
Abstract
Abstract
Aims:
One of the challenges of laparoscopic surgery is the time required to perform intracorporeal knots. This can result in considerably longer operating times when compared with the open approach. An example of this is pediatric laparoscopic pyeloplasty, where extensive laparoscopic suturing is required. To reduce the time suturing, the authors developed a new knotting technique for laparoscopic suturing.
Materials and Methods:
The authors modified a neurosurgical knot technique to speed up intricate continuous suturing, and a simple slip-knot-loop suture was created. Twenty continuous sutures were performed with five “bites” of tissue each. Ten were performed with a conventional intracorporeal knot to anchor the suture (Group 1), and 10 were performed using the slip-knot-looped suture to anchor (Group 2). This new knotting technique was used to perform five bowel anastomoses on pig intestine and tested for leaks by distending them with saline for 5 minutes.
Results:
The mean time to perform the suture for Group 1 was 300 seconds, and the mean time for Group 2 was 236 seconds. Unpaired two-tailed Student's t test comparing the means was significant (P < .001). No leaks occurred in any of the five anastomoses.
Conclusions:
This new slip-knot-loop technique modified for pyeloplasty was easy to use, was quicker than conventional knot tying, and produced safe knots and leak-free anastomoses. This knot is transferable to any laparoscopic procedure where continuous suturing is to be used.
Introduction
L
On searching the literature, we found that a neurosurgical team in 2013 developed a sliding knot for suturing dural patches during trans-sphenoidal surgery, reported by Sakamoto et al. 5 The authors described a technique to create a preformed loop using this “slip-lock-knot” for continuous suturing to considerably reduce the operating time and complexity of a procedure. Although the authors proposed this for use in pediatric pyleoplasty, there is no reason why this technique cannot be used in other operations requiring continuous suturing.
Materials and Methods
Slip-knot-sliding-loop suture technique
Initially 30 cm of preferred suture was cut as this left the operator with approximately 20–25 cm of suture after the knot was tied and trimmed, but obviously this can be adjusted to need and preference. The knot was then tied as shown in Figure 1. 5 The authors performed this around a clip, but any stabilizing implement is sufficient.
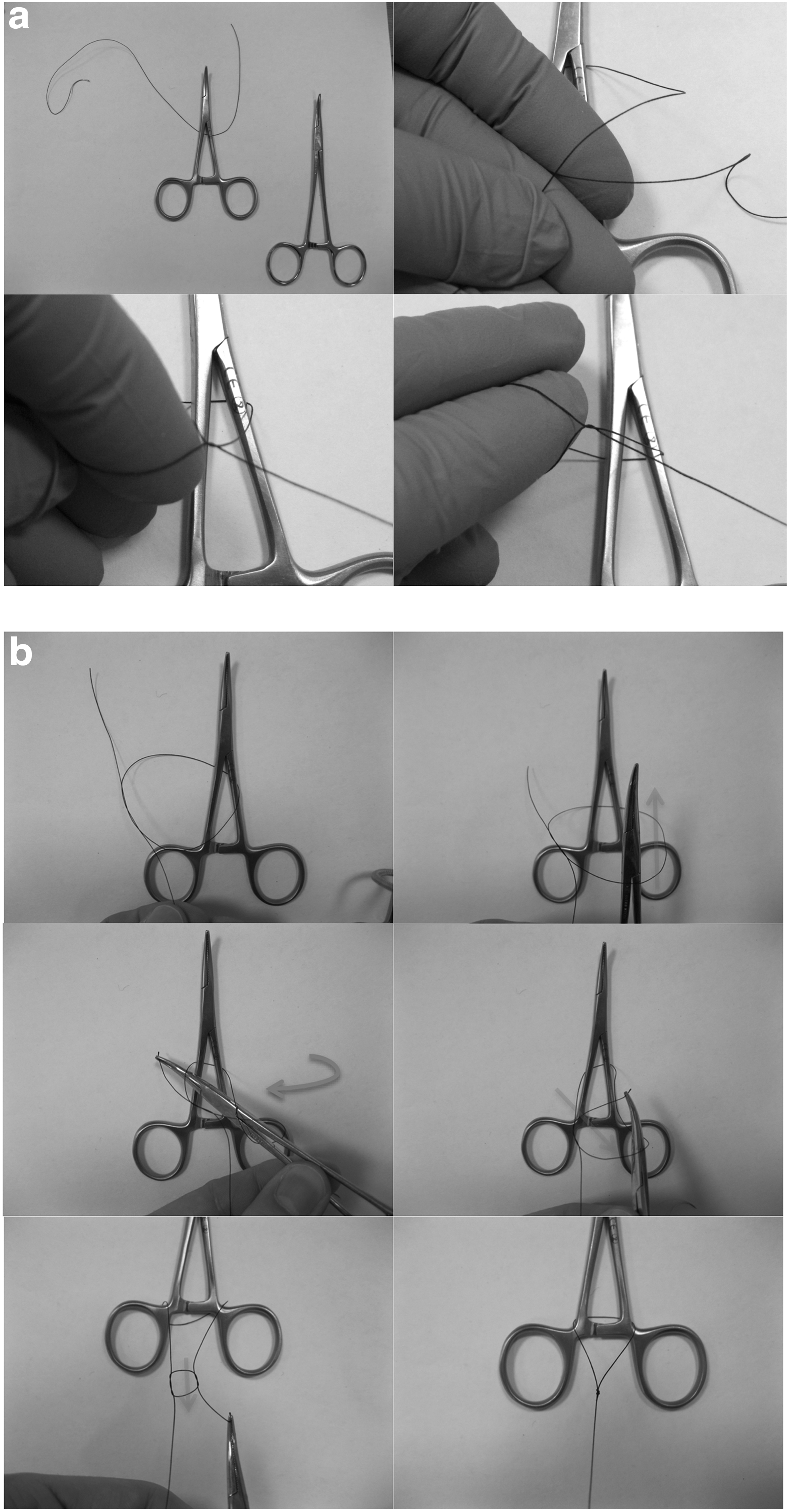
The slip-lock-knot of Sakamoto et al.
5
:
The loop was reduced to a preferred size. We found a loop of approximately 2 cm to be manageable (Fig. 2). If the surgeon finds the port valve mechanism tightens the loop when introducing it, grasping the knot in the jaws of a needle holder instead will prevent this occurring. However, these theoretical concerns proved to be unfounded with an assortment of disposable and reusable ports.
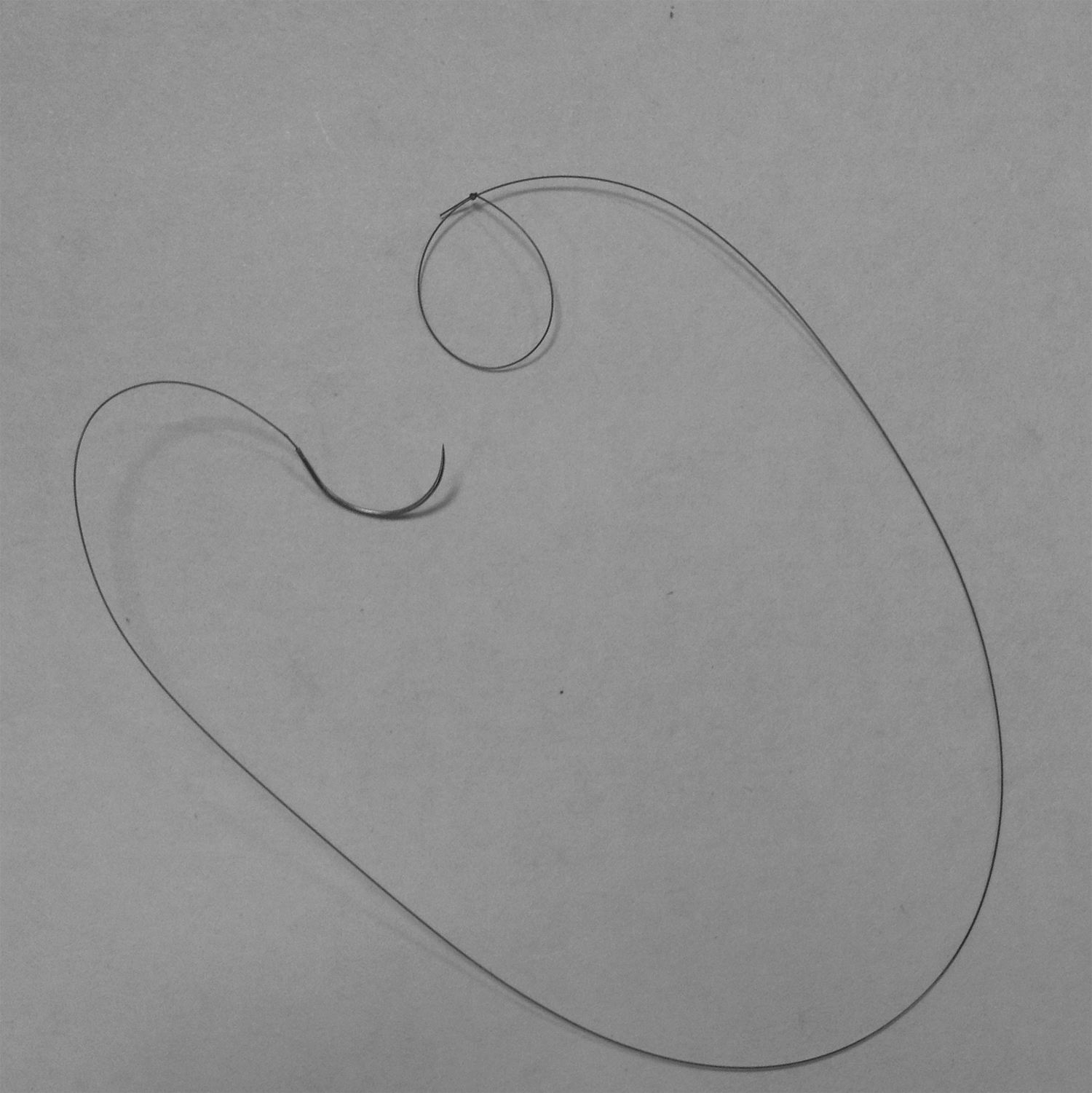
Resulting prelooped suture.
After the anchor “bites” of tissue are placed, the needle is passed through the loop, and the suture is tightened. It is important to visualize the loop snugging to as small as possible to prevent a loose initial “bite.”
When a traditional fixed loop is used after placement of the initial anchor “bite,” then the next “bite” must be taken on the opposite side to the loop to ensure as tight an opposition as possible for the anchor (Fig. 3). This is unnecessary when using the slip-knot-looped suture.
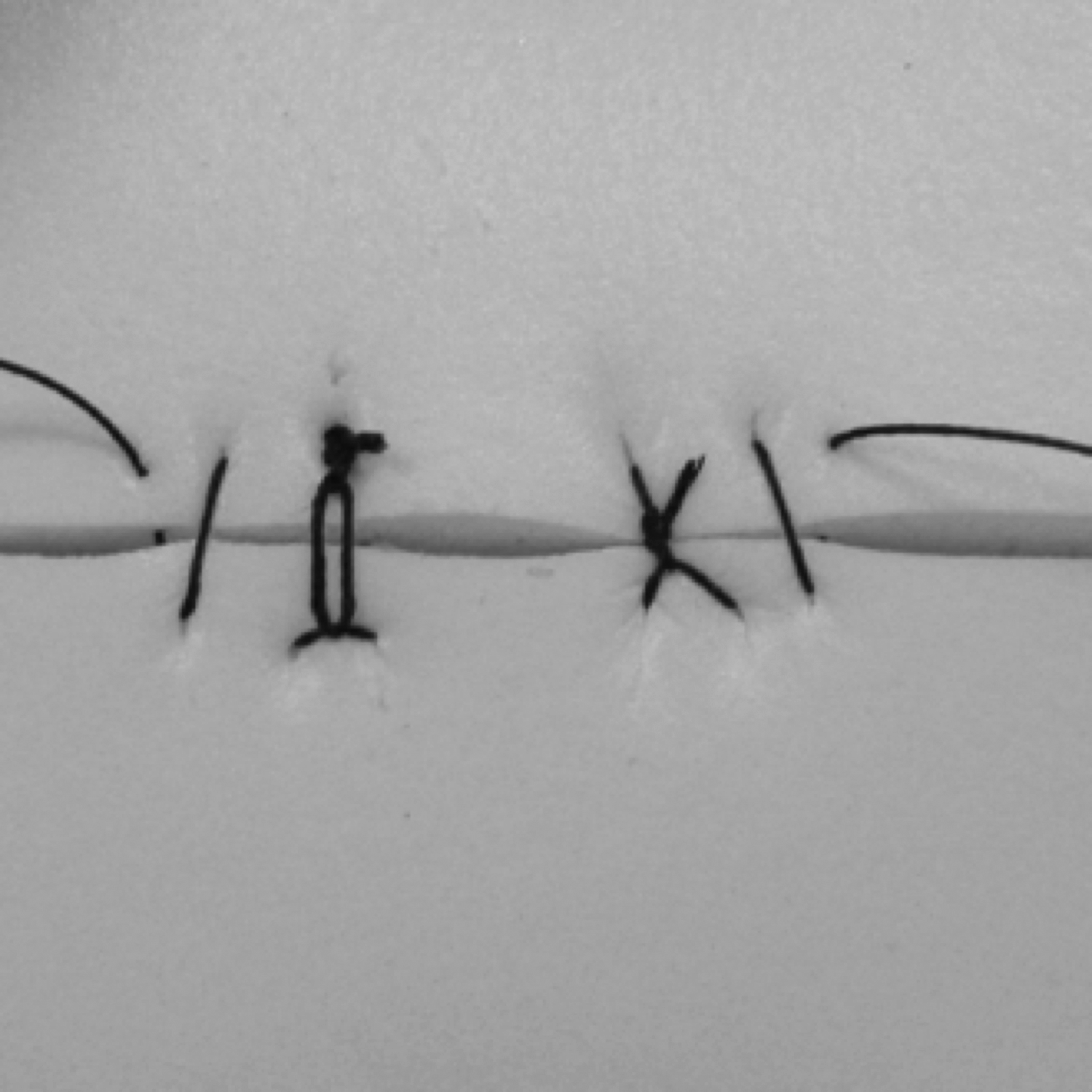
Anchor suture using
Testing of the looped suture
Two tests were performed using the slip-knot-looped suture. The first was to assess the time taken when compared with conventional intracorporeal knot-tying. The second was to assess the watertight nature of a suture performed with this knot.
Continuous suturing
In total, 20 continuous sutures were performed laparoscopically with 2/0 Vicryl (Ethicon) on a silicon benchtop suturing model. Each line of suturing had five bites of tissue. These 20 episodes of suturing were split into two groups. In Group 1, 10 sutures were performed using conventional intracorporeal knot tying for the initial anchoring suture. In Group 2, 10 sutures were performed using the slip-knot-looped suture to anchor. For both sets, the line of suturing was completed with a conventional intracorporeal knot. The slip-knot-looped suture was created using a 25-cm length of suture to produce the loop, and then the excess suture was trimmed. Each episode of suturing was performed by the same surgeon and timed in seconds. To minimize the possibility of surgeon improvement affecting the results, the surgeon would perform a suture from each group alternately.
Animal tissue anastomoses
Five end-to-end anastomoses were performed on pig bowel sourced from MedicMeat using 5/0 polydiaxanone (PDS®; Ethicon) by one surgeon. The slip-knot-loop was used to anchor at the mesenteric border, and a continuous suturing anastomosis was performed, completed with a standard surgeon's knot. Two sutures were used per anastomosis. This bowel was then instilled with saline at pressure with a bladder syringe, with the ends clipped (Fig. 4) for 5 minutes.

Bowel anastomosis under pressure.
Results
Continuous suturing
The times for suturing for the two groups are shown in Table 1. The mean time for Group 1 was 300 seconds, and the mean time for Group 2 was 236 seconds. Comparison of the means using unpaired Student's t test was significant (P < .001).
Time is measured in seconds.
Animal tissue anastomoses
No leaks occurred in any of the five anastomoses.
Discussion
Laparoscopic surgery is a technically challenging skill. 2 The benefits of improved cosmesis, reduced analgesia requirements, and quicker recovery times have long been recognized. 1 However, initial hesitancy and ongoing concerns are often related to the significantly longer operating times when compared with open procedures, especially with the more technically challenging procedures such as pyeloplasty. As a result, novel techniques and equipment have been developed to reduce this, often at great expense. Often the most useful new techniques are in fact a reworking of old knowledge or the application of established techniques to new problems.
Preformed loops have been proposed and used in laparoscopic surgery in different forms,6–8 but not for pediatric pyeloplasty and not as a slip-knot-loop. The preformed loop reduces the need for laparoscopic knot tying and therefore reduces the difficulty of surgery and operating time.6–8 Time is one of the most sensitive markers for technical skill, 9 so if a technique is easier to learn then it can be performed more quickly after fewer numbers of practices. In the current climate of reduced hours of training, attaining the required skill in fewer hours of training is a considerable advantage. Continuous suturing is described and accepted in adult practice of laparoscopic pyeloplasty but is still not common in the field of pediatric pyeloplasty. 10
There are many problems with existing examples of preformed loops that are in the literature.6–8 One technique involves an intricate prelooped suture attached to a device on the needle holder to enable easier throws. 6 The authors found this to be time consuming to set up and still required the creation of a knot intracorporeally. Raymond et al. 7 described a technique to tie a loop on the end of a suture extracorporeally. This technique resulted in a relatively large loop but satisfied the requirement of reducing knot tying intracorporeally. Because the loop plays a part in tissue opposition, a smaller loop is required in intricate suturing. Tying the knot onto a clip rather than an instrument may create smaller loops, but passing the needle through the loop as described by Raymond et al. 7 is often as time consuming as knot tying. Croce and Olmi 8 described multiple knot-tying techniques to create loops on sutures based on various knots with varying degrees of difficulty to tie, but all resulted in the difficulty of a large fixed loop, which results in a loose anchoring suture (Fig. 5). Using a slip-knot-loop negates this problem.
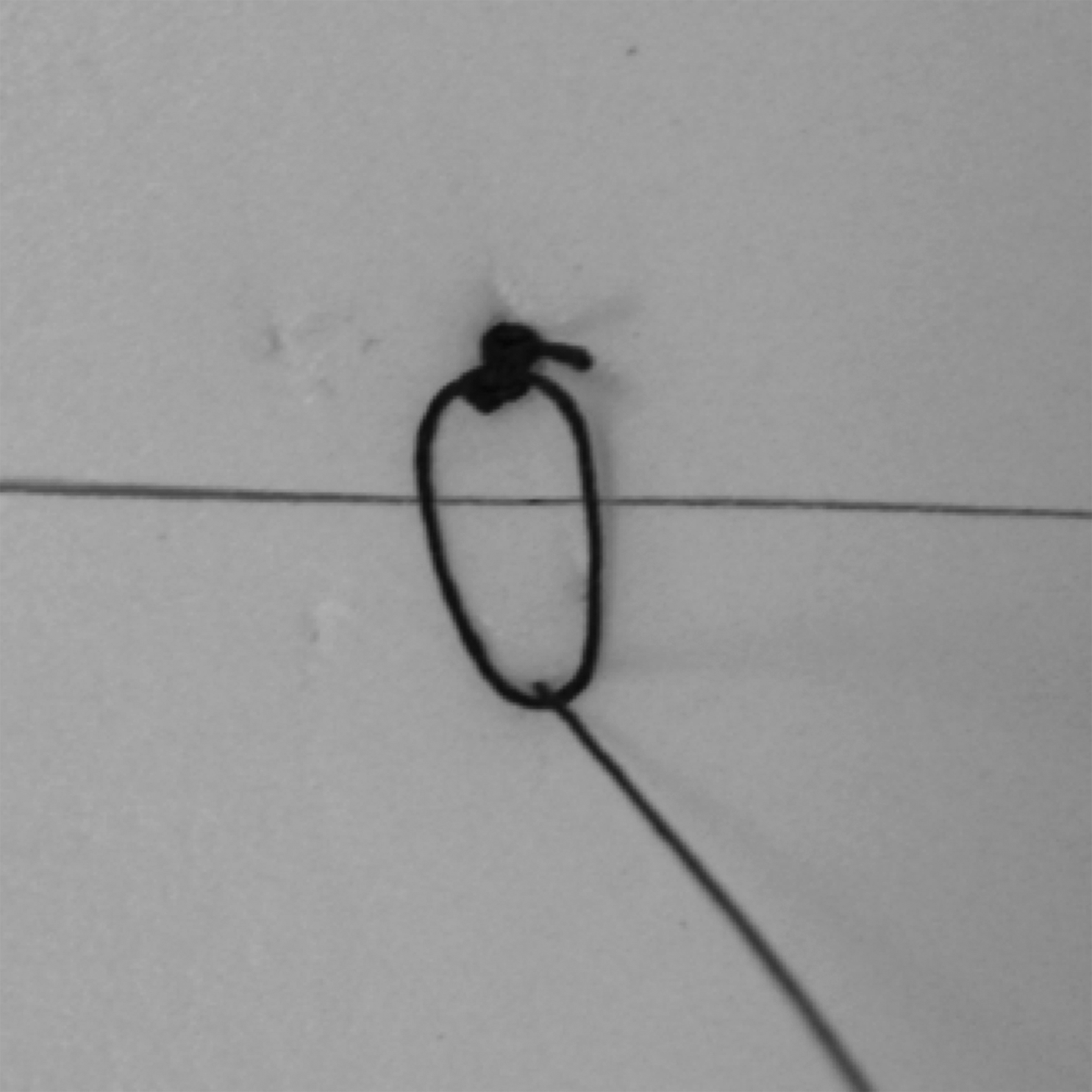
Large fixed loop resulting in a loose anchor suture.
The use of the “slip-lock-knot” by Sakamoto et al. 5 for suturing dural patches is testament to this knot's ability to hold and provide a watertight suture line. In our example we are in fact using the knot to secure the loop and not the tissue, negating the possibility of it “unslipping” due to the direction of forces on the knot. Although in view of the knot's use in neurosurgery for securing dural patches, we suspect this concern is unwarranted anyway.
The concepts of the looped suture or preformed knot are not new and are used on a daily basis from “endolooping” an appendix to closing a midline laparotomy. We are applying this principle to speed up a technically challenging procedure.
From our data the slip-knot-loop saved a minute on each suture. However, the surgeon who performed the suturing is proficient in intracorporeal knot tying. The total time taken for one continuous suture with five “bites” and two knots tied at either end was quicker than some surgeons would spend performing one intracorporeal knot. It is therefore very likely that the time saving is significantly underestimated. Despite this the time saving was still significant.
This technique for creating a looped suture is an additional “string in the bow” of the endoscopic surgeon. In our case the incentive was to reduce the time of pyeloplasty, but in achieving this we have developed a technique that has multiple translations across a wide variety of minimal access procedures.
Footnotes
Disclosure Statement
No competing financial interests exist.