
Abstract
Abstract
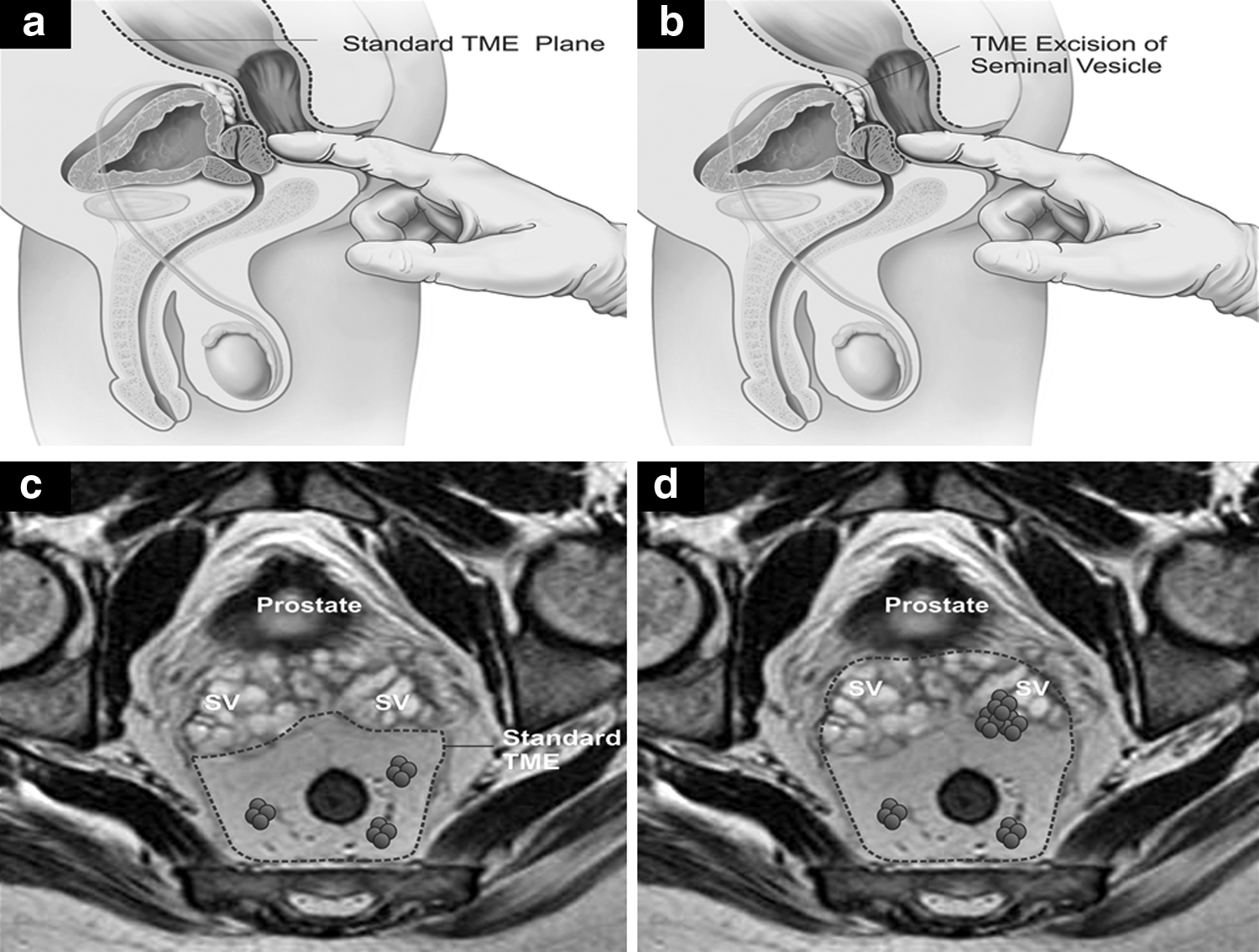
Complete surgical resection remains the primary goal of rectal cancer surgeries. However, in 10%–20% patients, rectal tumors invade adjacent pelvic organs and resection of such organs is essential to achieve an R0 resection. Seminal vesicle is the most commonly involved organ in males. Although laparoscopic surgery has been found to be safe and feasible for rectal cancer surgeries, multivisceral resection is considered complex, and hence majority of these patients are offered open surgical resection. However, with improved surgical expertise as well as better laparoscopic equipment, surgeons have been attempting more complex rectal surgeries through the laparoscopic approach. We are delineating the technical details as well as initial results of laparoscopic total mesorectal excision with enbloc resection of seminal vesicle.
Introduction
N
Technique
A patient is placed in a modified lithotomy position with proper support at all the pressure points. Standard laparoscopic ports are placed and adequate pneumoperitoneum is ensured (Fig. 2). Initial exploration of abdomen and pelvis is performed to ensure absence of liver and peritoneal metastasis. Inferior mesenteric pedicle is ligated at the root or after the origin of the left colic artery depending on the level of the tumor (Fig. 3a). Descending and sigmoid colon are mobilized by scoring the white line of Toldt (Fig. 3b).
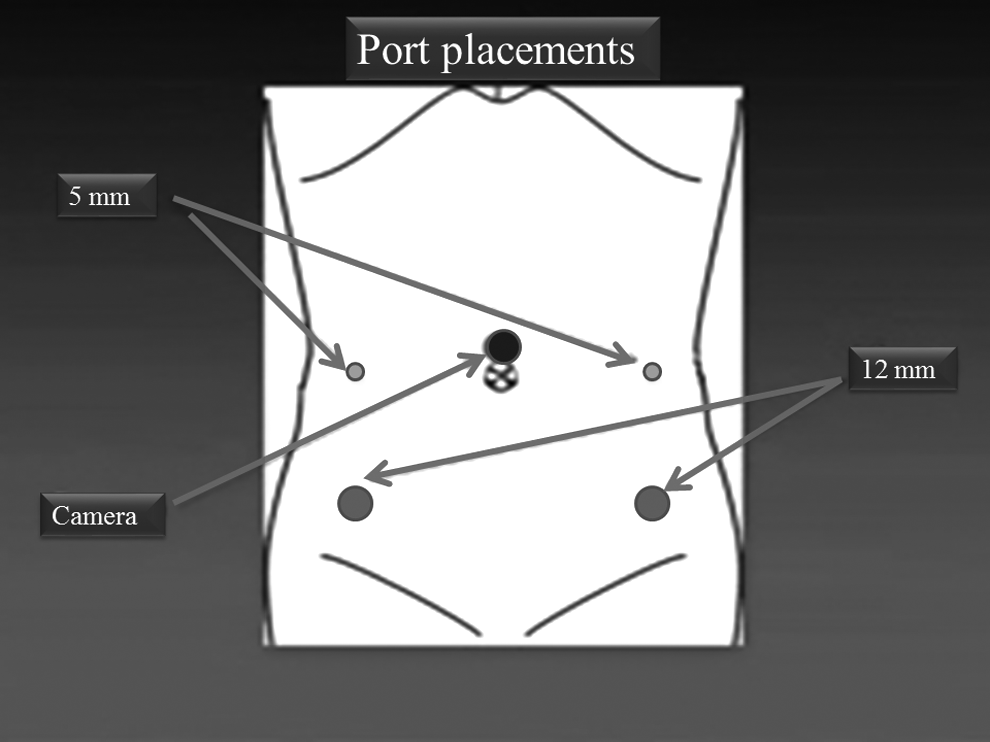
Standard laparoscopic ports for TME with enbloc resection of seminal vesicle.
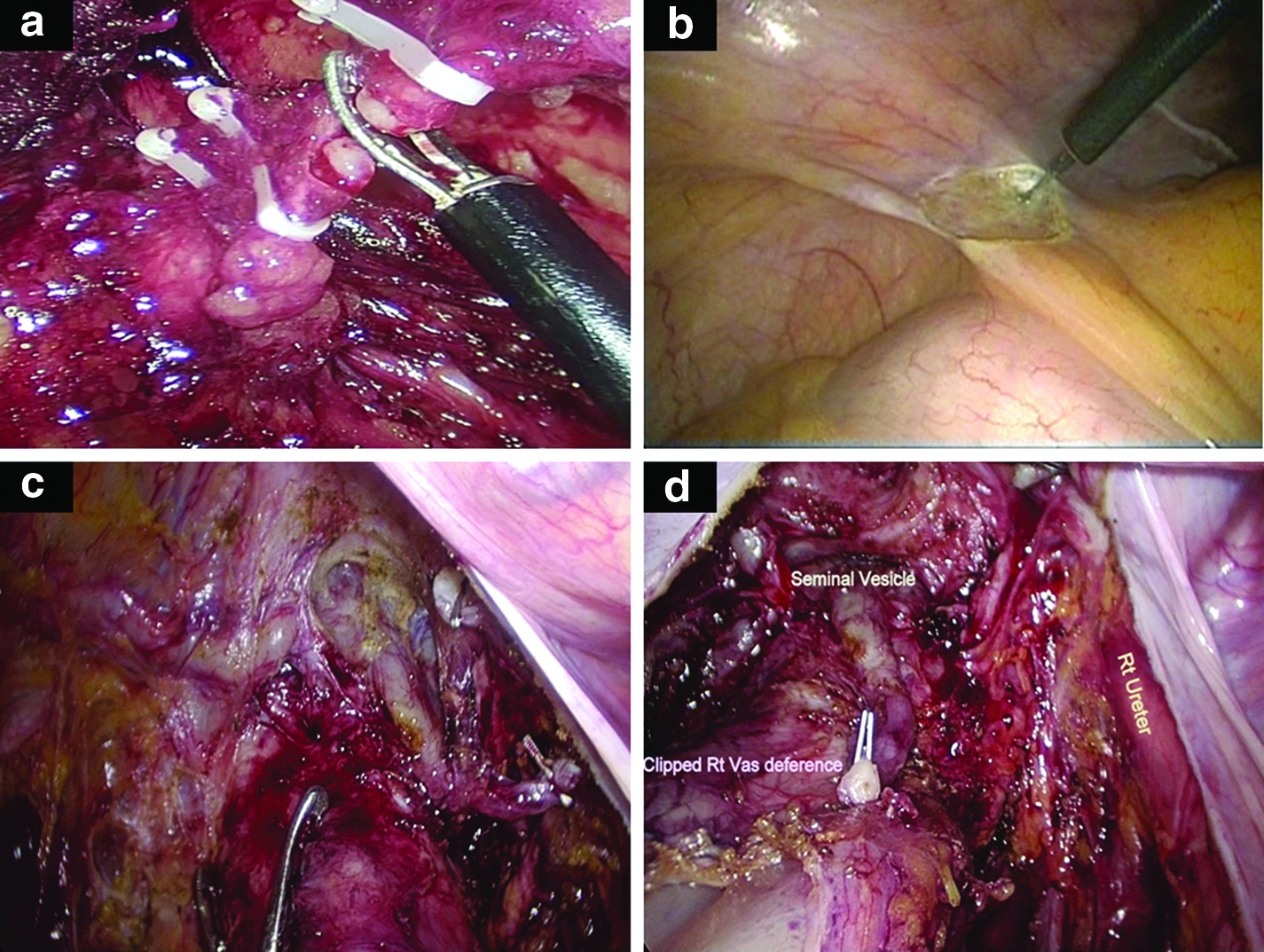
Rectum is then mobilized in the mesorectal plane upto the pelvic floor. Because the tumor is impinging on the seminal vesicle, peritoneal reflection is adherent to the rectal tumor, obliterating the groove for the anterior dissection. As a result, anterior peritoneal cut is undertaken higher on the urinary bladder and peritoneum is reflected on all the sides, avoiding injury to the bladder. The next step would be to identify vas deference, which is then dissected, clipped, and cut (Fig. 3c). The cut end of the vas deference is then traced further till the seminal vesicle is identified. Ureter arches below the vas deference at this point and is defined by dissecting it using a mixter. This is the most critical step in avoiding injury to the ureter. Once seminal vesicle is identified, dissection is continued anterior to it. Anterior dissection is continued till denoviller's fascia is cut and mesorectal fat is visible. Laterally, dissection is continued on the medial aspect of the ureter (Fig. 3d). Whenever unilateral seminal vesicle needs to be resected, dissection is done on the uninvolved side first.
Further lateral and posterior dissection is continued, preserving the lateral neurovascular bundle. Level of transection of the rectum and the type of anastomosis depends on the level of the tumor.
Results
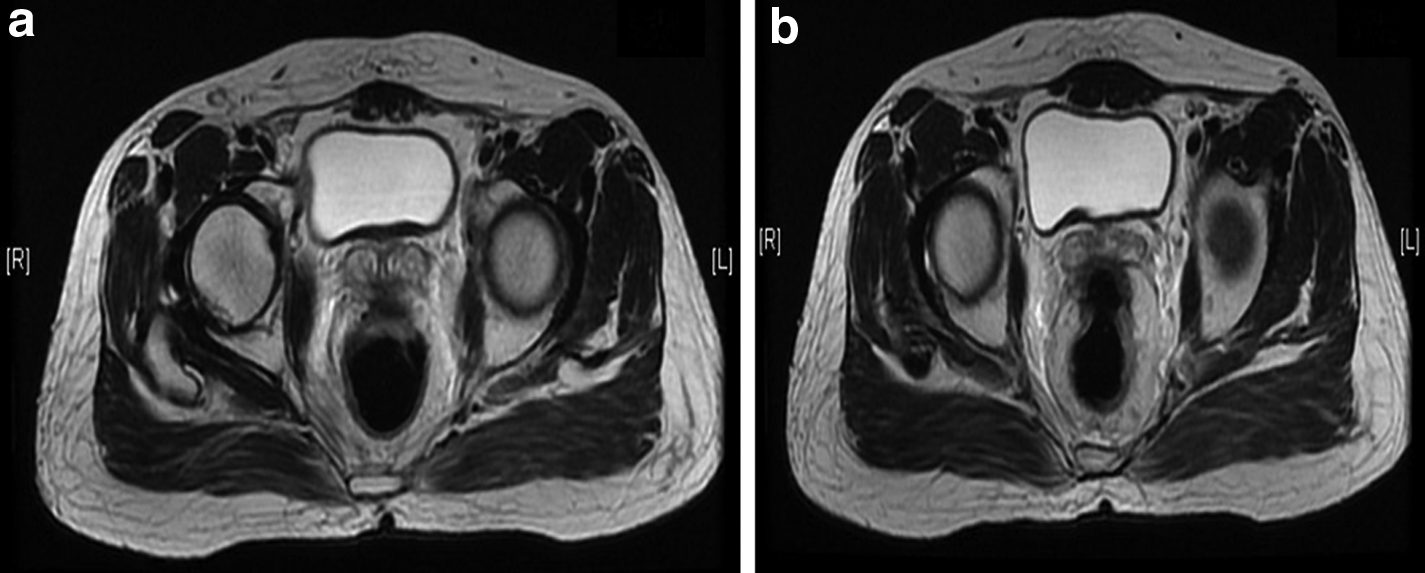
Two patients underwent laparoscopic TME with enbloc resection of seminal vesicle during the time period between July 1, 2013 to July 31, 2015. Patient characteristics are given in Table 1. Inferior mesenteric pedicle was ligated at the root in both patients. No patients had 30-day postoperative morbidity and mortality. Magnetic resonance imaging picture of the second patient is shown in Figure 4.
CRM, circumferential resection margin; NACTRT, neoadjuvant chemoradiotherapy; pT, pathological tumor stage; TME, total mesorectal excision; TX, complete response.
Discussion
Laparoscopic surgery has become a standard surgical procedure in the management of colorectal cancer. It has been found to be associated with significantly lower postoperative pain, faster recovery from paralytic ileus, and hence shorter hospital stay.4,5 Expertise of the surgical team is the single most important factor influencing the outcome. Studies have found shorter operative time and fewer postoperative complications with increase in experience in laparoscopic surgery. 6 Multivisceral resection for rectal cancer is technically demanding even by an open approach and is associated with significant postoperative morbidity. 7 The society of American Gastrointestinal and Endoscopic Surgeons has recommended an open approach for multivisceral resection for colon and rectal cancers. 8 However, with widespread use of laparoscopic surgery and increase in experience with laparoscopic techniques, laparoscopic multivisceral resection has been adopted by a number of colorectal surgeons worldwide.
Nagasue et al. 9 compared laparoscopic multivisceral resection with open resections in a retrospective study and found that median blood loss and hospital stay were significantly lower with laparoscopic surgery. Conversion to open surgery in this series was 6.7%. They concluded that laparoscopic multivisceral resection was safe and feasible in select patients. Similarly, Kim et al. 10 in their retrospective comparison of laparoscopic multivisceral resection with open surgery found similar short-term clinical outcomes. In addition, they also found that 5-year survival and local recurrence rates for the laparoscopic surgery group were similar to those for the open surgery group. However, both these studies were retrospective and included both colon and rectal cancers. In addition, there are no prospective, large studies that have focused on the laparoscopically managed multivisceral resections.
Laparoscopic resection of seminal vesicle has been described for benign seminal vesicle tumors as well as seminal vesicle cysts.11,12 These studies although small have found laparoscopic resection of seminal vesicle tumors safe and feasible without major untoward complications. We describe the technical steps in the surgical resection as well as short-term clinical and oncological outcomes in 2 patients.
Conclusion
Laparoscopic TME with enbloc resection of seminal vesicle is technically feasible with acceptable short-term oncological and clinical outcomes.
Footnotes
Disclosure Statement
No competing financial interests exist.