
Abstract
Abstract
Objectives:
To describe the initial experience of retroperitoneal laparoendoscopic single-incision radical nephrectomy (LESI-RN) without special platforms and use of conventional laparoscopic instruments and assess the safety and feasibility of LESI-RN.
Subjects and Methods:
Twenty patients who underwent LESI-RN were enrolled in this study. A 5-cm arc skin incision was performed at the midpoint between the costal arch and iliac crest on the midaxillary line. Trocars of 10, 5, and 11 mm were placed at the middle, left end, and right end of the arc incision, respectively. Demographic parameters and perioperative data were retrospectively analyzed and compared with the patients who underwent conventional retroperitoneal laparoscopic radical nephrectomy (LRN).
Results:
The LESI-RN patients had a significantly lower visual analogue scale (4.4 ± 1.9 versus 5.6 ± 1.4; P = .031) and analgesic requirement (18.5 ± 11.2 versus 28.6 ± 16.1; P = .026) compared with the conventional LRN group. The operation time in the LESI-RN group was longer than that in the conventional LRN group (P = .001). The two procedures were essentially similar in terms of the time to liquid intake and hospital stay after operation (P > .05).
Conclusions:
LESI-RN is a safe and feasible surgical strategy, which combines the common principles of using straight instruments and working triangulation in conventional LRN with advantages of cosmesis and minimal invasiveness in laparoendoscopic single-site surgery. The surgical and oncological efficacy of LESI-RN is similar to that of conventional LRN but with significantly improved control of postoperative pain and cosmetic results.
Introduction
L
With the continuous development of minimally invasive techniques, a single-incision approach, laparoendoscopic single-site (LESS) surgery, was developed and has been applied to conventional laparoendoscopic surgery. LESS surgery has many advantages compared to conventional multiport laparoscopic surgery, including improved cosmesis, reduced postoperative pain, and quicker convalescence. 4 However, LESS often needs special single-access platforms, such as TriPort, AnchorPort, or GelPOINT, and some special laparoscopic instruments, such as curved grasper, which have the potential to increase extra expense and limited its application, especially in some undeveloped area.5,6 Although some reports had described the application of homemade single-port instruments for urological procedures,7,8 it still requires additional time, and the device is not easily constructed.
Most of the LESS nephrectomy procedures often use the transperitoneal route, and the procedures were performed with the special LESS platforms mentioned above.6,9,10 Raman et al. 11 first reported LESS nephrectomy using three single ports through one incision without special platforms. However, the articulating laparoscopic grasper and deflectable tip video laparoscope were used for constructing the working triangulation. Nagele et al. 12 had made some innovation for this technique. In their procedures, three trocars were placed through one three-fourth umbilical incision in the umbilical fold, and LESS nephrectomy was performed with conventional instruments. Enlightened by their experience, we tried to use this technique in LRN.
There have been a few reports of LESS nephrectomy with retroperitoneal approach, and special platforms were also used in those procedures.2,13–16 Few reports concerned about comparison between the retroperitoneal LESS nephrectomy and conventional LRN. In the present study, we describe our initial experience of retroperitoneal laparoendoscopic single-incision radical nephrectomy (LESI-RN) without any special LESS platforms and the use of conventional laparoscopic instruments. Additionally, we assess the safety and feasibility of LESI-RN and compare variables with those of conventional LRN done by the same surgeon in our institution.
Subjects and Methods
From January 2012 to October 2014, a retrospective study of patients with RCC who underwent LRN was conducted in our institution. All the cases were evaluated by computed tomography and routine laboratory tests preoperatively. The indications for the LRN were cases of T1 tumor stage without evidence of lymphadenopathy or renal vein involvement. In addition, the cases in this study were not candidates for partial nephrectomy due to the tumor location (i.e., localization in the hilum or significant involvement of pelvicalyceal), or the patient decided to undergo a radical nephrectomy despite the selective indications for partial nephrectomy. The R.E.N.A.L. nephrometry score (RNS) was used to classify the tumors. The nephrometry scores were generated and verified by two physicians familiar with the RNS. Tumors with nephrometry scores totaling 4–6 were considered low complexity, 7–9 were considered moderate complexity, and 10–12 were considered high complexity. 17 All patients had discussed the risks and benefits related to the procedures of radical nephrectomy and partial nephrectomy before they made decisions. If the patient decided to undergo the LRN, the possibility of LESI-RN was proposed. The exclusion criteria were a body mass index (BMI) >30 kg/m2, American Society of Anesthesiology (ASA) score >2, and the inability to provide written informed consent.
Twenty patients who underwent LESI-RN were enrolled in the present study. For comparison purposes, the same number of demographics-matched patients with RCC of comparable tumor stage and tumor size who underwent conventional LRN was also enrolled. LESI-RN and conventional LRN were performed by a single surgeon who was proficient in both techniques. All patients gave written informed consent and were informed that additional incisions or open procedure might be warranted during the operation. The study protocol was approved by the Institutional Review Board of our hospital and was conducted in compliance with the Declaration of Helsinki.
The data collected from the two groups included the patients' demographics, operative time, estimated blood loss, transfusion requirements, perioperative and postoperative complications, time to liquid intake, length of hospital stay, postoperative visual analogue scale (VAS) on day 1, and analgesic use. The operative time was defined as the interval between the start of the skin incision and skin closure. The VAS ranges from 0 (no pain) to 10 (worst pain imaginable). The analgesic use from the recovery room to the moment of discharge was converted to morphine equivalents.
Statistical analysis was performed using the calculating program SPSS (version 16.0; SPSS, Inc., Chicago, IL) for Windows. Continuous variables were presented as mean ± standard deviation, and differences between group data were analyzed by the independent samples t-test. The categorical data were compared using Pearson's χ2 test, and Fisher's exact test was used when appropriate. Differences with P values <.05 were considered significant.
Surgical technique
Operation was performed under general anesthesia, and the patient was placed in the full flank position. Pressure points were fully padded. The table was flexed, and the patient was secured with adhesive tape. To perform the conventional LRN, we usually used three trocars (one 10 mm for the camera and the other two of 11 and 5 mm to insert the instruments). The only difference with LESI-RN is that in these cases, we reduced the number of incisions from three to one.
A 5-cm arc skin incision was performed at the midpoint between the costal arch and iliac crest on the midaxillary line (Fig. 1A). Subcutaneous fat was dissected, and the fascia layer was kept integrated. Then, the fascia and underlying musculature at the middle of the arc incision were spared by blunt splitting, and the thoracolumbar fascia was next exposed and penetrated for entrance to the retroperitoneum. The retroperitoneal space was initially developed using blunt finger dissection to push the peritoneum forward. An artificial gasbag was placed into the space with air inflation of 800 mL. The inflation was maintained for 5 minutes.
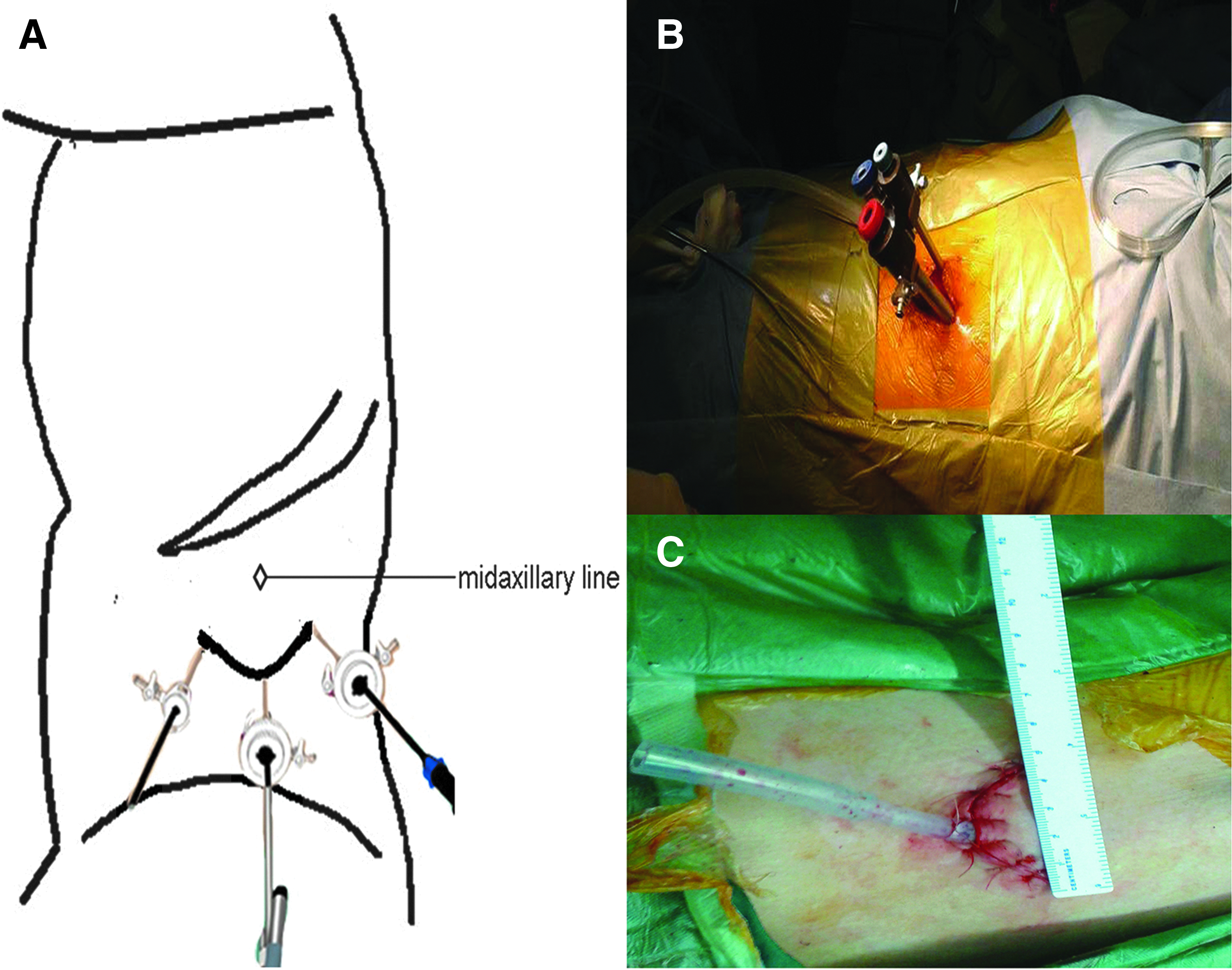
The balloon was subsequently deflated, and a 10-mm trocar was placed into the retroperitoneal space. Trocars of 5 and 11 mm were placed at the left and right ends of the arc incision, respectively (Fig. 1B). All trocars were secured by stay sutures. After insufflation of the retroperitoneal cavity with CO2 at 12–14 mm Hg, a 30-degree straight laparoscope was inserted through the 10-mm trocar at the middle of the arc incision for monitoring. The standard straight graspers were then inserted under direct visualization to perform the procedures. The subsequent operation steps are the same for both approaches.
The posterior surface of Gerota's fascia was sharply opened close to the psoas muscle to expose the fatty tissue harboring renal vessels. The procedure to locate the renal hilum was performed according to those described by Shi et al. 18 The arcuate ligament on the upper surface of psoas muscle can be taken as reference anatomic landmarks. Generally, the arcuate ligament at the boundary between the diaphragm and the psoas muscle is transversely close to the renal hilum. The renal artery and vein were individually divided after placement of the Hem-o-lok clips. Adrenalectomy was not performed routinely for T1 tumors, and there was no sign of adrenal gland involvement. The kidney was circumferentially mobilized, and the ureter was clipped and divided. After the kidney was completely detached from its surrounding tissues, the underlying musculature was spared, and the specimen was retrieved through the arc incision. Incision may be extended according to the size of the specimen. A drain tube was left in situ through the incision, and the incision was carefully sutured (Fig. 1C).
Results
A total of 40 patients had successfully undergone laparoscopic nephrectomy, of which half of the patients had undergone LESI-RN and the other patients had undergone conventional LRN. There was no conversion to open surgery, and no intraoperative complications occurred in either group. All the patients in the LESI-RN group were satisfied with their incisions. The patients in the two groups had comparable demographics with respect to age, gender, BMI, tumor size, tumor laterality, and RNS complexity (Table 1).
Data presented as mean ± standard deviation or n (%).
BMI, body mass index; LESI-RN, retroperitoneal laparoendoscopic single-incision radical nephrectomy; LRN, laparoscopic radical nephrectomy; RNS, R.E.N.A.L. nephrometry score.
The LESI-RN patients had a significantly longer operative time than the conventional LRN group (P = .001). The estimated blood loss in the LESI-RN group was higher than that in the conventional LRN group, but the difference had no statistical significance (P > .05). No patients needed transfusion in both groups. The two procedures were essentially similar in terms of the time to liquid intake (P = .531) and hospital stay after operation (P = .397). No postoperative complications occurred in the LESI-RN group. There was one case of subcutaneous emphysema that occurred in the conventional LRN group. The LESI-RN patients had a significantly lower VAS and analgesic requirement than the LRN group (P < .05). The histopathological evaluation showed complete excision of all specimens. All the postoperative pathological results demonstrated renal clear-cell carcinomas, and tumor stage had no significant difference between the two groups (P > .05) (Table 2). No positive surgical margins were observed in all the patients. The median follow-up was 11.0 ± 7.2 months in the LESI-RN group and 12.3 ± 5.8 months in the conventional LRN group. All patients were alive and free of tumor recurrence.
Data presented as mean ± standard deviation or n (%).
NA, not applicable; VAS, visual analogue scale.
Discussion
With the development of the surgical instruments and technological innovations, a rising demand for less invasive procedures from patients has led to an increased interest in the LESS technique. 19 LESS surgery has the advantages of decreased number of incisions needed and potentially good cosmetic results. 20 However, the procedure often needs some special commercial LESS platforms and instruments, which are not only expensive but also not generally available in some undeveloped area. Although there are some reports about the application of homemade LESS platforms,7,8,18 it still needs some time to construct the device. In addition, there have been some risks of the homemade platforms, such as the glove tear and gas leaking.18,21
Raman et al. 11 first described single-incision LESS nephrectomy using three adjacent trocars through one umbilical incision without special platforms. To minimize the instrument clashing and construct the working triangulation, articulating laparoscopic grasper and deflectable tip video laparoscope were used in their study. Nagele et al. 12 made some innovation on the basis of this technique. In their procedure, three trocars were placed through one three-fourth umbilical incision in the umbilical fold without any platforms. A 5-mm trocar cranially and an 11-mm trocar caudally were placed at a distance of 6–10 cm. A 5-mm camera trocar was placed in-between. Triangulation was achieved by the placement of the trocars, and procedures were performed with conventional instruments. We learned from their experience to perform retroperitoneal LESS nephrectomy.
In our study, we used an arc incision, and three trocars were placed separately to construct the working triangulation ergonomics. The retroperitoneal space is smaller than the transperitoneal space, which has limited the scope of its application and especially brought difficulties to the LESS operation. However, the distance from the trocar to the kidney is shorter in the retroperitoneal approach. With the placement of the trocars to construct the working triangulation, the procedure can be carried out without any extra prebent or articulating instruments. Moreover, after the subcutaneous fat was dissected, the fascia layer and underlying musculature were kept integrated to prevent leakage, except three channels for the trocars. The space between the instruments comprises soft subcutaneous tissue, which allowed for a wider range of motion for the instruments and was conducive to surgery.
It is helpful for improving dexterity and shortening the learning curve for laparoscopic surgeons, especially for those who are familiar with conventional retroperitoneal LRN. In our study, all the patients in the LESI-RN group had successfully undergone the procedure, and there was no conversion to open surgery or conventional LRN. The mean operation time was 149.0 ± 32.5 minutes, which was significantly longer than the conventional LRN group but was similar with Chueh et al. (153.8 ± 35.0 minutes). 13 Dong et al. 2 had described a comparable operative time for the LESS retroperitoneal nephrectomy and conventional LRN (120 minutes versus 120 minutes), demonstrating that average operation time is expected to decrease with increasing cases and experience.
Although the retroperitoneum has a smaller working space and less evident anatomic landmarks, it is exceedingly familiar to the general urologist due to the preponderance of genitourinary organs located therein. In addition, the retroperitoneal approach can provide more direct access to the kidney and less need for visceral retraction or bowel manipulation. 22 In the procedure of the retroperitoneal laparoscopic operation, retroperitoneal balloon dilation is necessary. Sufficient balloon dilation will provide a good working space and make later manipulation easier. In addition, according to the description of Dong et al., 2 there are some important landmarks in the retroperitoneum. The arcuate ligament on the upper surface of psoas muscle often indicates that the operation is near the renal hilum because this ligament extends transversely toward the renal hilum. Using this landmark in our cases, we found it is helpful to identify the renal hilum.
In the present study, it was observed that the LESI-RN group associated with lower VAS and analgesic requirement than the conventional LRN group. The results were similar to other published studies of LESS nephrectomy.4,23,24 For LRN patients, a corresponding incision is needed for removing the specimen. In our study, we used the single operation incision as the surgical manipulation channel for removal of the specimen, which avoided the other two incisions, required in the conventional LRN surgery and achieved the effect of reducing surgical trauma and scars. Decreased number of incisions is helpful to cause low levels of postoperative pain. Conventional equipment and devices were used in this procedure, which is more cost effective for the patients and suitable for the undeveloped area. The time to liquid intake, hospital stay, and follow-up results in the LESI-RN group were similar to the conventional LRN group, and no complications occurred in the LESI-RN group, which indicated that the LESI-RN was a safe and feasible method for selected RCC patients.
Patient selection may be an important consideration in LESS surgery. Mir et al. 25 reported that the younger and thinner patients with nononcological indications or smaller tumors are prime candidates for LESS nephrectomy. The challenge of LESS surgery is greatly amplified in obese patients due to the specimen weight, abdominal wall restrictions, and the distance from the skin to the organ. We would not recommend obese patients as the primary choice for our technique. In addition, we did not choose the large renal carcinoma patients in our preliminary attempts at LESI-RN surgery because we considered oncological clearance to be of utmost importance among those patients. Moreover, the removal of renal tumors that are too large would necessitate larger incisions, which would negate the advantages of LESS surgery.
Interestingly, some reports had found that the younger patients would place greater emphasis on cosmetic outcomes, while the elderly patients often expressed negligible attention to the cosmetic influence of the skin scar.25,26 Thus, the importance of cosmetic satisfaction varies greatly between patients, and it should be taken into consideration when choosing the LESS surgery.
There were some limitations in our study. First, the nature of a retrospective study made it impossible to avoid the selection bias and attrition bias. Second, the sample size of this study was small, and it is a single institution survey. Even though we obtained statistically significant data, the results may be difficult to make clinically significant conclusions. Additionally, although all the patients in the LESI-RN group expressed that they were satisfied with their surgical scars, there is an absence of a valid questionnaire when we assessed the cosmetic results of the scars. We will adopt a valid questionnaire to evaluate the effects of surgical approach on cosmesis for later patients.
In conclusion, the results of this study demonstrate that LESI-RN is a safe and feasible surgical strategy with favorable perioperative outcomes, which results in significantly improved control of postoperative pain and cosmetic results. It combines the common principles of using straight instruments and working triangulation in conventional LRN with advantages of cosmesis and minimal invasiveness in LESS surgery, which may be helpful to novice LESS surgeons, especially for those who are familiar with conventional retroperitoneal LRN. No special equipments and devices were used in this procedure, which indicates that LESI-RN is more cost effective. The mean operation time is expected to decrease with increasing experiences. However, additional research, including randomized and prospective trials with a larger sample size, will be needed to draw solid conclusions regarding the relative efficacy of this procedure compared with conventional retroperitoneal LRN approaches.
Footnotes
Acknowledgment
The authors would like to thank Todd Hubbard for the language review.
Disclosure Statement
No competing financial interests exist.