
Abstract
Abstract
Background:
Water-filled laparoendoscopic surgery (WaFLES) has been proposed as a novel surgical system achieving a wide surgical field in the intra- and extraperitoneal space with continuous irrigation of isotonic fluid into the field. Despite its technical feasibility and advantages, the safety of the technique, particularly with respect to physiological functions, has not been evaluated.
Methods:
Various types of minor abdominal surgeries were performed under general anesthesia in nine adult pigs either by conventional laparoscopy (n = 3) or WaFLES (n = 6). In addition to esophageal temperature and body weight, cardiorespiratory variables such as blood pressure, heart rate, and arterial blood gas parameters were compared before and after the surgeries. Blood samples were obtained for assessing changes in biochemical parameters before and after the surgeries.
Results:
Three to seven hours of various surgeries were completed without critical cardiorespiratory events in all animals. Oxygenation and ventilation were maintained regardless of the techniques used for the surgeries. A minor increase of body weight (2.5% of initial body weight), metabolic acidosis, hyperkalemia, and impaired hepatic function were observed after WaFLES surgeries.
Conclusions:
The preliminary study indicated no serious immediate adverse effects of the WaFLES technique.
Introduction
L
Any ideas to improve such problems and achieve better control of inflammatory reactions need to be tested and developed. Igarashi et al. proposed water-filled laparoendoscopic surgery (WaFLES)10–13 as a novel surgical system creating a wide surgical field for intra- and extraperitoneal organs with continuous irrigation of isotonic fluid into the field. The advantages of continuous saline irrigation have been well accepted in cystourethroscopy and arthroscopy, in which bleeding is suppressed by the water pressure and is easily managed by bipolar electrical and microwave devices. 14 Furthermore, the precise internal structure of parenchymal soft organs can be easily identified by intraoperative ultrasonography.
Despite its technical feasibility and advantages, the safety of the technique, particularly with respect to physiological functions, has not been tested. To achieve an efficient irrigation system that immediately removes the blood and floating obstacles from the surgical field, a large amount of saline needs to be continuously infused into the abdominal cavity, possibly causing adverse cardiorespiratory effects in surgical patients. We conducted a preliminary examination of its safety by assessing cardiorespiratory functions and blood biochemical parameters in anesthetized pigs undergoing various surgeries with the WaFLES system.
Materials and Methods
Anesthetic and cardiorespiratory management and surgical procedures
Nine specific pathogen-free pigs, weighing 30 kg (around 12 weeks old), F1 hybrids of the Landrace and the Large Yorkshire, were used for the experiment with the approval of the local ethics committee of Chiba University. Anesthesia induction was performed by experienced veterinarians in accordance with the handling and anesthesia techniques for experimental surgery in pigs. 15
After intramuscular injection of medetomidine (250 μg/kg) and midazolam (500 μg/kg), each pig was anesthetized by lumbar spinal anesthesia for relaxation of abdominal muscle with 0.1 mL/kg of 2% lidocaine under spontaneous breathing of room air. After intravenous injection of thiopental (10 mg/kg), the trachea was intubated, and volume-controlled mechanical ventilation was started with a tidal volume of 350 mL, respiratory rate of 15/minute, and positive end-expiratory pressure of 5 cmH2O.
The femoral artery was surgically exposed and cannulated for continuous arterial blood sampling and blood pressure monitoring. The electrocardiogram was also continuously monitored during anesthesia. Anesthesia was maintained with inhalation of isoflurane 1%–2%. Anesthesia induction and tracheal intubation were performed by an experienced veterinarian. Anesthesia during the surgery was maintained by one of the authors (T.I.) following the advice of an anesthesiologist (S.I.). Saline was administered intravenously at a rate of around 100 mL/hour depending on the amount of bleeding and circulatory status during surgery.
Various types of minor abdominal surgeries listed in Table 1 were performed in nine pigs under either insufflation of CO2 (three pigs: Laparoscopic L1, L2, and L3), or continuous saline irrigation (six pigs: WaFLES W1 to W6) by our surgical team (T.I. and Y.N.). The conventional laparoscopic surgeries with CO2 pneumoperitoneum were performed after insertion of a 10-mm trocar for a laparoscope and pneumoperitoneum and two 5-mm trocars for forceps maneuvering. Intraperitoneal irrigation was not performed after the laparoscopic surgeries.
WaFLES, water-filled laparoendoscopic surgery.
To perform the WaFLES surgeries, a WaFLES irrigation management unit, as previously described,10,11,13 was placed on a 5-cm abdominal incision (Fig. 1). Briefly, the unit consists of a closed recirculating circuit and a 30-cm diameter cistern with a hole connecting the abdominal cavity through the small incision allowing surgeries using an endoscope and surgical retractors. The saline was poured onto the cistern until it fully filled the abdominal cavity and made a 3-cm-deep fluid surface on the cistern. The closed recirculating circuit consisted of two high-powered pumps, a heat exchanger, and a hollow-fiber dialyzer with a surface area of 2.5 m (FDY-250GW; Nikkiso Co. Ltd., Tokyo, Japan).
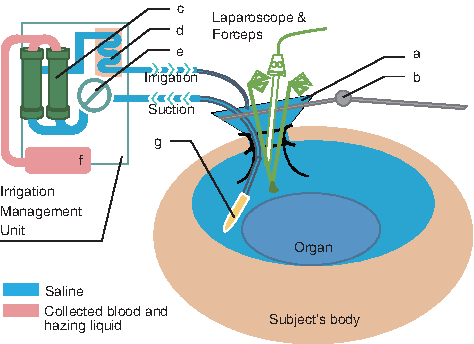
Brief schematic of the components of WaFLES. The cistern
Normal saline was used as the irrigant fluid and continuously introduced into the abdominal cavity through the cistern. The irrigant fluid was collected by a suction tube placed near the surgical site to maintain a clear view of the surgical site even with massive bleeding. The pumps were operated at an irrigation speed of 500–1500 mL/minute, whereas the fluid temperature was maintained around 41°C at the heat exchanger. For surgical maneuver in WaFLES condition, bipolar electric devices and a specially designed microwave coagulation device 16 could be utilized to control bleeding. The technical aspects of the WaFLES surgery and its effectiveness are reported in our related article. 13
Measurements
To assess the effects of anesthesia and the assigned surgical technique on vital signs, such as blood pressure, heart rate, arterial blood gas parameters, core body temperature in the esophagus, and body weight, were compared before and after surgery. Blood biochemical examinations, including electrolytes, blood urea nitrogen (BUN), creatinine (Cre), aspartate transaminase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP), lactate dehydrogenase (LDH), creatine kinase (CK), and interleukin 6 (IL-6) were also performed before and after surgery. Fluid within the abdominal cavity was aspirated as much as possible at the end of WaFLES surgery.
Statistical analysis
Changes of each parameter were evaluated statistically between the beginning of anesthesia and the start point of the surgical procedure, and between the start and end points of the surgical procedure, respectively, with Welch's t-test.
Results
Surgeries were completed without surgical complications in all animals. The WaFLES W5 pig was excluded because of unplanned additional surgical procedures, including an intentional bleeding test at the end of the surgery. The blood sample from the WaFLES W2 pig was considered to be hemolyzed, and its biochemical data were not used for the analyses.
Body weight
As presented in Tables 1 and 2, body weight increased significantly in the pigs at the end of WaFLES surgery by an average of 2.5% of the initial body weight (range 350–1250 g). To explore the mechanisms of the increased body weight after WaFLES surgery, CT images of the brain and thoracic and abdominal regions and T2-weighted MR images (Fig. 2) of the abdominal region were taken in one pig (W6). Careful reading of the images revealed no signs of brain swelling, pleural effusion, or intestinal edema formation, but there was residual fluid within the abdominal cavity.

T2-weighted MRI image of the abdominal cavity after WaFLES. The arrow indicates residual irrigant in the body. There is no sign of edema formation. MRI, magnetic resonance imaging.
n = 4 for blood sampling.
Minimum detection limit for IL-6 is 18.8 pg/mL. Asterisks indicate significant changes (P < .05) during the procedures.
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate transaminase; BUN, blood urea nitrogen; CK, creatine kinase; Cre, creatinine; IL-6, interleukin 6; LDH, lactate dehydrogenase; WaFLES, water-filled laparoendoscopic surgery.
Cardiorespiratory status and core temperature
None of the animals in this study had critical cardiorespiratory events such as hypotension requiring inotropic agents and hypoxemia requiring changes of ventilator settings during the surgeries. As presented in Table 2, blood pressure and heart rate did not change significantly after the WaFLES surgery, whereas the heart rate increased significantly after the laparoscopic surgery despite the small sample size.
Blood gas analyses showed maintenance of oxygenation and ventilation regardless of the surgical techniques, although arterial CO2 was higher during laparoscopic surgery for the same ventilator settings than during WaFLES surgery. It should be noted that the pH in the WaFLES group decreased significantly during the surgery despite maintenance of the arterial CO2 level, while excess of base in animals in the WaFLES condition tends to decrease within positive range.
Core temperature measured in the esophagus did not change significantly during WaFLES surgery, whereas it increased significantly during laparoscopic surgery by 1°C.
Blood biochemical analyses
The serum potassium increased progressively and significantly in both the laparoscopic and WaFLES groups, while the serum sodium and chloride did not change significantly (Table 2). None of the biochemical parameters indicated dysfunction of particular organs such as the kidneys and liver. However, both BUN and Cre, markers of renal function, increased significantly during laparoscopic surgery, and both AST and ALT, markers of liver function, increased significantly during WaFLES surgery. One of the inflammatory markers, IL-6, for which the minimum limit value of quantitation was 18.8 pg/mL, did not increase significantly during the surgeries, suggesting minimal invasiveness in both types of surgical techniques.
Discussion
Surgery within a space filled with saline has been safely performed in urological,17,18 orthopedic,19,20 and hepatic radiofrequency surgeries.21–23 The WaFLES technique is similar to these surgical techniques, but aims to perform surgery within the bigger abdominal cavity adjacent to the cardiac and thoracic cavities. Accordingly, massive saline absorption through the peritoneal membrane, suppression of cardiac output, and impairment of lung function due to the impact of gravity on the adjacent organs are expected complications during WaFLES surgery. In this study, the possible occurrence of these adverse effects of the WaFLES technique was assessed.
Since overload and/or absorption of irrigant were a matter of concern, increase of the body weight was measured. Although the increase of body weight after WaFLES surgery was observed in all animals, it stayed minor (2.5% of the initial body weight on average). The increase could be attributable to summation of absorption of the saline into the interstitial tissue and/or blood through the peritoneal membrane, and residual irrigant within the abdominal cavity after the experiment. Although the residual amount of irrigant may not be critical, the possibility of the absorption mechanism should be explored further, because of its unfavorable surgical outcomes.
In this context, a minor but statistically significant reduction of arterial pH and BE observed during the WaFLES suggests possible development of dilutional metabolic acidosis possibly due to the absorption mechanism.
CT and magnetic resonance imaging (MRI) were operated just in one animal, W6 with 350 g of body weight gain after the surgery. The residual irrigant in the abdominal cavity, which was estimated to be around 60 mL by extracting the high-intensity region in T2-weighted MR images, does not account for the observed weight gain in the pig, suggesting that 80% of body weight gain could indicate absorbed volume of the irrigant. Clearly, the results of this preliminary imaging analysis indicate the necessity for further experiments exploring mechanisms and clinical influences of the body weight during the WaFLES procedure.
During WaFLES surgery, cardiorespiratory function could be impaired due to the impact of gravity and water pressure on the adjacent organs, such as the heart and lungs. However, in this limited experimental setting, blood pressure was stable, and oxygenation and ventilation were maintained throughout the experiment, despite no aggressive therapeutic interventions and the absence of a certified anesthesiologist. Besides, in the Trendelenburg head-down position, for example, the hydrostatic pressure could raise risks of lung atelectasis, leading to hypoxemia, and restrict cardiac contraction, finally leading to lower cardiac output. Furthermore, circulatory responses to acute bleeding and fluid resuscitation during WaFLES surgery might be different from conventional laparoscopic surgery, and must be investigated further.
Core temperature was statistically more stable in WaFLES preparation than the conventional CO2 pneumoperitoneum. This result is probably due to the high quality of the heat exchanger unit developed for the WaFLES procedure and higher thermal conductivity of liquid than CO2. This is a significant contrast to accidental hypothermia induced by irrigation with unwarmed saline during laparoscopic surgery with pneumoperitoneum. 24 Notably, recent evidence indicates importance of temperature control during surgery for reducing postoperative complications such as wound infection. 25 Furthermore, this technique would be of great clinical advantage, particularly for the surgeries requiring organ and tissue protection against ischemic procedures as evidenced by partial nephrectomy26,27 and avoiding thermal tissue injury.28,29
Intra-abdominal pressure suppresses large venous bleeding,5,6 whereas exerts absorption of irrigant in WaFLES modality. Although we did not measure the pressure inside the abdominal cavity, the maximum hydrostatic pressure in the abdominal cavity was suggested below 15 cmH2O (approximately below 11 mmHg) by the MRI image shown in Figure 2. Besides, distribution of the abdominal pressure depends on the depth in WaFLES that is different, absolutely from the uniform pressure in the conventional CO2 pneumoperitoneum. The different nature of the pressure distribution between the techniques would have a different clinical impact on the surgical outcomes in deteriorated circulation of the abdominal organs. For example, circulation of the organs located at the upper level of the abdominal cavity dipped in the irrigant (low-pressure region) would be minimally reduced during the WaFLES surgery.
In this study, the liver and kidneys were partially resected in three pigs for biopsy. If massive saline absorption into the blood had occurred, hematocrit and serum potassium levels would have decreased rapidly, in addition to the development of metabolic acidosis. 30 However, the hematocrit did not change, and serum potassium rather increased, although minor dilutional metabolic acidosis possibly developed as indicated by minor reduction of both pH and BE during the WaFLES procedure. No animals showed apparent organ failures throughout the surgical procedure, however, the rough biochemical assessments might have overlooked minor damage and/or stress in potentially significant vital organs. More detailed and precise analyses using a molecular biological approach should be performed to explore possible silent lesions and effect on organ function in the convalescent periods.
In addition, intravascular induction of bacteria contaminating the irrigant draws was another concern. The hollow fiber membrane installed in the irrigant management system filtered out such contaminating bacteria and debris from the irrigant. Besides, IL-6 level revealed similar elevation compared with the pneumoperitoneum condition. Thus, the irrigation system simply showed washed out effect of contaminated pathogens, and would also be expected to collect live cells, such as blood corpuscles, cancer cells, and adhesion activation factors to establish advanced therapeutic modalities in the future.
This preliminary study revealed no serious and immediate adverse effects of continuous saline irrigation of the abdominal cavity on cardiorespiratory status and blood biochemical parameters in anesthetized pigs. The observed increase of body weight, metabolic acidosis, hyperkalemia, and impaired hepatic function after WaFLES surgery were minor but potentially significant issues. In addition, the water surface level at the cistern was manually controlled in this study. However, in some situations such as surgery for patients with large physique, excessive hydrostatic pressure could be loaded in the lowest area of the abdominal cavity to provoke reduction of blood supply to the abdominal organs. Thus, monitoring of water level at the cistern and/or intra-abdominal pressure on the lowest area should be considered in the future development.
Since the study has limitation in the small sample size and data from the healthy animals, it is not adequate to translate for humans regarding the safety of WaFLES. Full attention is needed at each step in applying the WaFLES surgical techniques on humans in the near future.
In conclusion, WaFLES would be a breakthrough to developing a next-generation, less-invasive, and highly accurate therapeutic strategy, enabling flexible ultrasonic image utilization and preservation of a physiological intra-abdominal environment during surgery. The observed effects on the subjects' bodies by the WaFLES conditions in these animal studies should carefully be considered before advancing into clinical practice.
Footnotes
Acknowledgments
Induction and instruction regarding anesthesia and treatment specialized for pigs were provided by a veterinarian, Dr. Kazuo Watanabe, Piglets Co., Ltd., Asahi, Japan.
Disclosure Statement
This study was funded by a special governmental budget from the Japanese Ministry of Education, Culture, Sports, Science and Technology, and Nikkiso Co. Ltd., Tokyo, Japan under a joint research contract with Chiba University.