
Abstract
Abstract
Background:
Fish bone migration from the gastrointestinal tract into the liver is an unusual cause of liver abscess.
Materials and Methods:
We describe successful laparoscopic removal of intrahepatic fish bones in 2 patients who presented with liver abscesses. Both patients were admitted to our institution with a 2-week history of right upper quadrant pain, fever, chills, and rigors. Radiological imaging revealed the presence of a linear calcified foreign body within a hepatic abscess in the left lateral section of the liver. These findings were suggestive of infection secondary to migration of fish bone from the stomach to the liver.
Results:
Both patients underwent percutaneous drainage of liver abscesses with control of sepsis, followed by laparoscopic removal of intrahepatic fish bones. Localization of the fish bones was facilitated by intraoperative ultrasonographic examination of the liver. Postoperative recovery was fast and uneventful.
Conclusions:
This is the first report of two consecutive cases of liver abscess caused by fish bone migration where our patients were successfully treated by percutaneous drainage of the abscess followed by laparoscopic removal of intrahepatic fish bone.
Introduction
U
Case Reports (Methods and Results)
Clinical presentation
Our patients' demographics, clinical presentation, and laboratory results were similar (Table 1).
Radiological findings and clinical management
Ultrasonography (US) and computed tomography (CT) of the abdomen was performed for both patients.
Patient A's US study showed a heterogeneously hypoechoic lesion in the left lobe (segment II/III) of the liver (Fig. 1). Contrast-enhanced CT of the abdomen revealed a 3.8- × 3.8- × 3.7-cm irregularly shaped hypodense lesion in the left lobe containing a linear hyperdensity, with a faint soft tissue tract extending from the lesion to wall of the gastric antrum. This was consistent with a liver abscess containing a foreign body that likely migrated from the antrum.
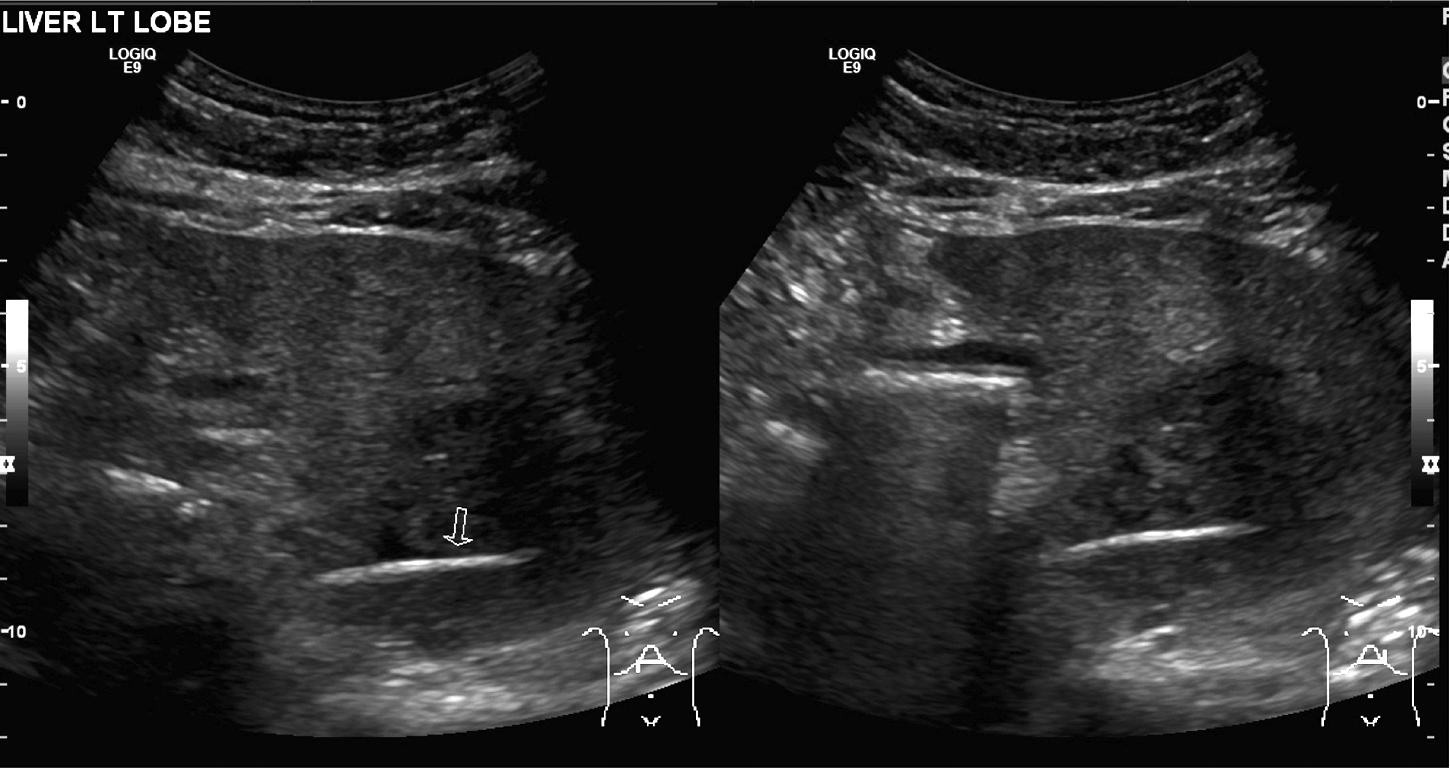
Ultrasound study of Patient A showing a linear hyperechoic foreign body within the liver parenchyma.
Patient B had a large, irregular, ill-defined mass of mixed echogenicity in the left lobe of the liver demonstrated on US. Contrast-enhanced CT of the abdomen revealed a large 9.0- × 9.0-cm multiloculated abscess containing a linear density closely related to the lesser curve of the stomach with surrounding fat stranding (Figs. 2–4). This was again consistent with a liver abscess containing a foreign body that likely migrated from the stomach.
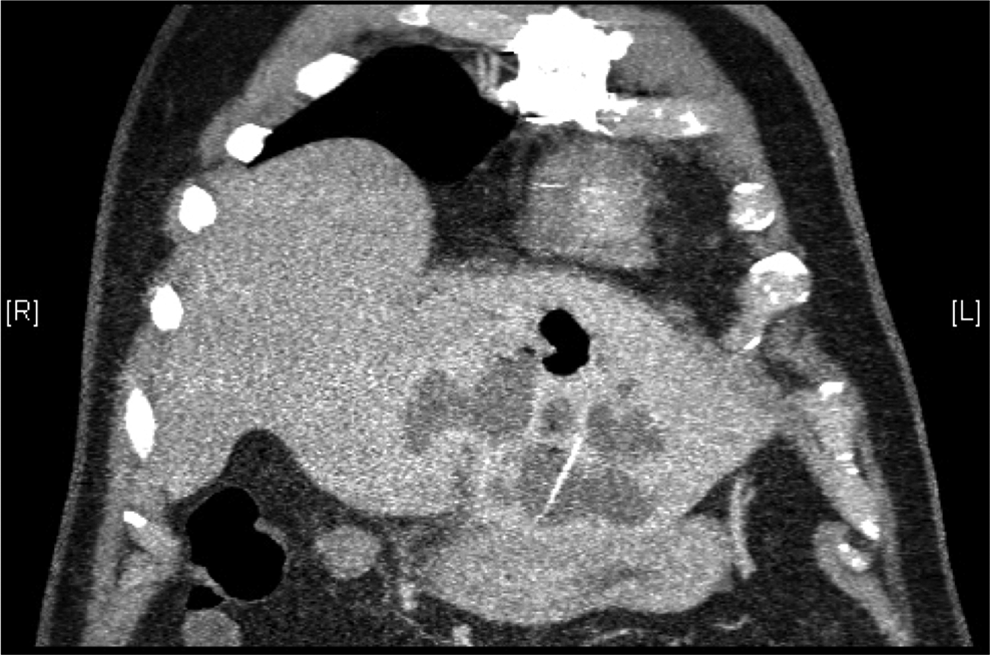
Coronal computed tomography scan of Patient B showing a linear calcified body with an abscess cavity within the liver parenchyma.
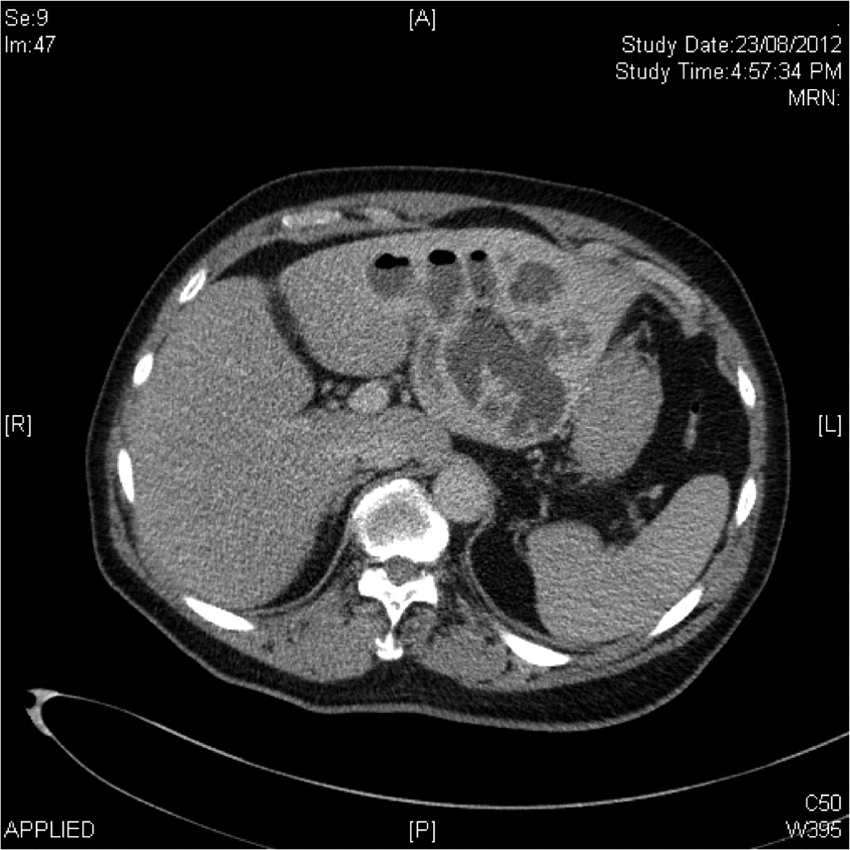
Axial computed tomography scan of Patient B showing a large abscess cavity within the liver parenchyma.

Sagittal computed tomography scan of Patient B showing a linear calcified body with an abscess cavity within the liver parenchyma.
Both patients were treated with intravenous antibiotics and percutaneous drainage of the liver abscess. Abscess cultures grew Klebsiella pneumoniae. Repeat imaging 3 weeks later showed marked improvement in the size of the abscesses, and the patients underwent operative intervention for removal of the foreign body.
Surgical technique
Each patient was placed under general anesthesia in a supine position. Pneumoperitoneum was achieved with an open technique via a 12-mm supraumbilical port. Two 5-mm trocars were inserted in the left upper quadrant and epigastrium, respectively. An exploration of the abdomen was performed: Patient A had an omental attachment to the inferior surface of the left lateral segment of the liver, whereas we encountered dense adhesions between the anterior antrum wall and the left lateral segment in Patient B.
The omental adhesion to Patient's A left lateral segment was taken down, and an intraoperative US scan was used to trace the position of the foreign body. The entry site of the foreign body was located, and a tiny tip of the object was noted protruding from the liver's surface. The tip was grasped, and the entire length of the foreign body was easily removed. There was a small, scarred prepyloric area in the stomach indicating the possible site of penetration.
US examination of Patient's B liver determined that the foreign body had impacted itself into the liver just left lateral to the falciform ligament. An intraoperative ultrasonogram confirmed the location of the fish bone. After careful adhesiolysis of the dense adhesions between the gastric pylorus and the antrum, the very tip of the fish bone was found and completely retrieved.
The postoperative recovery for both patients was uneventful.
Discussion
Although ingested foreign bodies are a common clinical problem, they are a rare cause of gastrointestinal (GI) perforation because most foreign bodies (80%–90%) pass through the GI tract uneventfully.2,3 Perforations tend to be caused by thin, sharp foreign bodies such as fish bones, chicken bones, toothpicks, and needles. Common sites of perforation include the pylorus, the duodenojejunal flexure, the terminal ileum, and the cecum. Perforation of the foreign body through the stomach into the liver, as detailed in our report, is extremely uncommon. About 10%–20% of foreign bodies will require endoscopic removal, whereas surgery is only necessary in 1% of cases. 3
Patients present with a wide variety of symptoms such as abdominal pain, tenderness, and fever. History of consumption of the foreign body is commonly obtained retrospectively. The diagnosis of a GI tract perforation secondary to an ingested foreign body may be difficult and require the use of multiple imaging modalities. 4 Plain radiographs can detect radio-opaque foreign bodies and confirm the location, progress, size, shape, and number of ingested objects. 5 Classic indicators of a perforated GI tract such as free air on abdominal x-ray may not be present.
CT has a higher sensitivity compared with plain radiographs for the detection of foreign bodies, particularly for objects that are faintly radio-opaque. 6 A high index of suspicion for a foreign body perforation is indicated if an abscess is seen on CT adjacent to or in continuity with parts of the GI tract, for example, an abscess in the left lateral segment of the liver. Presence of gas locules within the abscess, although unreliable, may also indicate the presence of a foreign body within the liver abscess. 7
Subsequent infection and abscess formation of the adjacent organ can contribute to the difficulties in making a diagnosis of a perforated GI tract secondary to an ingested foreign body. In some reports, no foreign body was found during preoperative imaging, although a foreign body was retrieved intraoperatively. 8 In other cases, further investigations such as colonoscopy were used in making the diagnosis. 9
Surgical exploration, repair of the perforation, and drainage of infection with removal of the foreign body are the mainstay of management for foreign body perforation of the GI tract (Fig. 5). Hepatic abscesses secondary to foreign body perforation of the GI tract usually require drainage of the abscess and surgical removal of the causative object, although interventional radiological methods may be attempted.10,11 Very few reported cases of hepatic abscess secondary to foreign body perforation have been successfully treated conservatively.
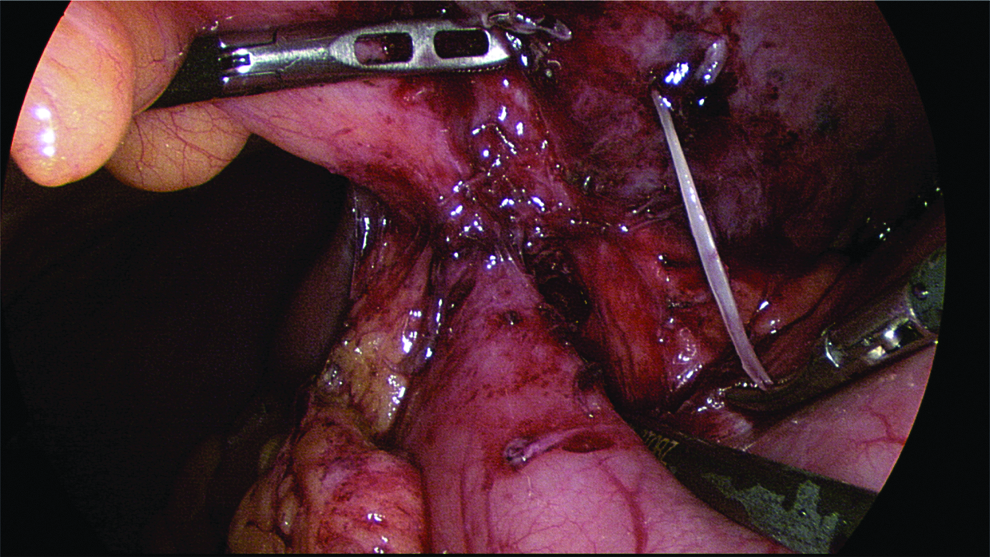
Intraoperative image of Patient A showing the retrieval of the fish bone from the liver parenchyma during laparoscopic surgery.
Because most of the foreign bodies that cause perforation tend to have long and slim profiles (Fig. 6), many of these may be extracted via a small incision (i.e., a laparoscopic port). In cases of fish bone embedded within a liver lobe, removal of the foreign body is facilitated by performing laparoscopic intraoperative US to detect the exact location of the fish bone. The bulk of the literature on the utility of laparoscopic US for liver lesions has been studied in the evaluation of liver metastasis, where sensitivity rates of 80%–100% may be reached. 12 Point-of-care US is commonly used to detect the location of ingested foreign objects in pediatric patients. 13 We used laparoscopic US to direct our dissection to the tip of the fish bone nearest to the surface of the affected liver.

Retrieved fish bone from Patient A.
The outcome of patients with hepatic abscesses secondary to foreign body perforation of the GI tract varies depending on how fast a diagnosis is made. When the diagnosis is not made early, the hepatic abscess may be fatal despite aggressive intervention. The literature reports at least 2 cases in which a fish bone was identified within the hepatic abscess at necropsy.11,14
Conclusions
We report 2 cases of hepatic abscess secondary to foreign body penetration successfully managed with percutaneous drainage prior to laparoscopic removal of the foreign body. In nonseptic patients with this type of liver abscess, conservative management until clinical improvement before undergoing elective laparoscopic removal of the foreign body is a safe and viable option. Localization of the foreign body may be performed with a laparoscopic intraoperative US probe if the site of entry into the hepatic parenchyma is not apparent.
Footnotes
Disclosure Statement
No competing financial interests exist.