as “normal” were found to have fecaliths or significant fecal stasis). Of the 22 patients who had been randomized to laparoscopic inspection only, one patient subsequently underwent an emergency laparotomy for a perforated gangrenous appendix, and 11 patients with ongoing pain elected to have a second laparoscopy with appendicectomy, with eight patients subsequently reporting resolution of pain.
The finding that all patients reported resolution of pain, despite appendiceal pathology being demonstrated in only 70%, is consistent with the literature. 5 The most common histological features identified in the present series were prominent lymphoid hyperplasia, fecaliths, luminal pus, features of early suppurative inflammation, and distal luminal fibrosis. Two adult studies in which incidental appendectomy was performed at the time of cesarean section 12 and abdominal hysterectomy 13 revealed histological changes in 20% and 31% of specimens, respectively. The histological features most commonly identified were consistent with the findings in our series: lymphoid hyperplasia, fibrous obliteration of the distal lumen, mucocoele, and foci of acute inflammation.
The fact that both the present series and studies such as that of Roumen et al. 5 have demonstrated resolution of CRIF pain in some patients following laparoscopic appendectomy despite no histological abnormality being identified, coupled with the same histological features thought to be suggestive of appendiceal pathology having been identified in incidentally removed appendixes, raises doubt as to the significance of the histological changes seen.
The seven children who presented with CRIF pain who had a functional comorbidity provide an important warning to the skeptical surgeon. Five of these patients were found to have histologically abnormal appendixes (two with features of early suppurative appendicitis). One patient was found to have adhesions between the caecum and anterolateral abdominal wall, which were taken down, and one had a torted fimbrial cyst excised. All seven patients reported resolution of pain. It is therefore important for the surgeon not to be dismissive of reported CRIF pain in the context of comorbidities such as psychiatric conditions, chronic fatigue syndrome, and chronic pain syndromes.
Conclusion
This series supports current available literature, which has demonstrated resolution of pain in the majority of children undergoing laparoscopic appendectomy for CRIF pain. Laparoscopic appendectomy in children with unexplained CRIF pain is safe, well tolerated, and provides clear visualization of the abdominal and pelvic structures with the opportunity for therapeutic intervention.4,8,9,11 Increased use of laparoscopic appendectomy in the management of CRIF pain may reduce the need for repeated hospital attendances, futile investigations, and missed days off school.
Important studies in adults, such as that of Roumen et al., 5 have emphasized that macroscopically normal appendixes often have underlying appendiceal pathology, which might account for CRIF pain. The ability to perform a blinded randomized controlled trial in adults also removes the possibility that resolution of pain can be accounted for by a placebo effect. Current evidence, however, suggests that caution must be applied to the significance of histological changes identified in the appendixes removed, as these same histological features have been identified in up to a third of appendixes removed incidentally in adults.
Footnotes
Disclosure Statement
No competing financial interests exist.