
Abstract
Abstract
Purpose:
To evaluate the efficacy and safety of bipolar and monopolar transurethral resection of bladder tumor (TURBT) procedures for non-muscle invasive bladder cancer (NMIBC) patients.
Materials and Methods:
We searched for all studies investigating bipolar TURBT and monopolar TURBT for NMIBC patients in PubMed, Web of Knowledge, and the Cochrane Central Search Library. A systematic review and meta-analysis were performed. Efficacy was assessed by catheterization time, resection time, pathology, and recurrence rate. Safety was assessed by obturator nerve reflex, bladder perforation, hemoglobin decrease, and transfusion.
Results:
Our searches identified eight studies. Bipolar TURBT is associated with decreased resection time, catheterization time, and hemoglobin changes. There were no statistically significant differences between bipolar TURBT and monopolar TURBT for rates of obturator nerve reflex, bladder perforation, and transfusion. The grade of cautery artifact had no different between the two procedures or even was lower in the bipolar arm. There was no significant difference in recurrence rate when comparing the two procedures.
Conclusions:
This systematic review indicates that the bipolar technique is more efficacious and safer for NMIBC patients. More large-scale, multicenter, randomized controlled studies are needed before final clinical recommendations can be made.
Introduction
B
Materials and Methods
In accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, 14 a systematic review of the literature was performed in May 2015 using PubMed, Web of Knowledge, and the Cochrane Central Search Library. Search terms used included “bladder cancer,” “bladder neoplasms,” “bladder,” “transurethral resection of bladder tumors,” “monopolar,” and “bipolar.” Additional studies were identified by manual search from the references of original studies or review articles on this topic. Full texts or abstracts of all related reports were then reviewed. The literature retrieval was performed by three independent reviewers.
The following criteria were used for study selection: (1) RCT, case-control study (CCS), and cohort study were included, (2) patients diagnosed with NMIBC, and (3) treatment intervention (monopolar TURBT versus bipolar TURBT). Studies with overlapping or insufficient data were excluded. Articles published in English were included in the search.
Two investigators independently assessed and extracted the data into a standardized data extraction form from each publication. Disagreements were resolved by a third author. The outcomes include efficacy and safety. Efficacy was assessed by catheterization time, resection time, pathology, and recurrence rate. Safety was assessed by obturator nerve reflex, bladder perforation, hemoglobin decrease, and transfusion.
The quality of RCT studies was assessed with the Jadad scale. 15 The non-RCT studies were assessed with a modification of the Newcastle–Ottawa Scale 16 : scores of 5–9 were defined as high quality, with a score of <5 as low quality. The trial data were processed as described in the Cochrane Reviewers' handbook. If the study did not provide the standard deviations, we calculated it based on the data extracted from confidence intervals (CIs) or P values. The statistical package (RevMan version 5.0) provided by the Cochrane Collaboration was used. Dichotomous data were presented as odds ratio (OR), and continuous outcomes were given as mean difference (MD), both with 95% CIs. If heterogeneity was reported as P > .10 and I2 ≤50%, heterogeneity was classified as low. The random-effects model was used when there was heterogeneity among the trials. Otherwise, the fixed-effects model was used.
Results
Study characteristics
Ninety-one studies were identified from the electronic database and hand search. We excluded 83 articles, resulting in 8 articles for analysis.8–13,17,18 These studies included three RCTs, four CCSs, and one cohort study that met our inclusion criteria (Fig. 1). The characteristics of the included trials are described in Table 1.
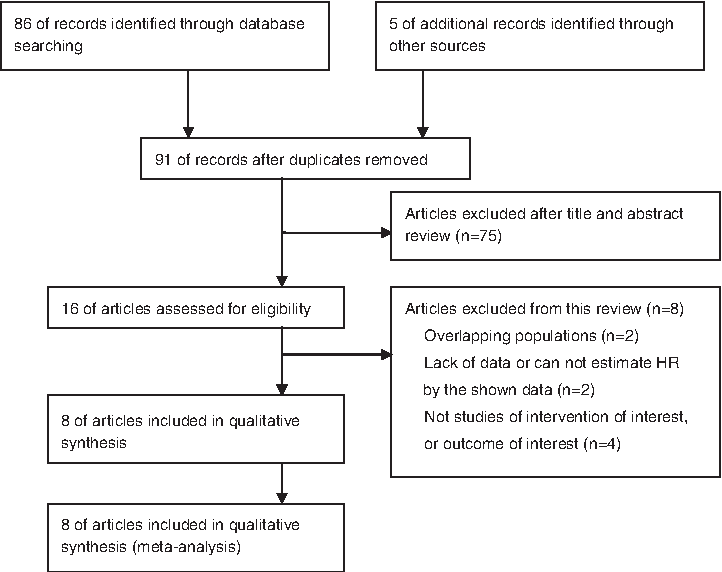
Flowchart of article selection. HR, hazard ratio.
Newcastle–Ottawa Scale score.
Jadad scale score.
CCS, case-control study; RCT, randomized controlled trial; NR, not reported; PK, plasma kinetic technology; TURis, transurethral resection in saline.
Efficacy
Resection time
Three studies reported resection time. There was no statistical heterogeneity among the trials (P = .36; I2 = 3%). Pooled analysis revealed a shorter resection time for bipolar TURBT compared with monopolar TURBT (fixed-effect model: MD = −1.79; 95% CI, −3.52 to −0.07; P = .04) (Fig. 2).

Forest plots of resection time. CI, confidence interval; IV, inverse variance; SD, standard deviation.
Catheterization time
Four studies reported catheterization time. There was no statistical heterogeneity among the trials (P = .28; I2 = 22%). Pooled analysis revealed a shorter catheterization time for bipolar TURBT compared with monopolar TURBT (fixed-effect model: MD = −0.83; 95% CI, −1.03 to −0.63; P < .0001) (Fig. 3).
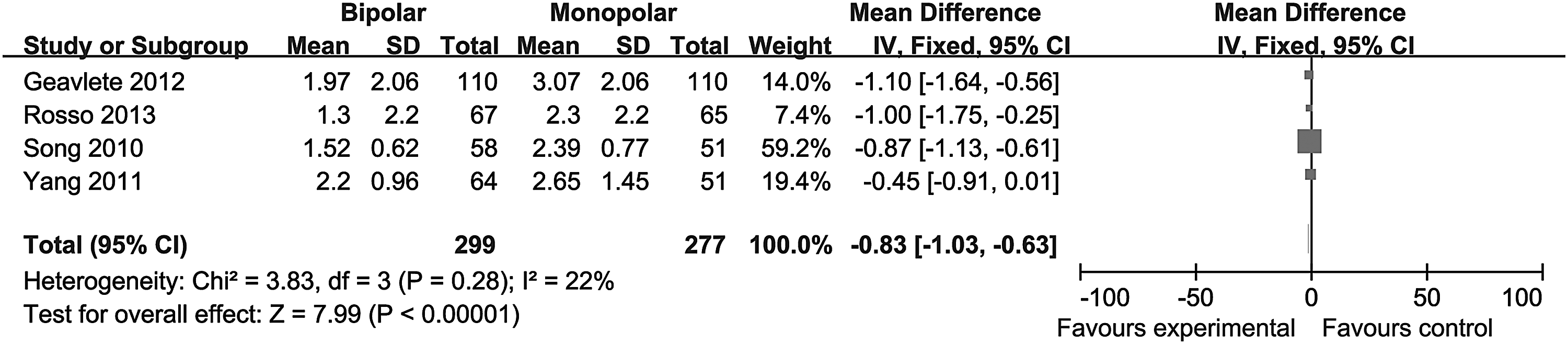
Forest plots of catheterization time. CI, confidence interval; IV, inverse variance; SD, standard deviation.
Pathologic outcomes
Five studies reported pathologic outcomes. Because of the different evaluation measures of pathologic outcomes in each study, meta-analysis could not be performed. Table 2 shows that the grade of cautery artifact has no different between the two groups or even was lower in the bipolar arm.
Grade 1 for a given case was defined as cautery artifacts involving less than one-third of the entire specimen. Tissue chips with one-third to two-thirds cautery artifacts were categorized as Grade 2. Tissue chips with over two-thirds cautery artifacts were categorized as Grade 3.
Severe artifact was defined as more than 50% cautery artifact in most chips.
TURBT, transurethral resection of bladder tumor.
Recurrence rate
Three studies reported recurrence rate. Because of the different follow-up or evaluation measures of recurrence rate in each study, meta-analysis could not be performed. All the three studies showed there were no significant differences in recurrence rate comparing the two procedures (Table 3).
The 2-year recurrence-free survival rates.
TURBT, transurethral resection of bladder tumor.
Safety
Obturator nerve reflex
Four studies reported obturator nerve reflex. Heterogeneity was detected among the trials (P = .002, I2 = 79%). There were no statistically significant differences in obturator nerve reflex between bipolar TURBT and monopolar TURBT (random-effect model: OR = 0.35; 95% CI, 0.06–1.95; P = .23) (Fig. 4).
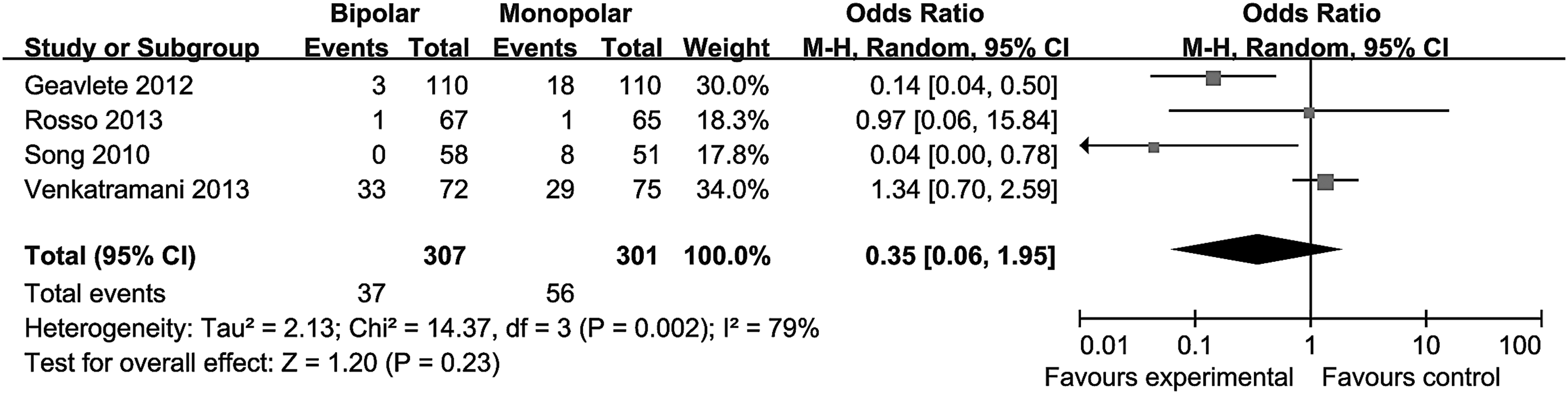
Forest plots of obturator nerve reflex. CI, confidence interval; M-H, Mantel–Haenszel test.
Bladder perforation
Five studies reported bladder perforation. There was no statistical heterogeneity among the trials (P = .12; I2 = 49%). Pooled analysis revealed no differences between bipolar TURBT and monopolar TURBT on bladder perforation (fixed-effect model: OR = 0.51; 95% CI, 0.25–1.01; P = .05) (Fig. 5).
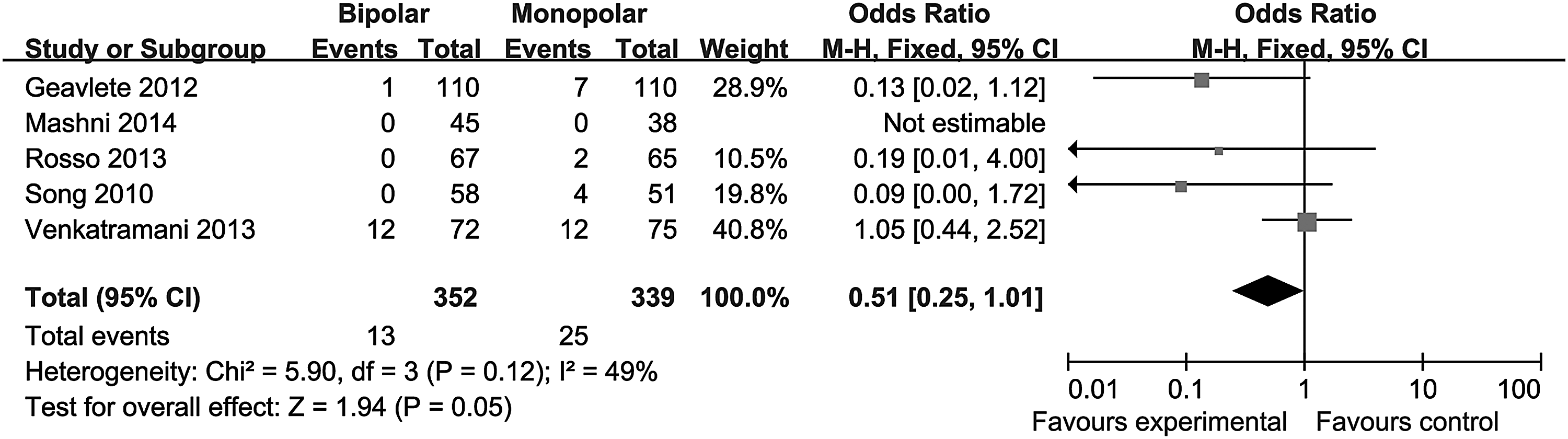
Forest plots of bladder perforation.
Hemoglobin decrease
Three studies reported hemoglobin decrease. There was no statistical heterogeneity among the trials (P = .49; I2 = 0%). Bipolar TURBT showed a beneficial effect on hemoglobin decrease compared with monopolar TURBT (fixed-effect model: MD = –0.57; 95% CI, −0.83 to –0.31; P < .0001) (Fig. 6).

Forest plots of hemoglobin decrease. SD, standard deviation.
Transfusion
Seven studies reported transfusion data. There was no statistical heterogeneity among the trials (P = .28; I2 = 23%). Pooled analysis revealed no differences between bipolar TURBT and monopolar TURBT on transfusion (fixed-effect model: OR = 1.02; 95% CI, 0.75–1.40; P = .88) (Fig. 7).
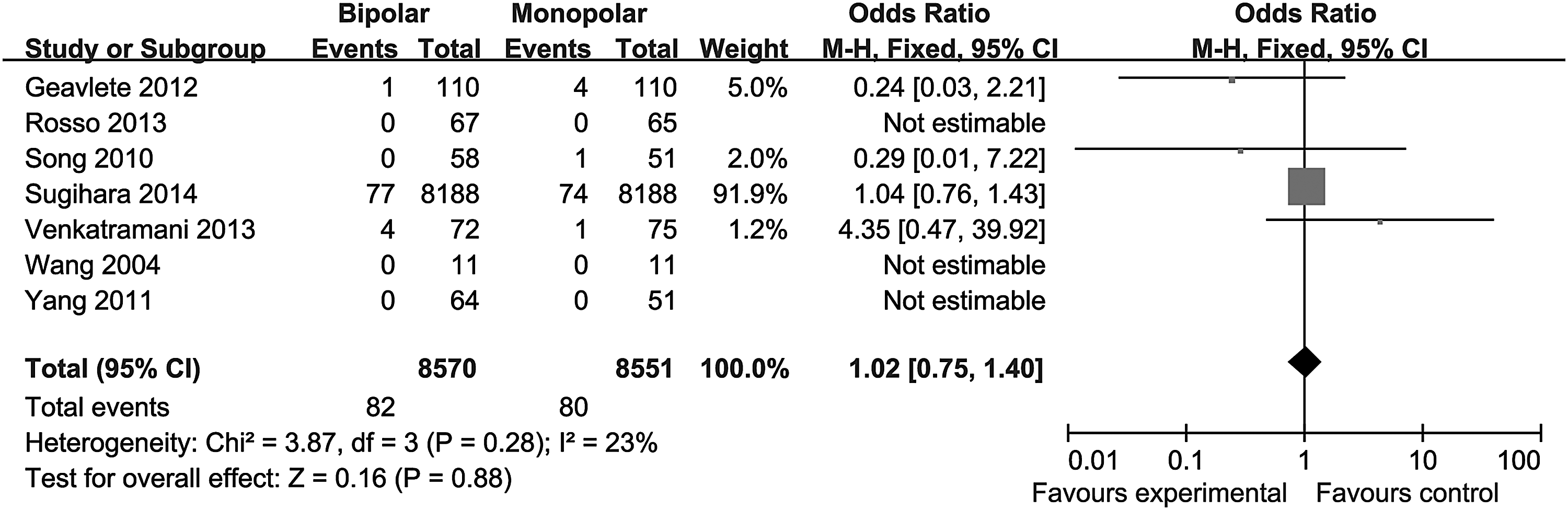
Forest plots of transfusion.
Discussion
With the development of bipolar resection techniques, more alternatives are available to substitute for the conventional transurethral monopolar resection of NMIBC. 7 In bipolar technology the positive and negative poles are isolated from each other by a ceramic connecting piece. The absence of a return current can coagulate small venous bleeding and minimize bleeding during the procedure, thereby providing a clearer view during surgery and a lower incidence of early complications compared with monopolar TURBT.
Our pooled analysis for resection time, catheterization time, and hemoglobin decrease had revealed that bipolar TURBT was associated with significant beneficial outcomes compared with monopolar TURBT. Bladder perforation is a frequently encountered complication, especially for tumors located on the lateral wall. 19 Most of these events occur after obturator nerve stimulation during the standard monopolar resection. In our pooled analysis there were no statistically significant differences between bipolar TURBT and monopolar TURBT for rates of obturator nerve reflex and bladder perforation. Different power settings in each study may explain the statistical heterogeneity in pooled obturator nerve reflex data. Gupta et al. 20 suggested that reducing the power settings to 50 W cutting and 40 W coagulation reduces the risk of obturator reflex and bladder perforation close to zero while maintaining its efficacy. In monopolar systems electrical energy is applied directly to the tissue, where its electrical resistance creates temperatures up to 400°C, which leads to tissue desiccation and penetrative tissue damage. Bipolar systems direct the radiofrequency current from an active electrode to an adjacent return electrode; this technique allows the thermal effect to occur at a much lower temperature.21–23 The ability of the pathologist to make an accurate diagnosis may be impaired by cautery artifacts. In our analysis the grade of cautery artifact was not different between the two procedures or even was lower in the bipolar arm. There were no significant differences in recurrence rate comparing the two procedures.
Sugihara et al. 12 compared the total costs of the two procedures. Compared with monopolar transurethral bladder tumor resection, bipolar resection was associated with slightly lower total costs (mean, $4628 versus $4727; difference = –1.1%; all P < .05).
Several limitations should be noted in our study. One limitation of our findings is some variables, such as local culture, the skill and experience of the operating surgeon, efficacy of perioperative care, and tumor size and number, have differed between the two groups. Some studies in our analysis used plasma technology, whereas the others used transurethral resection in saline technology. These variables may lead to biases. Further high-quality, large-scale, multicenter RCTs should be performed with consideration of these differences between the two groups. Second, four of the eight studies were not RCTs, a finding that raises inherent differences with selection, measurement, and attrition biases. Third, a small sample size study with only 11 cases in each group included in our analysis was also a limitation. However, we also included a large sample size, retrospective study with more than 1000 cases. Fourth, several standard devations were calculated based on the data extracted from the CIs for group means or P values, and this may yield errors, although tiny. Lastly, restriction of the literature search to the English language may result in missing eligible studies published in other languages.
Conclusions
The bipolar technique is more efficacious and safer than the monopolar version for NMIBC patients. Bipolar TURBT is associated with decreased resection time, catheterization time, and hemoglobin changes. There were no statistically significant differences between bipolar TURBT and monopolar TURBT for obturator nerve reflex, bladder perforation, and transfusion. The grade of cautery artifact was not different between the two procedures or even was lower in the bipolar arm. There were no significant differences in recurrence rate comparing the two procedures. More large-scale, multicenter, randomized controlled studies are needed before final clinical recommendations can be made.
Footnotes
Acknowledgments
This work is supported by the Fundamental Research Funds for the Central Universities of Central South University (grant 2015zzts109).
Disclosure Statement
No competing financial interests exist.