
Abstract
Abstract
Gastroesophageal reflux disease (GERD) is a common disorder that can cause a variety of typical and atypical symptoms. Although most patients can be rendered asymptomatic with medical treatment, some experience persistent breakthrough symptoms. A long history of GERD is associated with the risk for the development of Barrett's esophagus and ultimately esophageal carcinoma. Although often underutilized, minimally invasive antireflux surgery can help manage these patients. However, thorough evaluation and accurate diagnosis of GERD and its underlying pathophysiology are critical in ensuring successful surgical treatment. This review offers a stepwise approach to the diagnostic workup of GERD and how to appropriately tailor available surgical treatments to specific patient subgroups.
Introduction
G
In order to properly and successfully treat GERD, it is of paramount importance to understand its underlying pathophysiology, which goes beyond gastric acid production, currently the only target of medical therapy. Essentially, GERD is caused by the breakdown of one or more components of the antireflux barrier. This barrier is predominantly dependent on a competent lower esophageal sphincter (LES), which can be made defective by decreased intrinsic pressure, overall length, or intraabdominal length, as seen with hiatal hernia. 13 The competence of the LES also relies on effective esophageal peristalsis and gastric motility, as gastric distension decreases LES length and increases the reflux of gastric contents into the esophagus. 13 Thus, defective function of any component of the antireflux barrier can ultimately result in GERD.4,13,14 The role of increased intraabdominal pressure (seen in obese patients) as a cofactor in the pathophysiology of GERD is still largely unknown. Most experts agree on the fact that the treatment of severe reflux in morbidly obese patients should include a different strategic approach than the one used for patients with a normal body mass index (BMI).
The complexity of GERD and the variability in its presentation make its diagnosis and subsequent treatment a challenge. Deciding which patients have failed medical management and what is the next intervention is a matter of debate. However, it is clear is that all patients should undergo a thorough workup in order to confirm the diagnosis and to evaluate the integrity of the various components of the antireflux barrier. In properly selected patients surgical therapy in the hands of an experienced surgeon can achieve long-term satisfactory results. 15 In this review we propose a stepwise approach to the available surgical options for the treatment of GERD to specific patient subgroups. There are currently available endoscopic treatment options for the management of GERD, most with no or limited long-term data on efficacy; these will not be discussed in this review.
Patient Selection: Who Should Be Referred for Surgical Evaluation?
The overwhelming majority of patients suffering from GERD are managed medically. Although available medical options will suffice for the majority of patients, a significant group of patients will experience persistence of symptoms, progression of disease, or development of complications despite maximal medical therapy. These patients should be referred for surgical consultation. 4 Despite the advances and refinement of available surgical options, there has been a steady decline in the number of antireflux surgeries performed in the United States during the last 20 years, with only 18,780 cases in 2010 (Fig. 1).16–19 This decline is likely attributed to several factors. One important hurdle is the general misunderstanding and fear from referring physicians about the long-term morbidity and effectiveness of surgical treatment. The development of endoscopic therapies and the availability of over-the-counter PPIs, both perceived as less invasive interventions, have additionally influenced the fact that fewer patients are being seen for surgical consultation.7,16 However, with as many as 30%–40% of GERD patients experiencing poor symptom control with PPIs,6–9 there is a large subgroup of patients who deserve closer attention and evaluation.
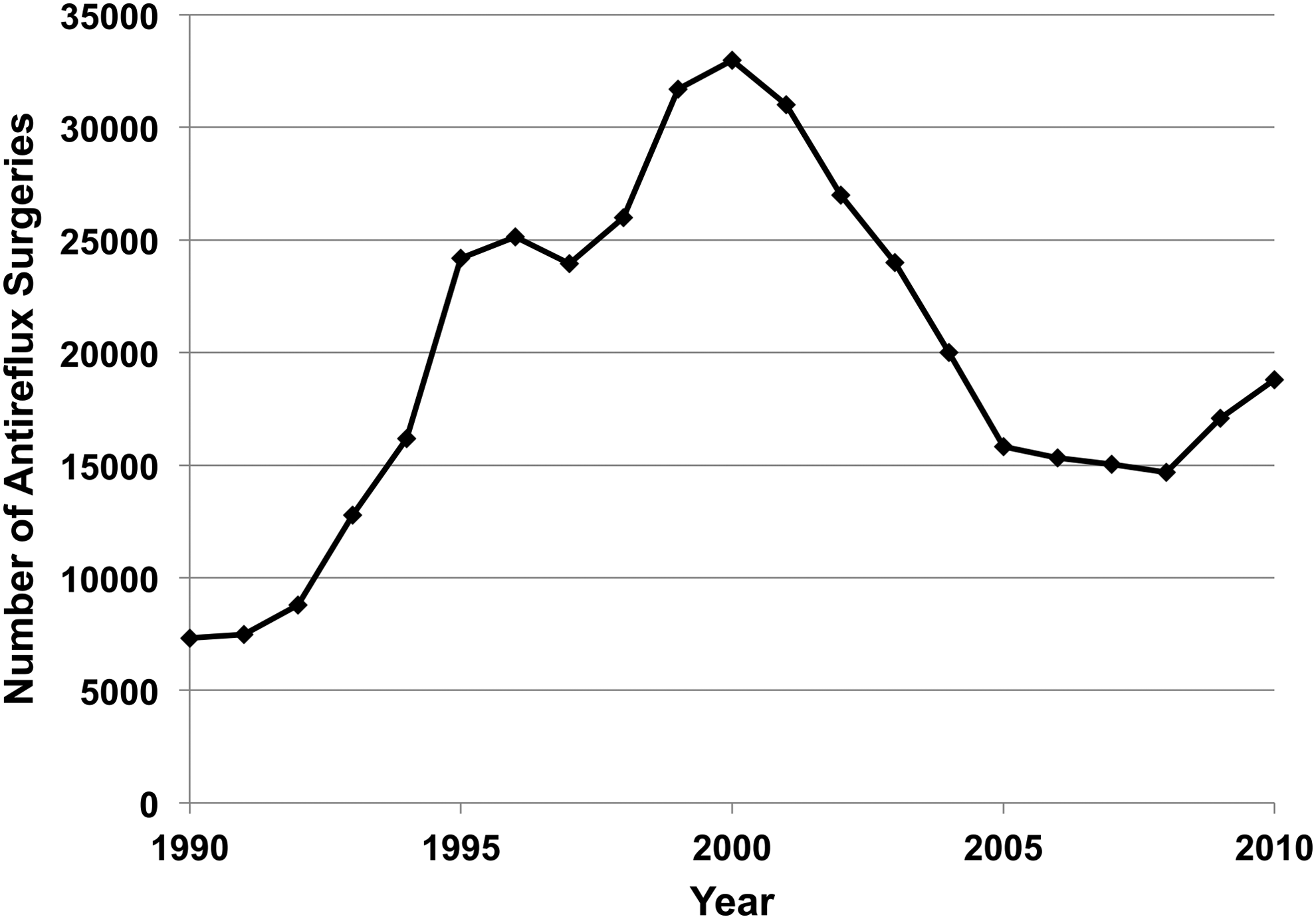
Annual rate of antireflux surgeries performed in the United States from 1990 to 2010.
The Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) 2010 guidelines state that antireflux surgery should be considered in the following clinical scenarios
4
:
1. Failure of medical management (i.e., persistent symptoms, severe regurgitation, side effects of medications). 2. Patient concerns regarding quality of life, expense of medications, and need for lifelong therapy despite successful medical management. 3. Presence of complications of GERD (BE, peptic stricture). 4. Presence of extraesophageal manifestations of GERD (asthma, aspiration, cough, chest pain, hoarseness).
The Antireflux Barrier
The antireflux barrier is composed of multiple physiologic and anatomic components that work together to prevent the reflux of contents from high-pressure distal compartments to low-pressure proximal compartments. 13 The most obvious element of the antireflux barrier is the LES, which serves as a barrier between the high-pressure stomach and low-pressure esophagus. This physiologic sphincter can be rendered incompetent by changes in its intrinsic pressure, overall length, and position.20,21 Patients with an intrinsic pressure of 6 mm Hg or less, a resting LES length of 2 cm or less, or an intraabdominal length of 1 cm or less are at increased risk of reflux. Other factors shown to decrease LES competence include laxity of the diaphragmatic crura and phrenoesophageal membrane, flattening of the angle of His, and development of a hiatal hernia. 14 The integrity of the antireflux barrier at the gastroesophageal junction is maintained by the LES and crura. Crural laxity and disruption of the phrenoesophageal ligament can contribute to hiatal hernia formation and subsequent LES dysfunction due to shortened intraabdominal length and exposure to negative intrathoracic pressure. Even in the absence of hiatal hernia, intrinsic loss of LES tone, increased frequency of LES transient relaxation, and reduction of LES length (both overall and intraabdominal length) can result in significant reflux.
Equally important to the antireflux barrier is the function of the esophagus and stomach. 13 Effective esophageal peristalsis is required for appropriate LES relaxation and esophageal clearance. Additionally, ineffective gastric emptying may lead to gastric distension resulting in shortening of the LES, thus decreasing LES competence. Appreciation of the complexity of the antireflux barrier and understanding its various components are essential in evaluating and treating patients with GERD.
Presurgical Evaluation of Reflux
In evaluating a patient for invasive therapy, it is important to first confirm the presence of GERD and then to study its underlying pathophysiology in order to recommend the appropriate treatment that affords the patient the highest chance for success. A careful history with review of presenting symptoms is an important first step. Then direct investigation of the antireflux barrier is necessary. Past experience has found that successful outcomes are most likely in those with typical symptoms of GERD, increased esophageal acid exposure confirmed on pH testing, and some level of symptomatic response to PPI therapy. 22
Both SAGES and the European Association of Endoscopic Surgery (EAES) recommend esophagogastroduodenoscopy to confirm the diagnosis of GERD and to obtain tissue biopsies.4,5 The diagnosis is firmly established with the presence of severe reflux esophagitis or long-segment BE (≥3 cm Barrett's metaplasia). 7 If there is diagnostic uncertainty or in patients with only mild or no erosive esophagitis or short-segment BE, pH monitoring with or without impedance testing should be used. 7
Once the diagnosis of GERD is confirmed, esophageal manometry should be performed to evaluate esophageal motility. Although manometry is not necessary for the diagnosis for GERD, it is considered mandatory for presurgical evaluation to help identify conditions in which an antireflux procedure may be inappropriate or contraindicated, such as achalasia, ineffective esophageal motility, severe hypomotility secondary to scleroderma, nutcracker esophagus, or distal esophageal spasm.6,7
A barium swallow is useful to delineate the anatomy of the esophagus and to identify a hiatal hernia, diverticulum, peptic stricture, or shortened esophagus.4,21 It can also evaluate the function of the esophageal body and LES. 21 Gastric emptying studies should be considered in select populations such as diabetics and those in whom typical symptoms are associated with nausea and vomiting. 5 This can help identify delayed gastric emptying, gastric outlet obstruction, or gastroparesis as the underlying cause of reflux.
Strategic Approach to Surgical Decision-Making
When deciding on an appropriate therapeutic approach, it is important to closely evaluate all diagnostic studies to determine the underlying pathophysiology causing reflux.
Thus, factors that are critical in surgical decision-making are as follows:
1. Presence/absence of GERD by esophagogastroduodenoscopy/pH study. 2. Assessment of esophageal motility by esophageal manometry. 3. Presence/absence of hiatal hernia. 4. Obesity (BMI >35–40 kg/m2). 5. Assessment of gastric motility.
In the following paragraphs we describe our rationale for surgical treatment of GERD patients. These general guiding principles are further outlined in Figure 2.
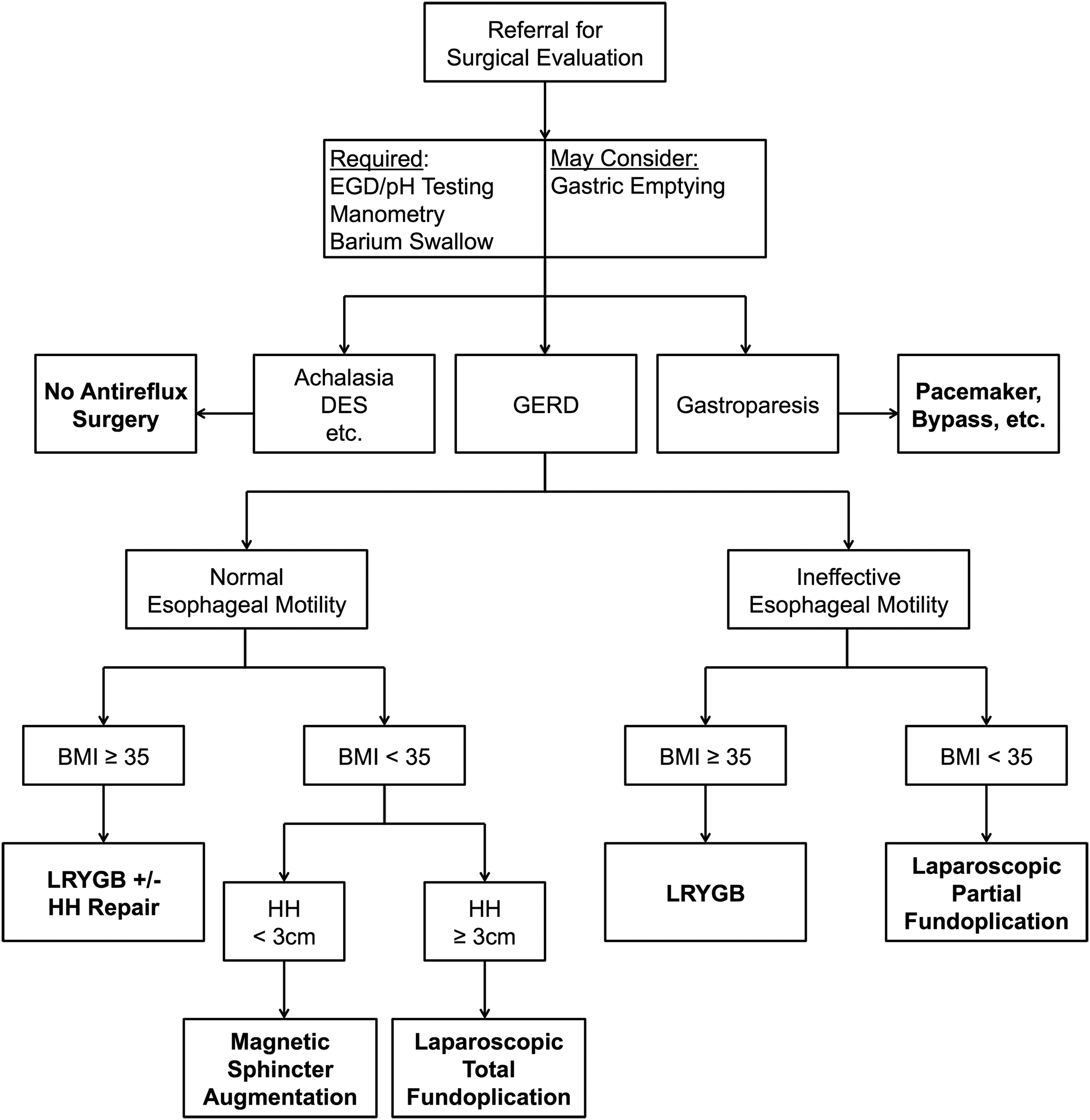
Proposed algorithm for the evaluation and treatment of patients with gastroesophageal reflux disease (GERD). BMI, body mass index (in kg/m2); DES, diffuse esophageal spasm; EGD, esophagogastroduodenoscopy; HH, hiatal hernia; LRYGB, laparoscopic Roux-en-Y gastric bypass.
Severe GERD with minimal or no anatomic disruption (LES dysfunction)
In the setting of normal esophageal motility with a weakened LES, patients with poorly controlled GERD have two surgical options: laparoscopic fundoplication (total or partial) or magnetic sphincter augmentation of the LES.
The current gold standard in this setting is represented by laparoscopic total or partial fundoplication. Long-term data have shown that over 90% of patients have continued symptom control with 70%–92% of patients remaining off daily antireflux medication. 23 Postoperative side effects include transient dysphagia, bloating, early satiety, and flatulence.4,5,23,24 If a hiatal hernia is present, particularly one larger than 3 cm, fundoplication is required to restore the length and competence of the LES. A total fundoplication is preferred in the setting of normal esophageal motility and, as stated above, is a well-proven, safe, and durable intervention in experienced hands.4,21
Critical to the success of this procedure is the need to follow key technical steps. These include the following:
• Complete crural dissection with identification and preservation of both anterior and posterior vagus nerve and reduction/excision of hiatal hernia sac if present. • Circumferential dissection of the esophagus and posterior mediastinum to obtain adequate abdominal esophageal length (3 cm). • Crural closure. • Mobilization of gastric fundus with division of short gastric vessels. • Fundoplication.
The last two steps have been a source of long debate in the surgical community, and although some authors, based on data from randomized controlled trials, 25 may recommend against routine division of the short gastric vessels, all agree that a form of fundoplication—partial or complete—is a mandatory final step for a successful antireflux procedure.
If preoperative evaluation indicates evidence of esophageal dysmotility, continued medical treatment or at a maximum laparoscopic partial fundoplication should be considered depending on the severity and type of dysmotility. Ineffective esophageal motility (ineffective esophageal manometry-contraction amplitudes of <30 mm Hg and <50% peristaltic waves) warrants partial fundoplication,5,21,26 whereas achalasia (aperistalsis) and diffuse esophageal spasm (high-amplitude nonperistaltic contractions) are considered contraindications for antireflux surgery. 7 Studies have shown that partial fundoplication is as effective as total fundoplication in controlling GERD with less postoperative dysphagia up to 5 years after surgery. 27 In addition, SAGES and EAES guidelines both advocate crural approximation and hiatal repair at the time of antireflux surgery.4,5
A recent addition to the surgeon's armamentarium is magnetic sphincter augmentation. This intervention has been studied in patients with severe GERD—proven by pH study—and with normal esophageal motility without hiatal hernia or with a hiatal hernia of less than 3 cm, as well as a BMI below 35 kg/m2.7,28 This is a novel Food and Drug Administration–approved therapy that strengthens the antireflux barrier by placing an expandable ring of titanium beads around the LES, which externally augments its resting pressure. The anatomy of the stomach is left unaltered, minimizing the risk of side effects associated with other antireflux operations, such as dysphagia and inability to belch or vomit. 29 Clinical trials to date have demonstrated normalization or 50% reduction of esophageal acid exposure in 64%–80% of patients.28–32 Postoperative dysphagia was reported in 43%–68% of patients but was self-limited in the majority of patients, resolving by Week 8–9 in most patients. We believe this is a very promising intervention and should be considered as first-line treatment for patients with severe GERD with minimal or no anatomic disruption and normal esophageal motility; results from long-term studies are still needed to confirm 10-year safety and continued efficacy.
Severe GERD with significant anatomic disruption (hiatal hernia >3 cm)
In this setting the patient should be recommended to undergo a laparoscopic total or partial fundoplication following the strict surgical criteria described in the above paragraph.
Morbid obesity (BMI >35 kg/m2)
Obesity is an independent risk factor for the development of GERD and progression to BE, ultimately placing this population at increased risk for esophageal adenocarcinoma.6,33 There are several proposed mechanisms linking obesity to GERD, including increased gastric distension leading to increased frequency of transient LES relaxations 33 and displaced LES secondary to increased intraabdominal pressure. 34 Traditional antireflux operations do not correct the underlying problem, and higher failure rates have been reported in obese individuals compared with normal-weight counterparts.35,36 The most recent SAGES and EAES guidelines recommend gastric bypass in the morbidly obese patient (BMI >35 kg/m2) with uncontrolled GERD as it simultaneously treats GERD, provides weight loss, and improves the associated comorbidities of both conditions.4,5
Abnormal gastric emptying: gastroparesis
An important consideration in patients refractory to medical therapy of GERD is whether or not an underlying gastric emptying component may be present. This is particularly relevant in diabetics, in whom gastroparesis is a common complication. Often the symptoms of GERD and gastroparesis overlap, making the diagnosis and treatment a challenge. When evaluating a patient for antireflux surgery, the surgeon should obtain a thorough history and physical, and, if warranted, a gastric emptying study should be performed to confirm the diagnosis of gastroparesis. In the setting of gastroparesis, delayed gastric emptying causes gastric overdistension, followed by subsequent shortening of the LES and reflux of gastric content into the esophagus. In these patients, fundoplication alone can worsen symptoms of early satiety, nausea, and bloating. Although the treatment of gastroparesis is predominantly medical, surgery should be considered in severe refractory cases. Options include pyloromyotomy, pyloroplasty, subtotal gastrectomy, gastric bypass, and gastric electrical stimulation, to name a few. The diagnostic workup and choice of operation are beyond the scope of this article. However, the presence of gastroparesis in the patient with GERD should be considered during preoperative evaluation for antireflux surgery in the above-mentioned clinical settings.
Conclusions
Although the majority of uncomplicated GERD patients can be appropriately treated with medical therapy, there remains a group of patients who require a more tailored approach for symptom relief and prevention of disease progression. Treatment of the GERD patient who is a “nonresponder” to medical treatment requires a thorough understanding of the antireflux barrier and evaluation of its components. This evaluation of the reflux barrier allows surgeons to appropriately tailor the surgical approach with hopes of excellent long-term outcomes, along with prevention of the sequelae associated with severe GERD.
Footnotes
Disclosure Statement
No competing financial interests exist.