
Abstract
Abstract
Background:
Further minimization of abdominal wall trauma during laparoscopic bariatric surgery is a topic of great interest. Reducing the number of trocars may provide superior cosmetic results with less pain and shorter length of stay (LOS). However, it remains unclear if this approach compromises safety or effectiveness of weight loss. The aim of this study is to report initial safety and feasibility results using a three-port minimally invasive sleeve gastrectomy technique.
Materials and Methods:
A retrospective review of patients who underwent laparoscopic three-port sleeve gastrectomy (3PSG) at our institution was conducted. Patient demographics, intraoperative parameters, and perioperative outcomes were extracted and analyzed. Postoperative data were obtained from routine follow-up history and physical examination.
Results:
From May 2013 to April 2014, 45 morbidly obese patients underwent 3PSG. The cohort had a male-to-female ratio of 20:25, mean age of 47.4 ± 11.6 years, and a mean preoperative body mass index (BMI) of 47.6 ± 9.7 kg/m2. The mean number of comorbidities was 4 (range 0–8), and the mean American Society of Anesthesiologists score was 2.82 (range 1–4). Mean procedural duration and blood loss were 165 ± 31.9 minutes and 27.0 ± 31.8 mL, respectively. Eight patients (17%) required one additional trocar. Two cases (4.4%) had an intraoperative complication (staple line bleeding and splenic capsule laceration). Two (4.4%) postoperative complications were encountered (wound infection and axillary vein thrombosis). The mean LOS was 2.7 (range 2–7) days. At a mean follow-up of 5 (range 0.4–11.7) months, the cohort had a mean BMI of 40.0 ± 9.26 kg/m2, which corresponded to a mean excess weight loss of 36.0% ± 18.1%. There were no trocar site hernias. All patients were highly satisfied with the final cosmetic result.
Conclusion:
Laparoscopic 3PSG appears to be a safe and feasible technique for performing sleeve gastrectomy. While further long-term research is needed, it appears to have significant benefits, mainly patient satisfaction and potentially less pain.
Introduction
S
The technical details of LSG vary from surgeon-to-surgeon, but the principle is to remove the vast majority of the stomach (especially the fundus), leaving only a narrow gastric tube from the esophagus to the pylorus, and reducing the production of ghrelin. 5 The absence of a gastrointestinal anastomosis during the operation and leaving patients with intact gastrointestinal continuity are other potential benefits of this new technique. LSG is considered a restrictive procedure, although it has been increasingly recognized to have metabolic effects similar to those observed after Roux-en-Y gastric bypass (RYGB).
A recent 5-year outcome study has reported successful LSG results, with an 86% average excess weight loss (EWL). 6 However, other studies have demonstrated more modest long-term weight loss results (especially in patients with body mass index [BMI] >50 kg/m2). 7 Current meta-analysis data suggest that LSG is the second most common bariatric operation performed around the world after laparoscopic RYGB. 8
The standard LSG procedure described by Trellelles and Gagner requires between six and seven trocars, although modifications of the initial procedure have been described. 9 Recent developments in minimally invasive surgery have been focused on reducing the size or number of ports to achieve the ultimate goal of minimal invasiveness. Single-incision laparoscopic surgery (SILS) is still being evaluated for its utility in the field of bariatric surgery. The limited studies of single-incision bariatric surgery that exist have suggested that SILS is safe and feasible in qualified hands.10,11 Better cosmetics, less postoperative pain, and shorter hospital stay are potential advantages of SILS over conventional laparoscopic bariatric surgery. However, safety, long-term weight loss, and incisional hernia are still controversial issues with regards to the SILS technique. The laparoscopic three-port sleeve gastrectomy (3PSG) has been recently described as a promising alternative between the standard LSG and SILS sleeve gastrectomy (SILS-SG). 12 The objective of this study is to report initial safety and feasibility results using a 3PSG technique.
Materials and Methods
After institutional review board approval was obtained, a retrospective review of patients who underwent 3PSG at our institution was conducted. Patient demographics identified included age, sex, height, weight, BMI, comorbidities, number and type of previous abdominal surgeries, and American Society of Anesthesiologists (ASA) score. Operative parameters extracted included operative time (OT), estimated blood loss (EBL), intraoperative events, and complications. Postoperative data were obtained from routine follow-up history and physical examination. Postoperative outcomes utilized were length of stay (LOS), postoperative complications, need for readmission, duration of follow-up, weight, BMI, and presence of complications at follow-up. These data were then used to calculate percentage of EWL of the cohort. The EWL was defined as the operative weight minus the follow-up weight, divided by the excess weight, and multiplied by 100. Excess weight was defined as the operative weight minus ideal body weight based on a BMI of 25 kg/m2. Categorical variables were reported as frequencies (%). Continuous variables with normal and non-normal distributions were presented as mean ± standard deviation and median (range), respectively.
Operative technique
A supraumbilical incision is made and the subcutaneous fat tissue dissected down to the level of abdominal wall fascia. Then a Veress needle is inserted and the abdomen is insufflated to a pressure of 15 mmHg. A 12-mm ENDOPATH XCEL® port laparoscope is inserted under direct vision and the abdominal cavity inspected. Next, 5-mm left lateral and right paramedian ports are placed slightly up from the 12-mm trocar site (Fig. 1). If needed, the liver is internally suspended using suture (n = 15, 2-0 polyester Endo Stitch) (Fig. 2). We then mobilize the greater curvature of the stomach from the angle of His down to the pylorus. A green load (Ethicon ECHELON ENDOPATH™) of the stapler is then applied about 4 cm from the pylorus parallel to the lesser curvature (Fig. 3). Next, we pass the flexible endoscope down the esophagus along the lesser curvature of the stomach and into the pylorus. Two or more applications of the stapler (green load) are then fired parallel to the endoscope and then multiple blue loads (Ethicon ECHELON ENDOPATH) are applied parallel to the endoscope up toward the angle of His. Short gastric vessels at the His angle are transected after the last stapling. Staple lines are carefully examined on both sides, and the gastric remnant is placed in a sterile bag and removed through the 12-mm trocar site. The fascia of the 12-mm trocar port was closed with Vicryl® 2-0 sutures.

Image depicting trocar placement.
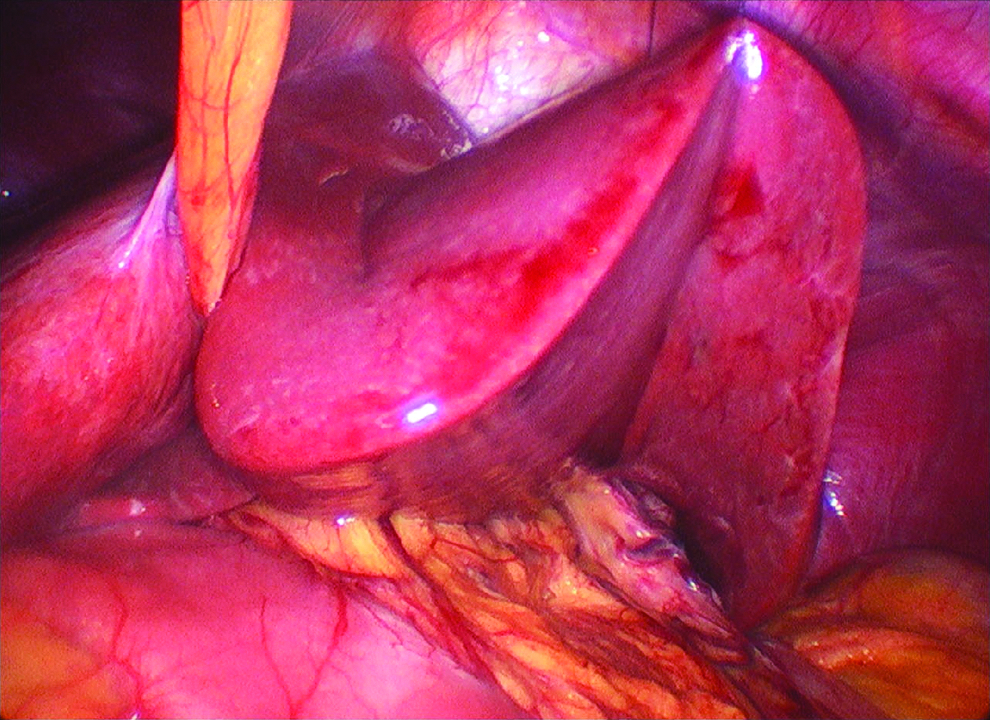
Image depicting left lobe liver suspension.
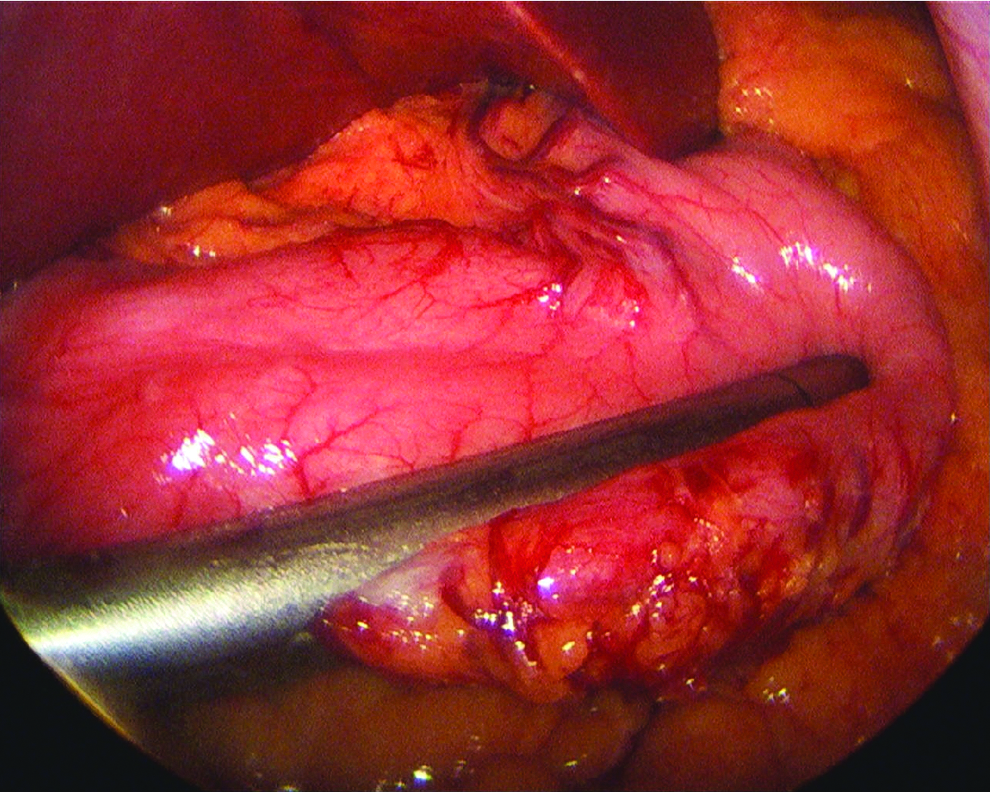
Image depicting gastric sleeve transection.
Results
We identified 45 patients who underwent 3PSG from May 2013 to April 2014. The cohort had a male-to-female ratio of 1:1.2, mean age of 47.4 ± 11.6 years, and a mean preoperative BMI of 47.6 ± 9.7 kg/m2. The mean number of comorbidities was 4 (range 0–8), and the mean ASA score was 2.8 (range 1–4). Of the 45 patients, 80% had obstructive sleep apnea, 78% had hypertension, 42% had hyperlipidemia, and 24% type 2 diabetes. Mean procedural duration and blood loss were 165 ± 31.9 minutes and 27.0 ± 31.8 mL, respectively. Eight patients (17%) required one additional trocar. Two cases (4.4%) had an intraoperative complication (staple line bleeding and splenic capsule laceration). Two (4.4%) postoperative complications were encountered (wound infection and axillary vein thrombosis). The mean LOS was 2.7 (range 2–7) days. Mean visual analog scale (VAS) pain score at postoperative days 1 and 2 was 2.6 and 3.4, respectively. At a mean follow-up of 5 (range 0.4–11.7) months, the cohort had a mean BMI of 40.0 ± 9.26 kg/m2, which corresponded to a mean EWL of 36.0% ± 18.1%. There were no trocar site hernias. All patients were highly satisfied with the final cosmetic result (Fig. 4).

Image depicting patient scars.
Discussion
Minimally invasive surgery has numerous advantages compared to open surgery, including decreased postoperative pain, less postoperative wound-related complications, shorter hospital stay, faster recovery, and better cosmetic results. Over the past few years, novel technologies have been developed that focus on even lesser invasive operative procedures. For instance, SILS-SG has been proposed to be safe and effective with good early postoperative results and less wound-related complications. 13
Recently, we retrospectively compared short-term outcomes between groups of patients undergoing SILS-SG (n = 14) and standard sleeve gastrectomy (n = 14). The EBL, OT, length of hospital stay, overall 90-day perioperative complication rate, and weight loss were comparable in both groups, and only pain score at day 1 was significantly less for SILS patients (P = .007). 11 However, the results of multiport conventional LSG are already excellent, and direct comparison with prospective randomized trials of SILS with conventional LSG is lacking. Currently, only one prospective comparative analysis has been published, and this study (n = 300 patients in each arm) was done in carefully selected patients by highly qualified surgeons in SILS. 13 At 2 years follow-up, Lakdawala et al. observed that SILS-SG was less painful compared with conventional LSG, although all other variables (weight loss, resolution of comorbidities, and incisional hernia) were comparable in both groups. 13
Several technical difficulties arise when utilizing the single-incision approach. Navigating the complex instruments and loss of triangulation because of the limited area of movement can be inconvenient for the operating surgeon and can tend to make SILS-SG more difficult than conventional LSG. The size of the incision required in SILS is another concern due to the potentially higher incidence of wound-related complications, longer recovery, and even higher postoperative pain in relation to the enlarged size. 1 Another argument against SILS can be whether elimination of 5-mm ports translates into cosmetic improvement, because 5-mm scars tend to be difficult to see 1 year after the procedure. In fact, long-term cosmetic outcomes from SILS and three-port laparoscopic procedures such as appendectomies and cholecystectomies are similar, minimizing the potential cosmetic advantage of SILS.14,15 Ultimately, the learning curve for surgeons to comfortably accomplish these techniques seems to be longer and may be one reason why SILS-SG has not gained widespread popularity.
An “ideal” solution to the difficulties surrounding SILS-SG may be the 3PSG technique. Potential advantages of 3PSG over SILS-SG are better triangulation, no need for different instruments, and likely a shorter learning curve. The safety and feasibility of 3PSG was initially reported by Arru et al. in a small prospective study. 12 Twenty-five patients with baseline BMI >50 kg/m2 underwent 3PSG and were followed for 3 months after the procedure. Overall, perioperative outcomes reported were excellent, with a mean operation time of 72 (range 50–110) minutes and only one conversion to a four-port procedure. Importantly, no complications were observed in the 25 patients included in this study. 12 We present a larger sample size (n = 45) with satisfactory outcomes, specifically in LOS (mean = 2.7 days), postoperative pain control (mean VAS = 2.6), and cosmetic effect (Fig. 4) compared with the standard LSG data available. 4 However, we do report two intraoperative complications (staple line bleeding and splenic capsule laceration) that required subsequent conversion to four-port LSG. Both cases were safely controlled by adding an additional port and conventional hemostatic maneuvers. Despite the reported successes of LSG, staple line bleeding continues to be a serious complication (1%–3%) in large published series. 16 There are numerous methods, including buttressing material or staple line reinforcement, which can decrease the chances of staple line bleeding. Results are controversial with regard to the optimal strategy, and we opted to routinely oversew the staple line in this series.17,18
None of the study cohort required reoperation or experienced clinically apparent trocar site hernia. Unfortunately, 2 patients (4%) in our study did experience postoperative complications (wound infection and deep vein thrombosis). While the potential benefit of 3PSG is to reduce wound-related complications, we did encounter a wound infection at the specimen extraction site (necessary regardless of technique) that was treated with local and systemic antibiotics. The patient with an axillary vein thrombosis was a high-risk patient with Factor V Leiden thrombophilia that despite adequate anticoagulation prophylaxis developed this complication during the early postoperative period. This patient was discharged with no further complications on warfarin.
One of the potential advantages of reduced port laparoscopic surgery is the improvement in pain control. In this study, we observed adequate postoperative control of surgery-related pain. The mean postoperative VAS score at days 1 and 2 was 2.6 and 3.4, respectively. Importantly, the VAS scores were inferior to those reported in our published SILS-SG series. 11 The differences in OT in our study compared to Arru et al.'s cohort can be explained by the additional procedures performed in 6 (13.3%) of our patients, including hiatal hernia repair (n = 2), umbilical hernia repair (n = 2), and extensive lysis of adhesions (n = 2). Another potential factor that may explain our longer mean OT may be related to the learning curve of residents and fellows performing portions of these cases at our academic institution.
Reduced port laparoscopic surgery has been developed in other fields of general and oncologic surgery. 19 Kim et al. recently demonstrated the feasibility and effectiveness of reduced port laparoscopy in early gastric cancer. Three-port distal gastrectomy was performed in 30 patients with optimal perioperative and oncologic results (number of lymph nodes dissected). 19 The safety, effectiveness, and cosmetic advantages of three-port surgery have also been described for laparoscopic colorectal cancer, while maintaining the oncologic principles of cancer surgery. 20
To the best of our knowledge, we present the largest series in 3PSG (n = 45). However, there are limitations to this study, including retrospective design, low case number, short-term follow-up, and the lack of a surgical control group. Further prospective research is needed to clarify the risk/benefit ratio of 3PSG.
Conclusion
Laparoscopic 3PSG appears to be a safe and feasible technique for performing sleeve gastrectomy. While further long-term research is needed, it appears to have benefits, mainly patient satisfaction and potentially less pain than standard LSG approaches.
Footnotes
Acknowledgments
None relevant by any of the authors and no funding in correspondence with the study. R.C.: writing of the article; M.B.: writing of the article and data entry; D.F.: writing of the article; C.D.: data entry; A.H.: data entry; P.S.: final review/study concept; and T.R.: final writing of the article/final review/study concept.
Disclosure Statement
No competing financial interests exist.