
Abstract
Abstract
Objectives:
Transareolar single-port needlescopic thoracic sympathectomy under intravenous anesthesia without intubation has rarely been attempted in managing primary palmar hyperhidrosis (PPH). The objective of this study is to evaluate the feasibility and safety of this minimally invasive technique.
Materials and Methods:
From May 2012 to May 2015, 168 male patients with severe PPH underwent single-port endoscopic thoracic sympathectomy (ETS) and were randomly allocated to groups A or B. Patients in group A underwent nonintubated transareolar ETS with a 2-mm needle endoscope, while those in group B underwent intubated transaxillary ETS with a 5-mm thoracoscope.
Results:
All procedures were performed successfully. The palms of all patients became dry and warm immediately after surgery. The mean resuscitation time was significantly shorter in nonintubated patients than in intubated patients. Postoperative sore throat occurred in 4 patients in group A and in 32 patients in group B (P < .01). The mean incision length was significantly shorter in group A than in group B. The mean postoperative pain scores were markedly higher in group B than in group A. The mean cost of anesthesia was considerably lower in nonintubated patients than in intubated patients. The mean cosmetic scores were higher in group A than in group B (P < .01).
Conclusions:
Nonintubated transareolar single-port ETS with a needle endoscope is a safe, effective, and minimally invasive therapeutic procedure, which allows a smaller incision with less pain and excellent cosmetic results. This novel procedure can be performed in a routine clinical practice for male patients with severe PPH.
Introduction
P
Nonsurgical treatments, such as botulinum toxin, systemic anticholinergic agents, local antiperspirants, and iontophoresis, can only alleviate symptoms transiently and have a high rate of recurrence.5–7 Endoscopic thoracic sympathectomy (ETS) is currently the only effective and sustainable surgical treatment for patients suffering from PPH. 8 Under general anesthesia with endotracheal intubation, transaxillary ETS with 5-mm thoracoscope offers a high level of safety and has obtained a satisfactory therapeutic effect. 9 The surgical procedure has evolved over the past few years in our institution—from a three-port to a one-port method. The issue with the intubated transaxillary procedure is that it still leaves visible scars on the chest wall and associated pain on the trocar sites. This procedure can sometimes cause complications associated with the endotracheal intubation.
With the continued development of endoscopic surgery and anesthesia, video-assisted thoracoscopic surgery without endotracheal intubation is a safe and feasible procedure for the diagnosis and treatment of pleural diseases, 10 including nonintubated needlescopic thoracic surgery. 11 Such procedures can last up to half an hour with adequate patient tolerance and could decrease the complications associated with endotracheal intubation, reduce surgical invasion, and greatly improve cosmetic outcome. This led us to question whether such a procedure could be applied to the simple surgery of ETS.
In this study, we report the results of a randomized comparison of nonintubated transareolar single-port ETS using a 2-mm needle endoscope with intubated transaxillary single-port ETS using a 5-mm thoracoscope.
Materials and Methods
Clinical data
During a 3-year period (May 2012 to May 2015), 307 male patients with severe PPH (palmar sweat was spontaneously dripping similar to a faucet leak when the patient made a fist, 12 or excessive palmar sweat affected patient's work, study, and social activity) underwent bilateral ETS at our institution. All of the patients received a preoperative routine blood examination, cardiological consultation, and chest computed tomography (CT) scan. The CT scan was to exclude patients with preexisting lung, pleural, and heart diseases. In addition, a detailed medical history with the degree of symptoms and the distribution of excessive sweating was also documented.
Enrollment and randomization
The trial was approved by the Institutional Review Board and Ethics Committee of the First Affiliated Hospital of Fujian Medical University. Prerandomization procedures for eligibility of patients consisted of a careful evaluation of inclusion and exclusion criteria.
Criteria for patient inclusion in this study were as follows: age ≥16 years and ≤50 years; male patients with severe palmar hyperhidrosis that significantly affects their daily life; absence of history of thoracic surgery, and severe chest wall deformity; and no contraindication for anesthetic procedures with single-lumen endotracheal intubation. Criteria for exclusion were as follows: female patients; plantar, axillary hyperhidrosis without palmar hyperhidrosis; lung, pleural, and heart diseases such as pneumonia, pleurisy, and pericardial effusion that could increase surgical risk; prior history of thoracic surgery and severe chest wall deformities; secondary hyperhidrosis, including hyperthyroidism, acute and chronic infections, malignancy, and immunologic disorders.
Recruitment began on May 1, 2012, and by the end of May 2015, all patients signed their informed consent forms before undergoing surgery. Each patient was provided with a detailed explanation of the procedure and the goals of the study. One hundred thirty-nine patients were excluded from the study. Among them, 122 patients declined to participate and chose traditional two-port ETS and 17 patients were scheduled to perform traditional two-port ETS because of prior history of thoracic surgery (eight cases) and pleural thickening (nine cases) diagnosed by chest CT.
Randomization was performed by following a computer-generated list. Patients were allocated to group A or group B by using sequentially numbered sealed envelopes with information disclosing the type of procedure to be applied. A total of 168 male patients had been randomly assigned, 85 to receive transareolar single-port ETS using a 2-mm needle endoscope (group A) and 83 to receive transaxillary single-port ETS using a 5-mm thoracoscope (group B). The CONSORT flow diagram is shown in Figure 1.

CONSORT flow diagram.
Surgical procedure
Bilateral sympathectomy in one stage was performed under general anesthesia with a single-lumen endotracheal tube for group B. As for group A, we employed intravenous anesthesia with laryngeal mask (53 cases, Fig. 2a), or face mask (32 cases, Fig. 2b), and endotracheal intubation was not needed. Anesthesia was induced with intravenous propofol (1.5 mg/kg) and fentanyl (50 μg). Throughout the surgical procedure, oxygen was delivered through a laryngeal mask, or face mask, and remifentanil (6 μg/kg/h) and propofol (6 mg/kg/h) were given by target-controlled infusion. Cisatracurium (3 mg) was given only at the beginning of the surgical procedure. The patients in both groups were placed on the operating table in a semisitting position (Fig. 2c), thus exposing axilla or areola to allow a sequential bilateral procedure without the need for turning.

The incision designed for group A was characterized by a 5-mm incision delineated along the areola margin on the operative side of surgery. A 2.5-mm trocar with blunt obturator was introduced into the thoracic cavity. Open pneumothorax was achieved when the trocar's obturator was pulled out. After temporarily disconnecting the ventilation pipe of anesthesia machine, ventilation stopped for 10 seconds and the lung deflated from the vertex of thoracic cavity under gravity and atmospheric pressure. A 2-mm 30° endoscope (Karl Storz, Tuttlingen, Germany) then was introduced into the thoracic cavity. When the trocar was pulled out from the incision, a 2-mm cautery hook was inserted into the thoracic cavity through the same port (Fig. 2d).
Usually the first rib cannot be seen in the thoracic cavity, so the uppermost rib visualized was the second rib (R2), followed by the third and fourth ribs (R3 and R4). Once the sympathetic chain was identified, the sympathetic chain crossing the R4 was simply transected by the cautery hook (Fig. 3a). The tissue adjacent to R4 was also interrupted laterally for 2 cm to include any accessory nerve fibers (the nerve of Kuntz). The planned depth of ablation was to the periosteum of the rib. Once sympathectomy was completed, the cautery hook was pulled out and the trocar was inserted along the thoracoscope into the thoracic cavity. Then the thoracoscope was removed, leaving the trocar in position as a vent for retained air.
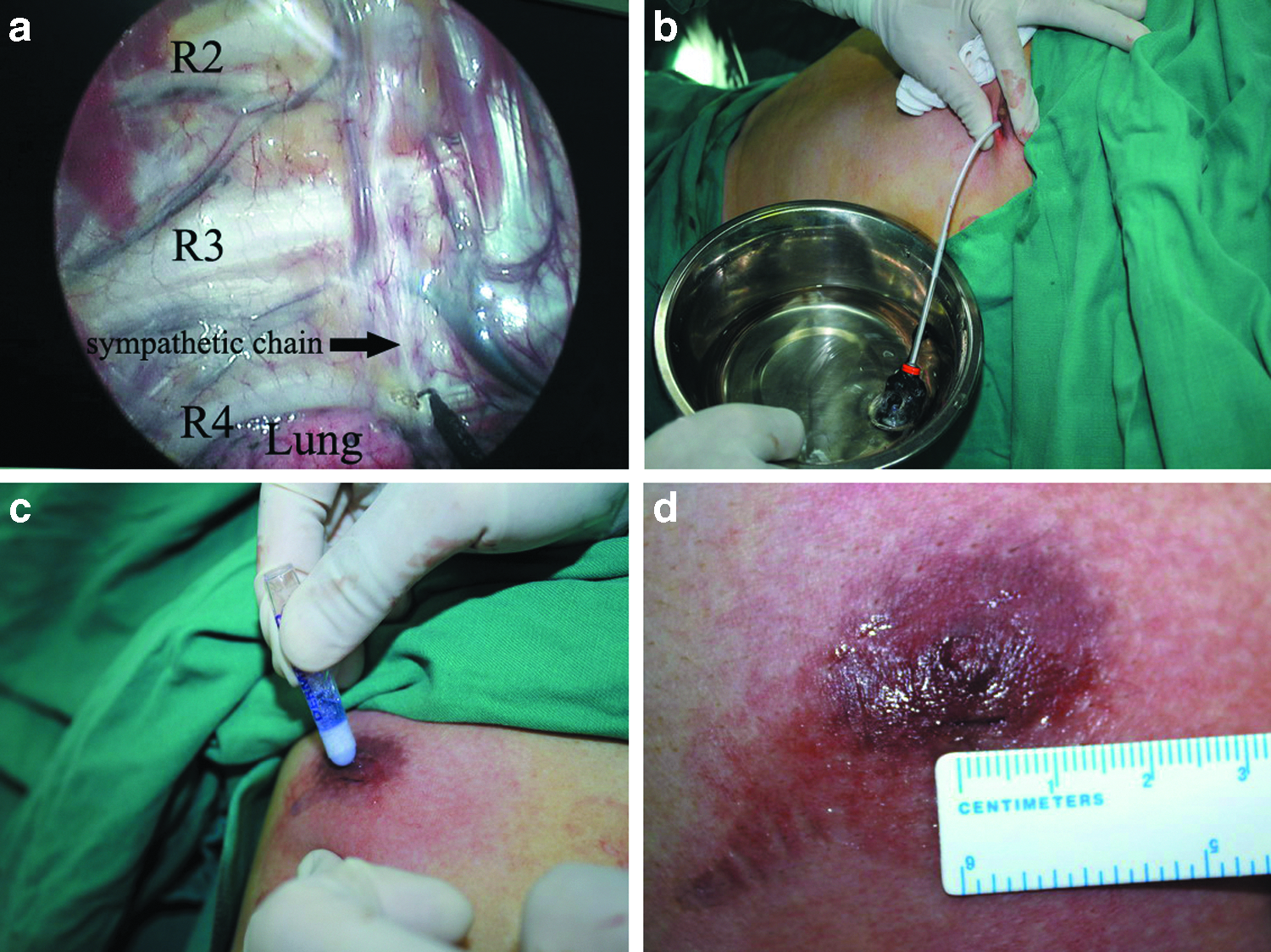
The surgical procedure was completed by insertion of an 8F chest tube into the thoracic cavity through the trocar (Fig. 3b). The chest tube was aspirated while the anesthesiologist ventilated the patient manually, exerting continuous positive pressure for a few seconds, to prevent pneumothorax before the drainage was subsequently removed. At the end of surgery, the incision was tightly pressed for a few seconds to ensure there was no active bleeding. The incision was closed with DERMABOND skin adhesive (Ethicon, West Somerville, NJ) (Fig. 3c, d). No sutures or dressings were needed. The entire procedure was then repeated on the opposite side without changing the position of the patient or the operational setting.
The operative procedure for group B was basically same as group A, except that the needlescopic instruments were replaced by 5-mm thoracoscopic instruments and that the incision was only a single 11-mm transaxillary incision compared with a 5-mm transareolar incision in group A.
Data collection and follow-up
The operating time, resuscitation time, sore throat, resolution of palmar hyperhidrosis, hospital stay, incision length, postoperative pain score, cost of anesthesia, and complications were collected after surgery. The resuscitation time was counted from closing over incisions to the time of patients opening their eyes. Postoperative pain score was assessed at 8 am on the first postoperative day by means of a visual analogue scale, which ranged from 0 “no pain” to 10 “worst pain imaginable.”
The patients were followed up for between 3 and 29 months. The mean duration was 16.7 ± 4.4 months. Patients were required to complete a detailed questionnaire (Table 1). Resolution of symptoms, compensatory hyperhidrosis (CH), cosmetic scores, satisfaction scores, residual pain (postoperative pain lasted for more than 3 months), and incidence of recurrence was evaluated by hospital visits, telephone, or e-mail.
The degree of postoperative compensatory hyperhidrosis was classified as mild, moderate, or severe, according to Cerfolio. 5
Statistical analysis
Statistical analysis was performed using SPSS version 11.5. Variables were expressed as mean ± standard deviation. Comparisons between groups were performed using independent sample t-tests. Pearson's chi-squared test was used to determine the significance of differences between groups for dichotomous variables. Two-sided values of P < .05 were considered statistically significant.
Results
A total of 168 single-port bilateral ETS procedures were successfully performed at our hospital. Age, history of nonsurgical treatments, family history, and distribution of sweating were similar in both groups (Table 2). There was no operative mortality, and conversion to open procedure was not necessary. The palms of all patients became dry and warm as soon as the sympathetic chain was cut off. All patients were monitored for one night postoperatively in case of some serious complications, such as pneumothorax, hemothorax, and arrhythmia. Hospital stay was relatively short, with 164 patients (97.6%) discharged on the first postoperative day and the remainder discharged on postoperative day 2.
The operative outcomes in both groups are shown in Table 3. The vital signs of all nonintubated patients were stable, and none of them converted to endotracheal intubation. The mean resuscitation time was significantly shorter in nonintubated patients (5.6 ± 1.7 minutes) compared to the intubated patients (11.4 ± 2.3 minutes) (P < .01). Postoperative sore throat occurred in 4 patients (4.7%) in group A and in 32 patients (38.6%) in group B (P < .01).
From the time of skin incision to the application of the dressing over the incision. This excluded anesthesia induction and resuscitation time.
The mean incision length was significantly shorter in group A (5.1 ± 0.1 mm) than in group B (11.2 ± 0.8 mm) (P < .01), and the mean postoperative pain scores were markedly higher in group B (3.2 ± 0.9) than in group A (1.1 ± 0.9) (P < .01). Eight patients (9.6%) in group B required analgesia after surgery, whereas none of the patients in group A required analgesia (P < .05). The mean cost of anesthesia was considerably lower in nonintubated patients (3017.6 ± 299.3 RMB) than in intubated patients (5155.4 ± 228.6 RMB; P < .01).
There was no difference in terms of mean operating time and transient postoperative sweating between the two groups. Postoperative complications were minor. Two patients in group B had intraoperative bleeding secondary to injury to a paravertebral vein. The bleeding required insertion of a second trocar and the application of an endoclip, and open surgery was not required. Postoperative pneumothorax was found on the chest X-rays of six patients, three of which resolved after chest drainage for 1 day; the other three patients did not require further intervention. Neither Horner's syndrome nor wound infection was observed in any patient.
Follow-up was 100% complete. One hundred forty-two patients (84.5%) returned the questionnaire within 3 days after receiving the questionnaire, and 26 returned it after a reminder or repeated mailing. The mean follow-up time of group A and group B was 16.3 ± 2.7 and 16.4 ± 3.5 months, respectively. There was no significant difference between group A and group B in terms of mean follow-up time. Outcomes of follow-up after surgery are shown in Table 4. The mean cosmetic scores were higher in group A (3.9 ± 0.3) than in group B (3.2 ± 0.5; P < .01). There were no significant differences between the two procedures in terms of resolution of symptoms and CH, or satisfaction scores. Residual pain occurred in 14 patients (16.9%) in group B, whereas only 3 patients (3.5%) in group A had residual pain (P < 0.01). No recurrence of symptoms was observed in either group.
Discussion
Under general anesthesia with endotracheal intubation, transaxillary ETS is widely used in the treatment of patients with severe PPH. Despite its persistent effectiveness, high safety, and cosmetic benefits,13,14 transaxillary single-port ETS with a 5-mm thoracoscope still has some shortcomings to be improved. To begin with, endotracheal intubation can easily cause postoperative sore throat, dysphagia, and even possible cardiopulmonary complications. More importantly, the cost of general anesthesia with endotracheal intubation can run as high as 5000 RMB, which is more than intravenous anesthesia without intubation. Finally, ETS through single transaxillary incision still leaves visible scars on the chest wall; this results in a permanent cosmetic defect, postoperative wound-related pain, numbness, or paraesthesia.
The aforementioned shortcomings can be overcome with the implementation of transareolar single-port ETS by utilizing a 2-mm needle endoscope. The results are consistent with those of previous reports of ETS.15,16 All patients woke up quickly from anesthesia, and none of the patients complained about sore throats after surgery. The effectiveness of palmar hyperhidrosis was 100%; none of the patients required open surgery.
Incidence rates of Horner's syndrome, the pathogenesis of which consists of direct or indirect lesions of the stellate ganglion, vary considerably and have been described as ranging from 0.5% to 17%. 17 In our study, no patients developed Horner's syndrome, possibly because the sympathetic level of R4 ablation is distant from the stellate ganglion. The frequency of recurrence of PPH is variable (1%–27%). 18 The most common causes of recurrence are anatomic variability of the sympathetic chain, nerve regeneration, or, more importantly, incomplete nerve ablation. In our study, there was no recurrence observed during the follow-up period. This is probably because the sympathetic ganglion and the nerve of Kuntz were completely ablated.
The most common early postoperative complication was pneumothorax. However, exertion of continuous positive pressure for a few seconds in coordination with the anesthesiologist before the closure of the skin incision can successfully prevent pneumothorax.
CH is one of the most problematic complications of sympathectomy, which is characterized by excessive sweating from some regions of the body where it had not been observed preoperatively. The incidence of CH varies between 4.9% and 100%.19–22 This wide variation may be attributable to different levels of nerve ablation, emotional stress, or a variety of definitions of CH. In group A, CH occurred in 36.5% of patients, most of which were mild to moderate. The most affected areas were the back, thorax, abdomen, and lower extremities. However, the symptoms were not severe enough to interfere with lifestyle and this required no further treatment. The pathogenesis of CH remains unknown, but may represent an augmented local sweat rate from skin areas with uninterrupted sympathetic innervation based on evaporative heat balance requirements. 23
Follow-up results revealed a better cosmetic outcome in group A. However, the satisfaction scores were not significantly different between groups A and B. We consider the level of satisfaction to depend mainly on whether the symptoms resolve. Because the resolution rate of palmar hyperhidrosis was 100% and no recurrence was found in either group, similar satisfaction scores should be considered as reasonable.
In comparison with transaxillary single-port ETS, this novel procedure has more advantages. First, an analgesic and an amnestic, remifentanil and propofol, are used by target-controlled infusion throughout the surgical procedure, the patients did not experience or remember pain. After surgery, most of the patients regained consciousness quickly from anesthesia and only four of them complained about sore throat. Therefore, the procedure greatly reduced the costs of anesthesia for patients. Second, with a single 5-mm incision on the areola margin hidden in the color of the areola, this needlescopic procedure is nearly scarless and achieves an excellent cosmetic effect. Third, this procedure with needlescopic instruments only needs a single small transareolar incision, which could greatly reduce postoperative wound-related pain. Last, this newly designed transareolar incision avoids the defect that the trocar restricts the operative direction of thoracoscope and electrocautery in other types of single-port ETS during operation. As a result, our technique could simplify the surgical procedure and offer a higher level of safety. However, transaxillary single-port ETS could avoid the risk of injury to the mammary gland and is more suitable for female patients.
While an improvement over the traditional method, the described procedure still has some shortfalls that need to be overcome. First of all, as this was the primary evaluation of such a technique, we restricted the criteria for inclusion to male patients. Moreover, the 2-mm needle endoscope was comparatively thin; this fragile characteristic of the needle makes it more susceptible to breakage during the operation. Third, we routinely used chest CT preoperatively to exclude diseases affecting the operation that would increase the cost of examination. Finally, the smoke generated from ablating the nerve may affect the surgical view and increase the surgical risk. The troublesome smoke, which also had an impact on group B, cannot be easily removed from the chest cavity because the thoracic cavity is isolated from the atmosphere. Effective methods should be taken to solve the problem.
To our knowledge, these are the first clinical applications of a needle endoscope through a single areolar incision to perform ETS. This study demonstrates that transareolar single-port needlescopic thoracic sympathectomy under intravenous anesthesia without intubation is a safe, effective, and minimally invasive therapeutic procedure for PPH, which provided excellent cosmetic results and less pain as a consequence of a smaller incision. This novel procedure is a promising technique that can be performed in a routine clinical practice for male PPH patients.
Footnotes
Acknowledgment
The research was supported by the Key Program of Scientific Research of Fujian Province (Grant No. 2015-ZQN-ZD-22).
Disclosure Statement
No competing financial interests exist.