
Abstract
Abstract
Background:
Obesity is an epidemic on the rise. Increasing body mass index (BMI) has been associated with a number of comorbid diseases, including rarely reported motility disorders such as achalasia. Motility disorders are prevalent in obese patients, possibly more prevalent when compared to the nonobese population. Identification of motility disorders is important before bariatric surgery and may alter the planned type of procedure performed. Limited data exist regarding the development or existence of esophageal motility disorders after bariatric surgery. This study aims to characterize patients who have undergone bariatric surgery and subsequently developed or were diagnosed with achalasia.
Methods:
Patients with a diagnosis of achalasia who previously underwent bariatric surgery were identified. Data collected included baseline demographics, perioperative parameters, and postoperative outcomes. Descriptive statistics were computed for all variables.
Results:
Ten patients met the inclusion criteria. All patients had endoscopy and manometry confirming diagnosis of achalasia after previous bariatric surgery. Eight patients had undergone Roux-en-Y gastric bypass (RYGB), and two patients had vertical banded gastroplasty (VBG). Median length of time from bariatric surgery to diagnosis was 6 years. Two patients had undergone Botox® treatment, and five had gone through the scope esophageal dilations. All patients had a surgical intervention for achalasia, specifically Heller myotomy (HM) (n = 4 open, n = 4 laparoscopic) was performed in the eight RYGB patients, whereas near total gastrectomy and esophagectomy (n = 1), and transhiatal esophagectomy with a partial gastrectomy (n = 1), were performed in each of the patients who previously underwent VBG. These patients were considered to have end-stage achalasia. All patients showed significant decrease in BMI after bariatric surgery (11.1 ± 1.5 kg/m2). Six of the eight patients who underwent HM achieved resolution of achalasia symptoms at a mean time of 1.6 months and remained asymptomatic for the total follow-up of 36 months. One patient developed recurrent achalasia 2 years after HM and subsequently underwent a peroral endoscopic myotomy. One HM patient was lost to follow-up. The two patients who underwent esophagectomies were symptom free at 36 months.
Conclusion:
Although the incidence of achalasia in the bariatric population is unknown, it does coexist and should be treated when identified. Dysmotility is not uncommon and rarely is the workup completed to identify achalasia before bariatric surgery. Increasing our attention to identify motility diseases preoperatively and specifically raising awareness that achalasia can occur after bariatric surgery will result in better care for patients. Our results suggest achalasia can be effectively treated with surgical therapy after previous bariatric surgery.
Introduction
O
Methods
Patients
After institutional review board approval was obtained, patients with a diagnosis of achalasia who had previously undergone bariatric surgery between 2000 and 2012 were identified through Cleveland Clinic's electronic medical records (EMR) using current procedural terminology (CPT) and international classification of diseases-9th edition (ICD-9) codes. Specifically, CPT codes for Heller myotomy (HM) type procedures and ICD-9 codes for achalasia were used. A total of 2733 patients with achalasia were identified, of which 280 received surgical treatment (Fig. 1). The records were then further reviewed to select patients who also had documentation of prior bariatric surgery. Patients' aged 18–75 years were included in this retrospective analysis. Data, including demographic data, date of diagnosis of achalasia, achalasia-related symptoms, achalasia workup (manometry, time barium swallow [TBS], and histologic diagnosis [Fig. 2]) smoking history, previous surgical procedures, and comorbid conditions, were collected for all patients. Data regarding the bariatric procedure, onset of achalasia, and treatment modalities were collected.
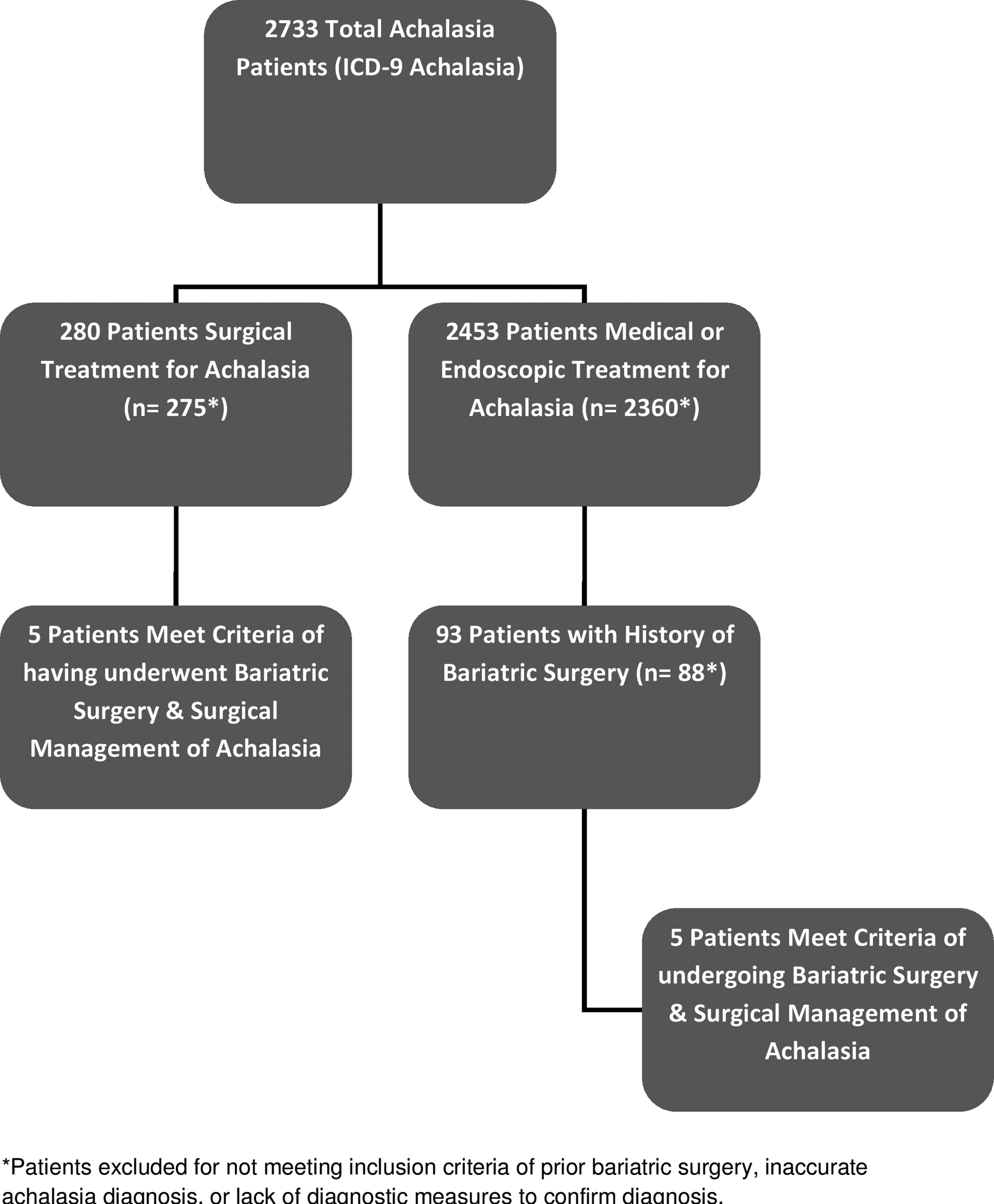
Algorithm depicting inclusion and exclusion of patients.
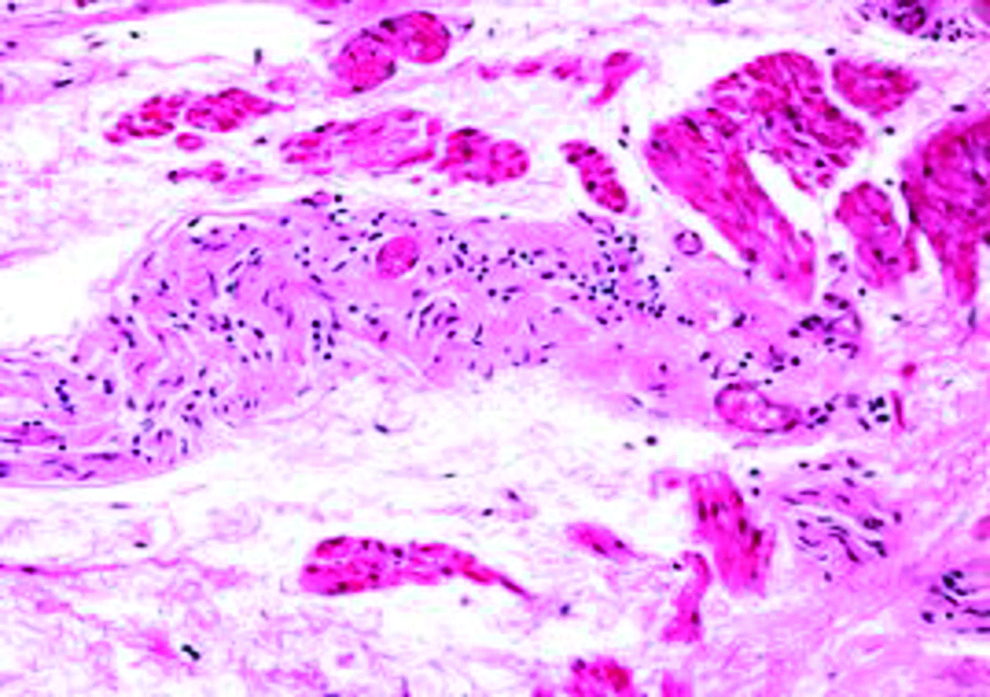
Histologic section of myotomy specimen.
Statistical analysis
Descriptive statistics were computed for all variables.
Results
A total of 10 patients (3 male, 7 female) developed achalasia after bariatric surgery and met inclusion criteria. Ages ranged from 29 to 63 years with a mean age of 46.9 years at the time of bariatric surgery. Median BMI at the time of bariatric surgery was 54.0 kg/m2. Seven patients had a clinical history of GERD before a diagnosis of achalasia, but only one underwent formal pH testing before bariatric surgery (6 out of 10 unknown) (Table 1). Eight patients had an RYGB and two had a vertical banded gastroplasty (VBG) previously performed. All patients underwent esophagogastroduodenoscopy (EGD), upper gastrointestinal series (UGI) with TBS, and esophageal manometry for diagnosis. Histology that demonstrated reduced or absent myenteric ganglion cells as a confirmation of diagnosis was available in five patients (Table 2 and Fig. 2).
ASA, American Society of Anesthesiologists; BMI, body mass index; EGD, esophagogastroduodenoscopy; F, female; GERD, gastroesophageal reflux disease; LRYGB, laparoscopic Roux-en-Y gastric bypass; M, male; NA, not available; NR, not recorded, data were not accessible after thorough review of medical records, or could not be inferred from the information available; RYGB, Roux-en-Y gastric bypass; VBG, vertical banded gastroplasty.
Achalasia type determined using Chicago classification.
Other: patient 1 had near-total gastrectomy with esophagectomy and patient 5 had transhiatal esophagectomy, partial gastrectomy with pyloromyotomy.
LES, lower esophageal sphincter; LHM, laparoscopic Heller myotomy; NA, not available; OHM, open Heller myotomy.
The median length of time from bariatric surgery to diagnosis of achalasia was 6 years. Two patients were treated with Botox®, and five had gone through the scope esophageal dilations. All patients eventually underwent surgical intervention for definitive treatment of achalasia. HM (n = 4 open, n = 4 laparoscopic) was performed in the 8 RYGB patients, whereas near total gastrectomy and esophagectomy (n = 1), and transhiatal esophagectomy with a partial gastrectomy (n = 1), were performed in each of the patients who previously underwent VBG. The patients with previous VBG were considered to have end-stage achalasia (Table 2). Six out of the eight patients who underwent HM had resolution of achalasia symptoms at a mean follow-up time of 1.6 months and remained asymptomatic for the total follow-up of 36 months. One patient developed recurrent achalasia 2 years after HM and subsequently underwent a peroral endoscopic myotomy. One HM patient was lost to follow-up. The two patients who underwent esophagectomies for definitive treatment reported symptom resolution at 36 months. All patients showed significant decrease in BMI after bariatric surgery (11.1 ± 1.5 kg/m2). Eight patients had a history of smoking with an average 12-pack year smoking history.
Discussion
Achalasia is a rare esophageal motility disorder with a reported incidence of ∼1.5/100,000 people. 8 Typical clinical presentation involves progressive dysphagia and chest pain. It is characterized by failure of the lower esophageal sphincter (LES) to relax especially upon deglutition, and a baseline normal or increased LES pressure. Aperistalsis is pathognomonic.
However, the exact pathophysiology is not completely understood. Transition from other esophageal motility disorders (such as diffuse spasm, nonspecific motor disorders, and GERD) to achalasia has been documented in the literature and may suggest a common pathogenesis. 9
Obesity has been reported as an independent risk factor in the development of esophageal motility disorders.5,6,10 Motility disorders in obese patients are rare, but existent. Obese patients with motility disorders may present with atypical or extraesophageal symptoms, if any symptoms at all. This may make timely and accurate diagnosis challenging. In a study reporting on 111 morbidly obese patients by Jaffin et al., 68/111 (61%) patients were noted to have at least one abnormality on esophageal manometry. The authors report that 28/111 (25.2%) patients were found to have hypotensive LES. GERD incidence was reportedly greater in 18/28 (66%) patients with hypotensive LES, in comparison to 17/83 (20%) (p < 0.02) patients with normal LES pressure. Approximately, 60% of patients with motility abnormalities were asymptomatic, making identification more challenging, and increasing the likelihood of misdiagnosis. 5 This study did not report significant findings regarding correlation of BMI to LES pressure.
Furthermore, there is incomplete and contradictory evidence on the impact of bariatric surgery on esophageal motility.2,5,11 There are limited data on achalasia in the obese population, especially in those who have undergone bariatric surgery. The majority of the published literature consists of case reports describing achalasia after RYGB. A case report presented by Ramos et al. describes a patient who developed achalasia approximately 4 years after RYGB. The patient presented with classical symptoms of regurgitation and dysphagia to solid foods. The diagnosis was confirmed after barium esophagogram and esophageal manometry detecting a dilated esophagus with a classical “bird beak” appearance and achalasia with aperistalsis on manometry. This patient's symptoms resolved after performing laparoscopic anterior myotomy. Chapman et al. also presents a case report that confirms a patient developing achalasia 2 years after open gastric bypass. Similarly, Shah et al. also reports two patients who developed achalasia after RYGB. The authors hypothesize that trauma secondary to surgery may serve as a promoting factor in the development of achalasia. In addition, it is hypothesized that trauma may cause damage to the vagal nerve during surgery to the foregut or chest, furthermore causing vagal dysfunction and possibly contributing to the development of achalasia.7,9 Some studies have reported sequelae of esophageal dilatation after these procedures in addition to the well-documented condition of pseudoachalasia after LAGB.2,12,13 There are theories describing the development of achalasia, which may be linked to the indirect effect of RYGB on the LES pressure. Schrumpf et al. suggests that postprandial gastrin levels decrease as an effect from vagotomy to the gastric remnant, causing an increase in the resting tone of the LES.
Our study is the largest series, to date, of patients developing achalasia after bariatric surgery. Morbid obesity is considered a contributing risk factor in the development of esophageal motility disorders, with a reported prevalence of 20%–61%.5,6,10 Smoking has both a direct and indirect effect on diseases across systems. The effect of smoking on the esophageal mucosa promotes malignant changes, but an established link to esophageal motility disorders is yet to be made. In particular, patients with achalasia after bariatric surgery often have dysphagia, resulting in transition to liquid-based foods. Ingestion of these liquid high-calorie foods may result in suboptimal weight loss if uncorrected. In this series, all patients underwent surgical intervention for treatment of achalasia with acceptable results. Limitations of this study include the small number of patients, no control cohort, the lack of testing for achalasia before bariatric surgery, and the usual limitations of a retrospective study, including selection bias and missing data points.
Conclusion
Esophageal dysmotility is not uncommon in obese patients and usually is not evaluated before bariatric surgery unless symptoms are severe. With careful attention, both pre- and postbariatric surgery symptoms may result in better and timely intervention for achalasia. Our results suggest that achalasia can be effectively treated with surgical therapy after bariatric surgery.
Footnotes
Acknowledgments
Writing of article and data entry (M.B.), writing of article (R.C.), data entry (A.Z. and E.B.), statistical support (D.F.), final review (J.R.), final review/study concept (S.B. and K.E.-H.), and final writing of article/final review/study concept (M.K.).
Disclosure Statement
No competing financial interests exist.