
Abstract
Abstract
Objective:
Direct excision of dermoid cysts of the eyebrow and forehead may lead to a prominent facial scar. Endoscopic techniques have greatly reduced the morbidity of excising benign orbitofacial masses. Access, visualization, and dissection of these masses are comparable to open approaches without the use of large or conspicuous incisions. This study evaluates the efficacy of the endoscopic approach in the treatment of dermoid cysts of the eyebrow and defines the place of this approach as an alternative to open surgery.
Materials and Methods:
Between July 2008 and April 2015, a total of 23 pediatric patients (13 females and 10 males) with dermoid cysts of the brow underwent excision by endoscopy. The mean age was 11.9 months (2–32 months). The lesion was located on the lateral brow in 17 cases and on the hairless forehead in 6 cases. To assess osseous involvement, sonography and magnetic resonance imaging study were performed in 22 and 1 case, respectively. Medical photos documentation was done systematically. For those children having an excision of cyst by endoscopy, the operative time, hystopathological examination, specimen size, and hospital stay were evaluated. In addition, parents of these patients were contacted to determine satisfaction with the procedure.
Results:
All procedures were successfully performed endoscopically. The mean operative time was 41 minutes (range 17–120 minutes). There was no intraoperative complication. The mean specimen size was 12 mm. In postoperative period, 1 patient presented edema on the forehead with uneventful course. All procedures were performed on the day-surgery. The hystopathological examinations were dermoid cysts in 21 cases, hemangioma in 1 case, and dermatofibroma in 1 case. The mean follow-up was 45.5 months (4–84 months). There was no residual mass or recurrence after long follow-up. Cosmetic results were excellent and all families were pleased with the outcome.
Conclusions:
Endoscopic excision of forehead masses and dermoid cysts of the eyebrow is safe and it has proven to be an effective and minimally invasive alternative to the conventional approach. The main advantage of this procedure is the minimization of scar visibility compared with open surgery.
Introduction
D
They can also occur adjacent to the nose but are rarely found in association with the bones in the lower part of the eye socket. Rarely, orbital dermoid cysts are found more posteriorly in the eye socket. The cyst cavity typically contains some combination of sebaceous fluid, keratin, calcium, and cholesterol crystals. 1
Rarely, dermoid cysts can cause vision loss in the affected eye, nevertheless it has a tendency to grow and cause an inflammatory reaction and infection. For these reasons, the pediatric ophthalmologist may recommend that the dermoid cyst must be removed.
The treatment of these lesions can be accomplished by an incision directly over the lesion or an upper eyelid. Cosmetic results are not optimal because the skin is thin at this point, so it is difficult to hide the scar.
The first description of endoscopic brow-lift techniques was described by Ramirez in 1995, 2 after that different reports have been described with the use of these advanced techniques for removal of benign lesions on the face.3–17
The objective of this study is to evaluate the efficacy of the endoscopic approach in the treatment of dermoid cysts of the eyebrow and define the place of this approach as an alternative to open surgery.
Materials and Methods
Between July 2008 and April 2015, a retrospective study evaluated a total of 23 pediatric patients (13 females and 10 males) with dermoid cysts of the eyebrow, who underwent excision by endoscopy. The mean age was 11.9 months (2–32 months). The lesion was located on the lateral brow in 17 cases and on the hairless forehead in 6 cases.
To assess osseous involvement, sonography and magnetic resonance imaging study were performed in 22 cases and 1 case, respectively (Fig. 1). In addition, medical photos documentation was done in all patients. For those children having an excision by endoscopy, the operative time, complications, hystopathological examination, specimen size, and hospital stay were determined. To evaluate the cosmetic results, parents of the patients were contacted to determine satisfaction with the long-term outcome.
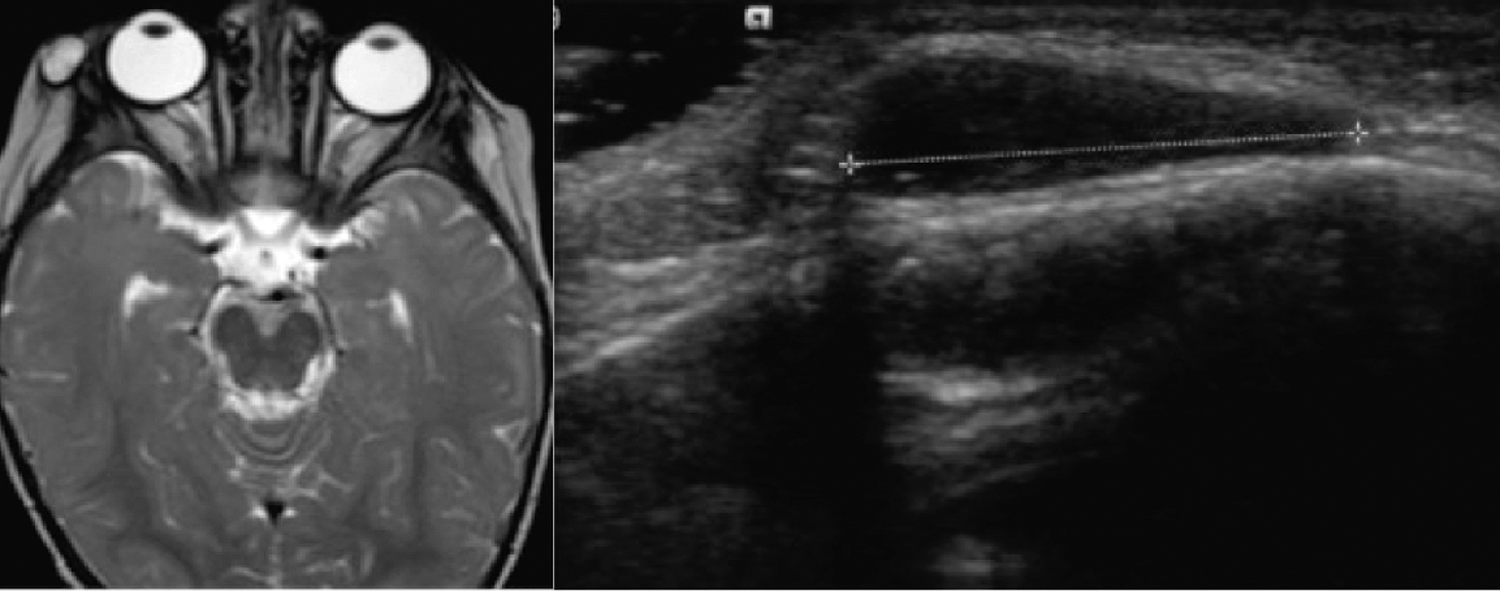
Magnetic resonance imaging and sonography study in a patient with dermoid cyst located on the right side.
Surgical Technique
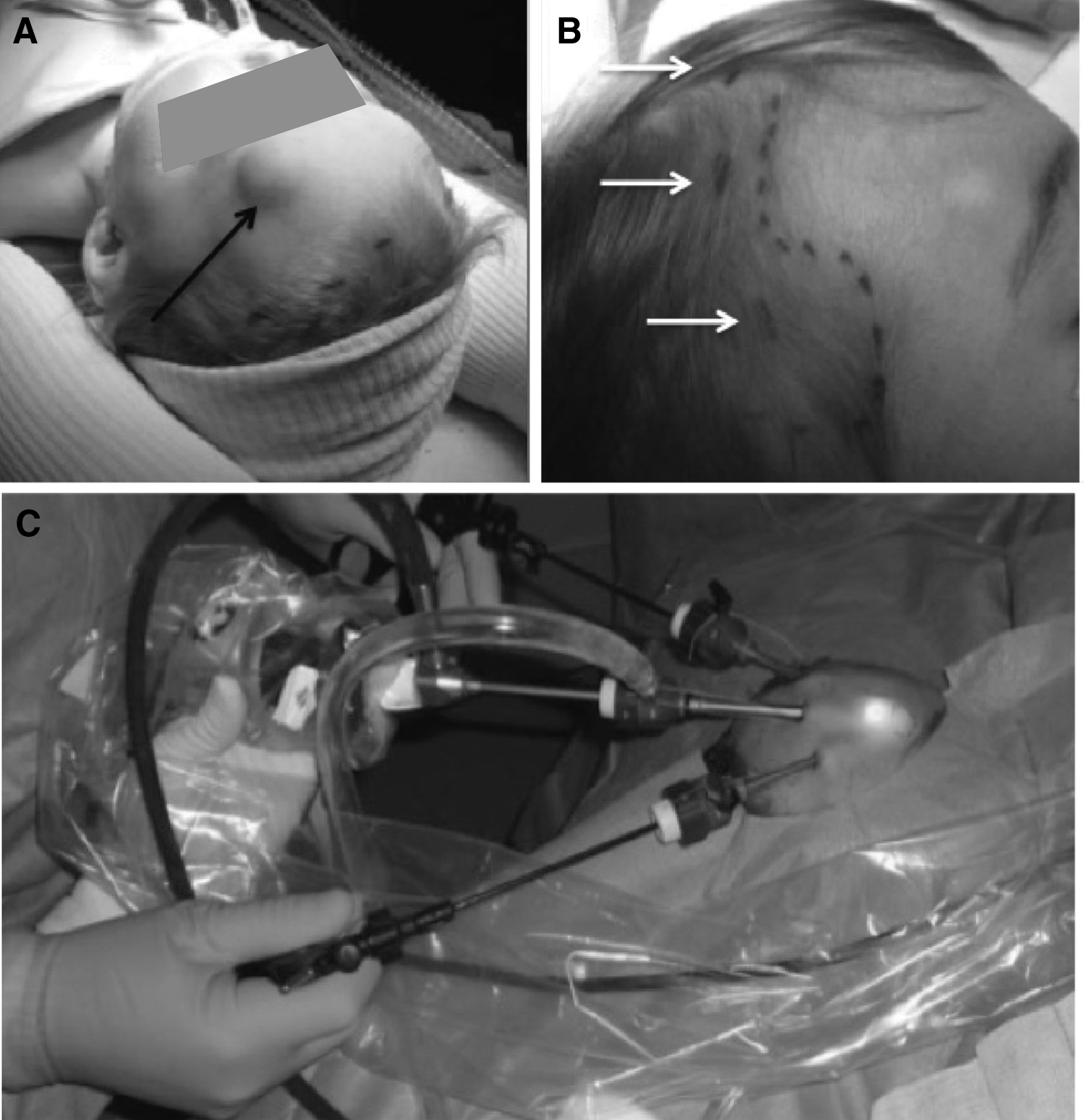
Under general anesthesia, an ipsilateral block was done systematically at the territory of the trigeminal nerve. The patient was placed in decubitus position with the head turned toward a contralateral position to the lesion. The surgeon was positioned at the head of the patient, the assistant to the right, and the screen at end of the table.
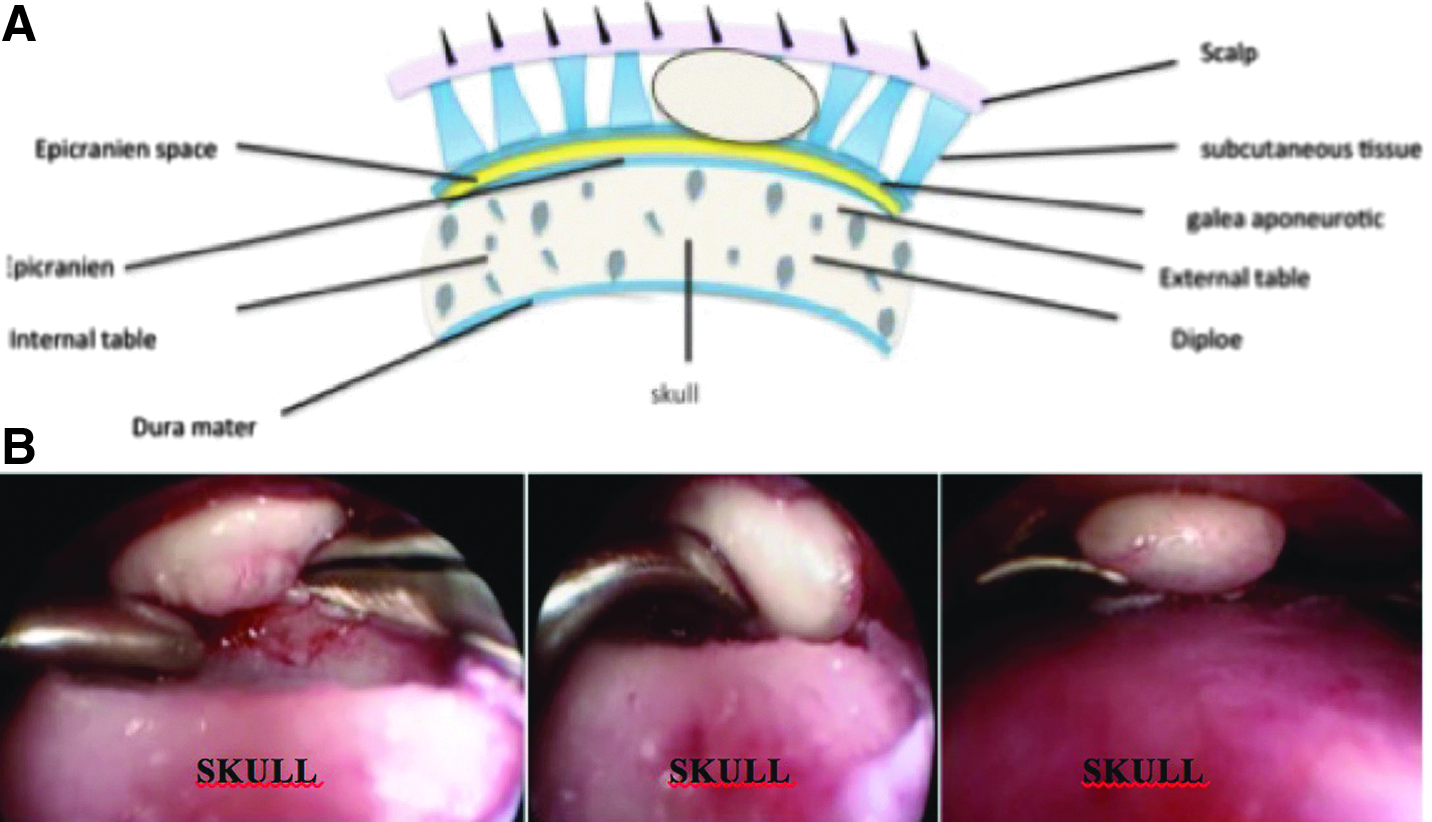
Two or three ports were used in all cases (Fig. 2). The incision was made in the temporal region inside the hairline. The dissection was carried out by blunt dissection through the subgaleal plane with the 5 mm-30° telescope to create a workspace (Fig. 3). An insufflation was done with CO2 at pressure of 4 mmHg. One or two 3 mm instruments were placed in each side. The dissection was generally bloodless; the fingertip palpation on the skin was helpful for localizing the lesion. Once near to the lesion, the dissection was done and involves separating the lesion free from the surrounding tissues. Once removed, the dissection path was irrigated with copious amounts of saline. The skin incision was closed with a fast absorbable braid.
Results
All procedures were successfully performed by endoscopy without rupture. The mean operative time was 41 minutes (17–120 minutes). There was no intraoperative complication. All procedures were performed on the day-surgery. The lesion was predominantly in temporal region. The mean specimen size measurement by sonography was 11.3 mm (8–20 mm). In postoperative period, 1 patient presented edema on the forehead with uneventful course.
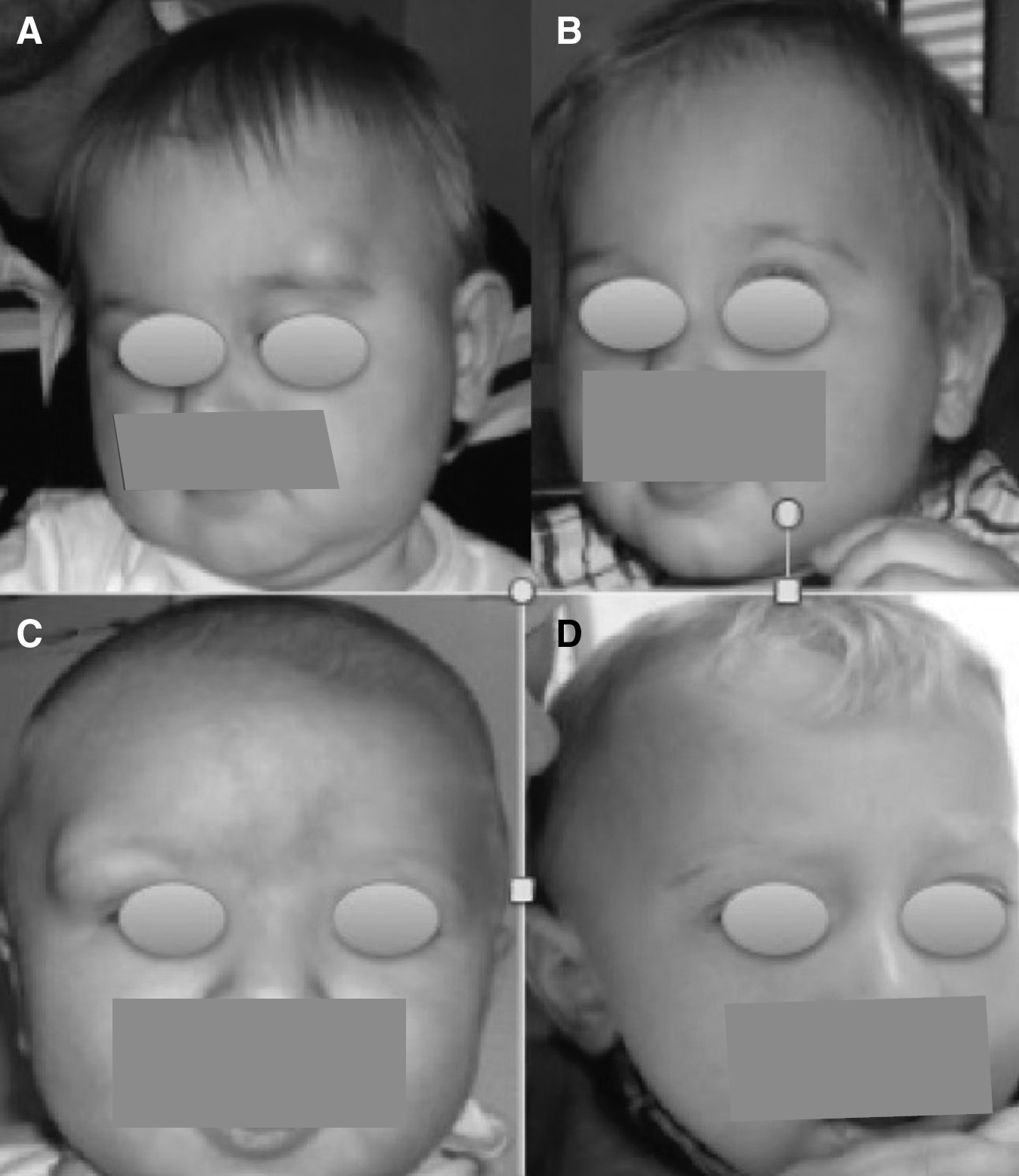
All patients were checked at 2 months postoperatively. No frontal branch paresis or hypoesthesia was noted. The hystopathological examinations were dermoid cysts in 21 cases, hemangioma in 1 case, and dermatofibroma in 1 case. The mean follow-up was 45.5 months (4–84 months). There was no residual mass or recurrence, and cosmetic results were excellent and all families were pleased with the long follow-up outcome (Fig. 4).

Cosmetic results. Same patient.
Discussion
Dermoid cysts in children are one of the most common benign noninflammatory space-occupying orbital lesions and are present in the first few years of life as smooth, well-circumscribed, subcutaneous, painless masses. The most common location is in the external third of the fronto-orbital region near the end of the eyebrow in the pediatric population. 18
Conventionally, these lesions are removed through direct skin incisions over the mass itself. It had a good exposure associated with a low complications rate. Nevertheless, the forehead is a conspicuous part of the face, and any incision in this area inevitably results in visible scars even if the incision is parallel to the facial expression lines. When the incision is made along the eyebrow, discoloration or disrupted hair growth in the scarline may appear, and is bound to leave a scar on the face, which may be cosmetically unacceptable to patients, especially when complicated by hypertrophy or keloid formation.
Another alternative approach to excision of dermoid cysts situated in the lateral third of the brow is to perform by incision through the superior eyelid. This approach has been reported to produce excellent results with low complication rates. 19 Nevertheless Kersten reported a later complication associated with early scar retraction. 20
The endoscopic approach achieves an exposure and access similar to open approach. It provides direct and magnified visualization of the mass, facilitating minimal tissue manipulation, and avoidance of neurovascular injury. An excellent esthetic outcome can also be achieved, with no forehead scarring as a sequela. However, endoscopic surgery on the forehead requires minimal familiarity with the neuronal structures in the region, specifically the temporal branch of the facial nerve, the supratrochlear nerve, and the superficial branch of the supraorbital nerve.
Endoscopic dissection to reach the mass can be either by the subgaleal or subperiosteal plane. It is often dependent on surgeon preference as well as tumor location. Papay et al. propose subperiosteal dissection, even for soft-tissue masses. In our cases the dissection was done through the subgaleal plane, because in this plane the dissection is generally bloodless and offers a more direct approach to soft tissue, thus this approach is easier and faster than the subperiosteal approach (Fig. 3). Dutta et al. reported in 2006 9 consecutive outpatient procedures, all lesions were successfully excised endoscopically without complications. This report shows that endoscopic excision of forehead masses is a safe and efficacious procedure in the hands of pediatric surgeons. No recurrence of dermoid cysts has been reported by this endoscopic approach. 12
We strongly believe that, in the hands of endoscopic surgeons, endoscopic excision of forehead and eyebrow benign tumors by the subcutaneouscopic approach is easy and safe, allowing a safe removal with excellent cosmetic results compared with open surgery (Fig. 5).
Comparison of cosmetic results between open and endoscopic approaches.
Footnotes
Disclosure Statement
No competing financial interests exist.