
Abstract
Abstract
Introduction:
Surgical intervention for duodenal atresia most commonly entails duodenoduodenostomy in the neonatal period. Occasionally, type I duodenal atresia with incomplete obstruction may go undiagnosed until later in life. Endoscopic approach to dividing intestinal webs has been reported as successful in patients as young as 7 days of age, and can be a useful modality particularly in patients with comorbidities who may not tolerate open or laparoscopic surgery.
Methods:
A 2-year-old female with a history of trisomy 21 and tetralogy of Fallot underwent laparoscopic and endoscopic exploration of intestinal obstruction as seen on upper gastrointestinal series for symptoms of recurrent emesis and weight loss. After laparoscopy confirmed a duodenal web as the cause of intestinal obstruction, endoscopic division of the membrane was carried out with a triangle tip electrocautery knife and 15 mm radially dilating balloon.
Results:
The patient tolerated the procedure well, and also tolerated full age-appropriate diet by time of discharge on postoperative day 2. She remains asymptomatic as of 6 months postoperatively.
Conclusions:
This report describes a successful endoscopic approach for definitive treatment of a duodenal web in a 2-year-old girl with trisomy 21, and laparoscopy confirmed no intraabdominal obstructive process or complication from endoscopy. Endoscopy enables minimal recovery time and suggests an improved method of duodenal web division over pure surgical intervention.
Introduction
D
Duodenal atresia is often diagnosed in the prenatal period after identification of polyhydramnios and dilatation of the stomach and proximal duodenum (double bubble sign) on screening with ultrasonography. In the absence of prenatal diagnosis, persistent vomiting in the immediate postnatal period and the double bubble sign on abdominal plain film enable the diagnosis. Occasionally, a type I duodenal atresia—duodenal web—causes only a partial obstruction and goes undiagnosed until later in childhood.
Definitive surgical management of duodenal atresia typically occurs in the newborn period and consists of open or laparoscopic duodenoduodenostomy. Those defects that go undiagnosed until later in life, however, provide a unique opportunity to potentially employ a novel endoscopic approach. There are limited descriptions of endoscopic repair of congenital webs in children. Case reports describe laser resection, 5 suction with high-frequency wave snare, 6 and balloon dilation with sphincterotome. 7 The earliest report of endoscopic membranectomy was in 1989, in which authors described successful use of a high-frequency wave cutter to make a “T-shaped” incision. 8 More recent accounts of endoscopic incision of partially obstructing webs have demonstrated efficacy. Endoscopic intervention as early as 7 days of age has been reported as safe and effective. 9 Surgeons have reported excellent outcomes after circumferential 10 and longitudinal 11 incisions using an insulated tip knife and biliary needle knife catheter, respectively. Incising the web with radial cuts alone has also achieved promising intraoperative results as suggested by a luminal caliber sufficient to admit the operating endoscope.12,13 This report describes a successful endoscopic approach to correcting a type I duodenal atresia (partially obstructing duodenal web) using a triangle tip electrocautery knife and balloon dilation.
Case Report
A 2-year-old female with trisomy 21 presented to her pediatrician's office with 2 months of progressive nightly emesis and weight loss. Her medical history was significant for tetralogy of Fallot diagnosed at birth that required repair at 6 weeks of age. She had one hospitalization for respiratory distress secondary to croup and subglottic stenosis at 8 months of age. Of note, an abdominal radiograph at that time showed no abnormalities of the gastrointestinal (GI) tract.
At 1 year of age, she developed episodes of nocturnal emesis of undigested food. These episodes persisted despite dietary modifications and medical treatment of gastroesophageal reflux. Her growth plateaued and began to decline 6 months before presentation. Ultimately, she underwent upper endoscopy, which showed a possible duodenal web, and was referred to pediatric surgery for evaluation.
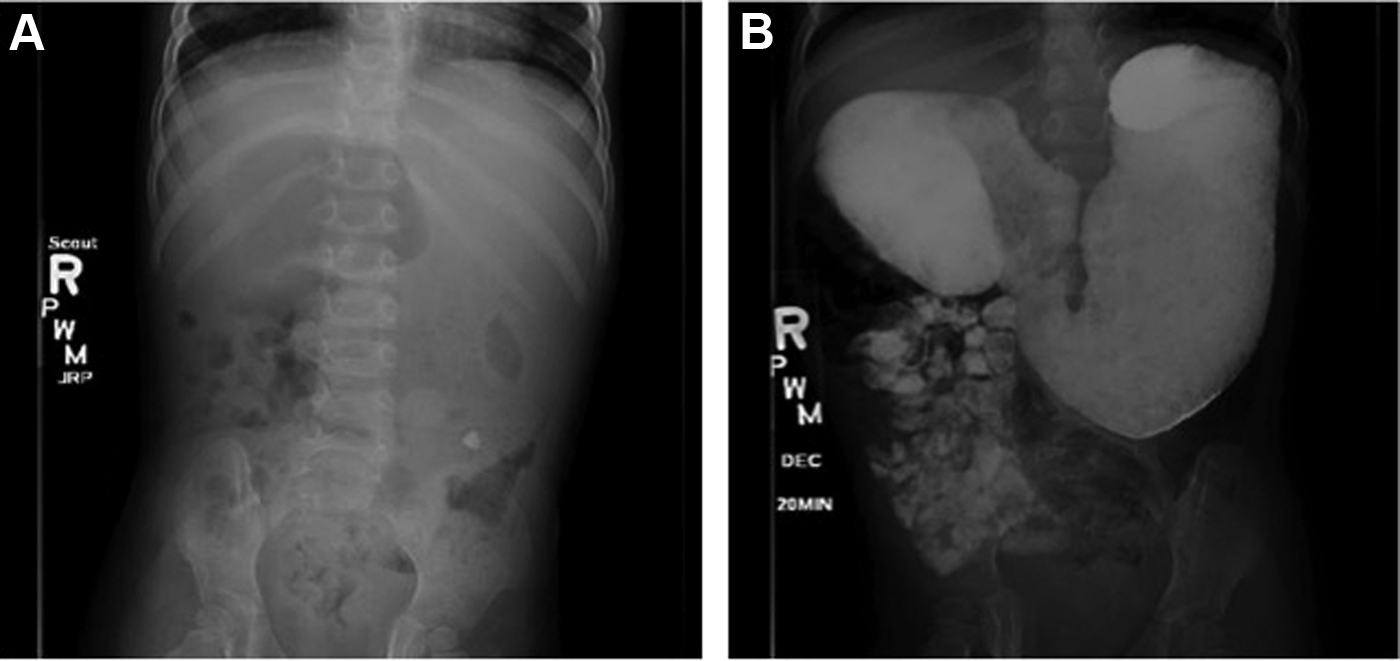
Upper GI series with oral contrast revealed dilated first and second portions of the duodenum proximal to an abrupt transition point, suggestive of an obstructive process (Fig. 1).
Given the endoscopic and radiographic findings suggestive of a web, the patient was prepared for a combined laparoscopic and endoscopic exploration. Initial approach was performed through laparoscopy to rule out causes of partial duodenal obstruction that would not be amenable to endoscopic intervention, including annular pancreas and preduodenal portal vein. The patient's proximal duodenum was noted to be markedly distended with Ladd's bands connecting the cecum to the duodenum in the right upper quadrant. The Ladd's bands were divided, but clearly were not the cause of obstruction.
Upper endoscopy was then performed using a high-definition single 2.8 mm channel upper endoscope (Olympus Medical Systems, Tokyo, Japan) (Video can be viewed online at: www.liebertpub.com/vor); significant debris—undigested food and even a plastic bead—were present in the second portion of the duodenum (Fig. 2A). After copious irrigation, a pinpoint opening was appreciated with some reflux of bile (Fig. 2B). To confirm that this opening led to the distal duodenum, a radio-opaque wire (Glidewire; Terumo Interventional Systems, Somerset, NJ) was passed and fluoroscopy showed the wire to continue into the bowel distally (Fig. 3A). To further confirm the patency of the bowel distal to the web, an endoscopic injection needle in the closed position was passed through the opening and contrast was delivered, opacifying the distal bowel (Fig. 3B). After sufficient verification, the web was endoscopically incised with a triangle tip electrosurgical knife (Olympus Medical Systems), in a radial manner at the superior, lateral, and inferior aspects of the web, avoiding the medial wall to prevent potential damage to the Ampulla of Vater, which had not been seen in the proximal duodenal bulb (Fig. 2C). The endoscope then easily passed through the incised web to see the distal bowel (Fig. 2D).
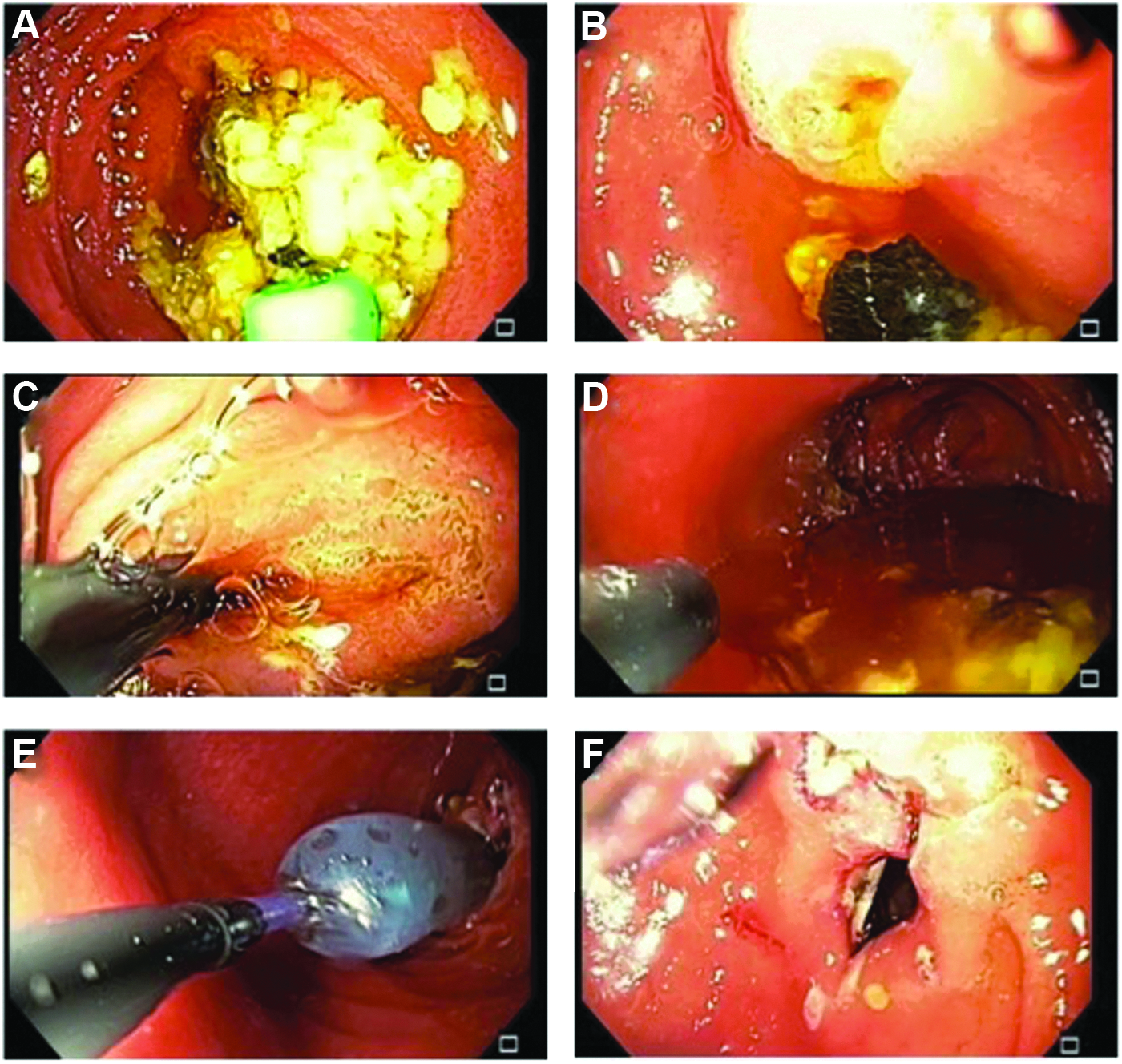
Images from upper endoscopy.
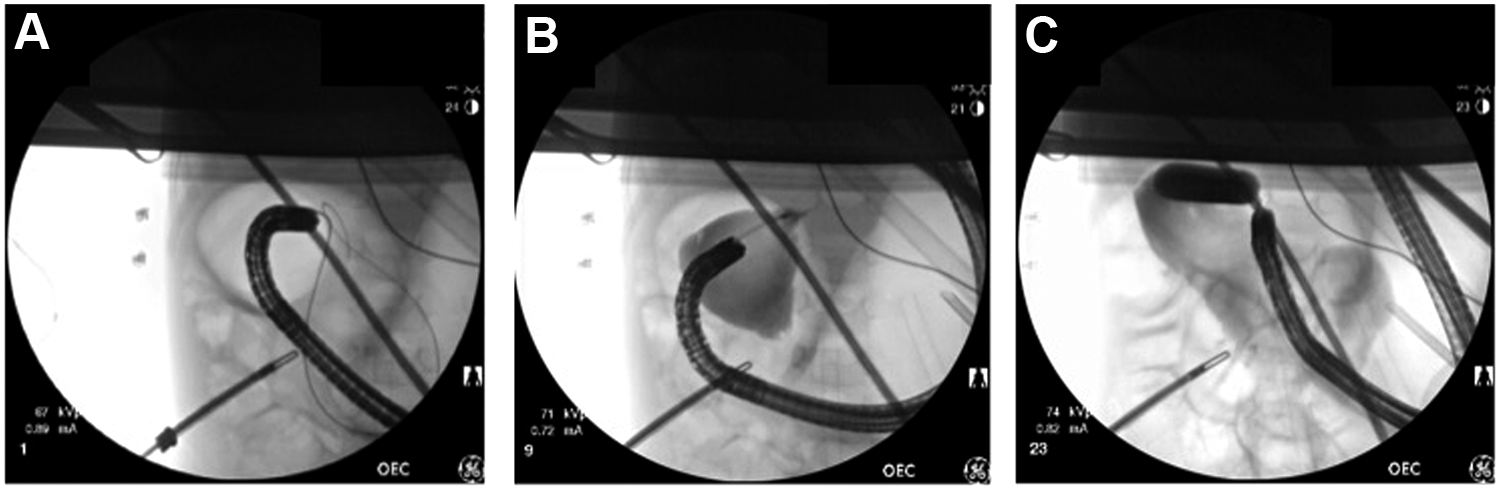
Intraoperative fluoroscopic image shows
A 15 mm radially dilating balloon (Boston Scientific, Natick, MA) was passed through the endoscope to further widen the opening (Figs. 2E and 3C). At the end of the procedure, a generous lumen was visible where the web had been divided and dilated (Fig. 2F). Laparoscopy confirmed no perforation occurred during the endoscopic procedure. Postprocedural fluoroscopy confirmed no leak of contrast, and confirmed rapid transit of contrast into the distal small bowel; abdominal plain film did not have evidence of a residual duodenal web (Fig. 4).

Postprocedural abdominal radiographic contrast study 15 minutes after administration of contrast per nasogastric tube. Divided web was not clearly seen given overlapping loops of bowel, but contrast quickly passed into distal duodenum and proximal jejunum; there was no radiographic evidence of a residual duodenal web.
The patient's postoperative course was uncomplicated, and she was discharged home on postoperative day 2, tolerating a full age-appropriate diet. At her 2-week clinic follow-up appointment, her parents noted that she had more energy, was no longer vomiting, and had gained 2 pounds.
Discussion
Approximately 4% of individuals with trisomy 21 are having duodenal atresia,14,15 and up to 50% of patients with duodenal atresia also have trisomy 21. 1 Other associations with duodenal atresia include renal, vertebral, and cardiac developmental defects.1,2,16–18 Suspicion for intestinal atresia should be high in patients with existing comorbidities—tetralogy of Fallot and trisomy 21 in this patient's case—who present with symptoms of obstruction.
Duodenoduodenostomy is the most commonly performed procedure for an obstructing duodenal web. Although effective, this type of surgery may carry a higher risk in children with significant comorbidities, and typically requires a longer hospitalization. In addition, with an intestinal anastomosis, patients are at risk for complications such as anastomotic leak, megaduodenum, and intestinal stenosis, each of which often requires the need for reoperation.19,20 Laparoscopic duodenoduodenostomy is associated with shorter hospitalization and quicker return to full feeds than open intervention, 21 but does not avoid the risk of anastomotic complications. Endoscopic treatment of duodenal webs appears to result in even shorter hospitalizations and faster return to full feeds than with laparoscopic intervention,10,13 although this has not been formally studied.
Endoscopic intervention is also associated with potential complications and include restricturing,7,22 injury to the Ampulla of Vater, and intestinal perforation. 23 Few case reports, however, discuss adverse outcomes, reflecting either an underreporting of complications or the relatively safe nature of this approach. If there is concern for obstruction secondary to scarring postoperatively, follow-up imaging may be beneficial but should be pursued based on symptoms. In studies where fluoroscopy or endoscopy was performed routinely in asymptomatic patients as part of longer term follow-up, adequate patency of the previously incised web was found.9–11 The patient in this case report had no symptoms as of 6 months postoperatively, and will continue to be monitored closely for stricture or other complications.
We have demonstrated clear symptomatic improvement and short inpatient recovery time with endoscopic division of a partially obstructing duodenal web using radial incisions and balloon dilation. Although endoscopic management of congenital duodenal webs has been reported since 1989, 8 improved technologies in endoscopy are enabling more advanced pediatric endoscopic interventions. Given the relatively few reports to date, long-term follow-up in patients undergoing endoscopic treatment of duodenal atresia is needed to establish efficacy, risk of recurrence, and potential long-term complications.
Consent
An exemption for submitting the following case report to the Institutional Review Board for research approval was granted by the Stanford University Research Compliance Office; this report does not meet the definition of research or clinical investigation.
Footnotes
Disclosure Statement
No competing financial interests exist.