
Abstract
Abstract
Objective:
The concept of reducing the number of transabdominal access ports has been criticized for violating basic tenets of traditional multiport laparoscopy. Potential benefits of reduced port surgery may include decreased pain, improved cosmesis, less hernia formation, and fewer wound complications. However, technical challenges associated with these access methods have not been adequately addressed by advancement in instrumentations. We describe our initial experience with the NovaTract™ Laparoscopic Dynamic Retractor.
Methods:
A retrospective review of all patients who underwent two-port laparoscopic cholecystectomy between 2013 and 2014 using the NovaTract retractor was performed. The patients were equally divided into three groups (Group A, B, C) based on the order of case performed.
Results:
Eighteen consecutive patients underwent successful two-port laparoscopic cholecystectomy for symptomatic cholelithiasis. Mean age was 39.9 years and mean body mass index was 28.1 kg/m2 (range 21–39.4). Overall mean operative time was 65 minutes (range 42–105), with Group A of 70 minutes, Group B of 65 minutes, and Group C of 58 minutes (P = .58). All cases were completed laparoscopically using the retraction system, without a need for additional ports or open conversion. No intra- or postoperative complications were seen. All patients were discharged on the same day of surgery. No mortality found in this series.
Conclusions:
The NovaTract laparoscopic dynamic retractor is safe and easy to use, which is reflected by acceptable operative time for a laparoscopic cholecystectomy using only two ports. The system allows surgical approach to mimic the conventional laparoscopic techniques, while eliminating or reducing the number of retraction ports.
Introduction
I
As laparoscopy becomes less invasive, optimal retraction is oftentimes compromised. Dedicated retraction ports are usually the first to be eliminated. Inadequate retraction undoubtedly serves as an obstacle when performing laparoscopic operations, especially when the anatomy is atypical. In addition to the inevitable prolongation of operative time, inadequate retraction and visualization can potentially convert a technically straightforward operation into a complex maladventure. Therefore, surgeons have been developing novel methods of obtaining adequate retraction to accomplish the procedure safely with reduced port, less trauma, and invisible scars.
The technical challenges associated with these access methods, however, have not been adequately addressed by advancement in instrumentations. In this study, we describe our initial human experience of two-port laparoscopic cholecystectomy (LC) using the NovaTract™ laparoscopic dynamic retractor. Various other methods of retraction used for reduced-port LC were also reviewed.
Materials and Methods
A retrospective review of a prospectively maintained database of all patients who underwent two-port LC between September 2013 and July 2014 using the NovaTract laparoscopic dynamic retractor was performed. Inclusion criteria include all patients who presented with symptomatic cholelithiasis and chronic cholecystitis. Patients who presented with acute cholecystitis, gangrenous cholecystitis, choledocholithiasis, Mirizzi syndrome, and pregnancy status were excluded from this initial study, to avoid a wide variability in disease severity and its associated differences in the degree of technical difficulty during performance of the cholecystectomy. All cases were performed by a single minimally invasive trained surgeon in an academic tertiary referral center (senior author). The study was approved by the institutional review board. After successful trial on porcine models, approval was obtained to perform cholecystectomies using the device on human subjects. The LC was performed with patients in a standard supine position. A 5-mm camera port at the umbilical location and an 11-mm working port at subxiphoid location were used. The operative dissection of the Calot triangle to expose the critical view of safety was similar to that of the conventional four-port LC. Dissection of the gallbladder specimen from the liver bed was completed using a monopolar hook electrocautery in a standard manner. An Endo Catch™ bag (Covidien, Norwalk, CT) was routinely used to remove the gallbladder specimen using the 11-mm subxiphoid working port.
The patients were equally divided into three groups (Group A—first six cases, B—second six cases, C—last six cases). Patient demographics, perioperative major complications (bleeding, infection, bile duct injury, and bile leak), operative time, estimated blood loss, conversion rate, and pathology reports were recorded and compared among the groups. Statistical analysis was performed using analysis of variance (ANOVA). P-value of <.05 was considered statistically significant.
The NovaTract laparoscopic dynamic retractor
The device consists of a delivery system that includes a deployable abdominal wall stainless steel anchor, a deployable atraumatic toothed grasper, all of which are attached to a retraction line (Figs. 1–3). The system is reloadable and it can be delivered through a 5-mm laparoscopic port. After a proper access, a target tissue/organ (in this case gallbladder fundus) is held securely by the deployed grasper. The anchor is then deployed against the abdominal wall, which acts as a fulcrum for the retraction line (Figs. 3 and 4). The retraction line can be pulled through a trocar with varying degrees of tension to manipulate the gallbladder, while simultaneously freeing up this trocar for other working instruments or camera (Fig. 5). The locations of both the anchor and the grasper can be easily altered or adjusted during the operation to achieve critical view of safety (Fig. 6). The two standard 5-mm right upper quadrant retraction ports, which are typically used in a conventional four-port LC, are no longer necessary. The device was designed to meet several objectives, such as ease of use, reestablishment of working angles mimicking the conventional multiport laparoscopy, 5-mm introduction platform, adjustable tension with simple manipulation, and secure atraumatic tissue grip.
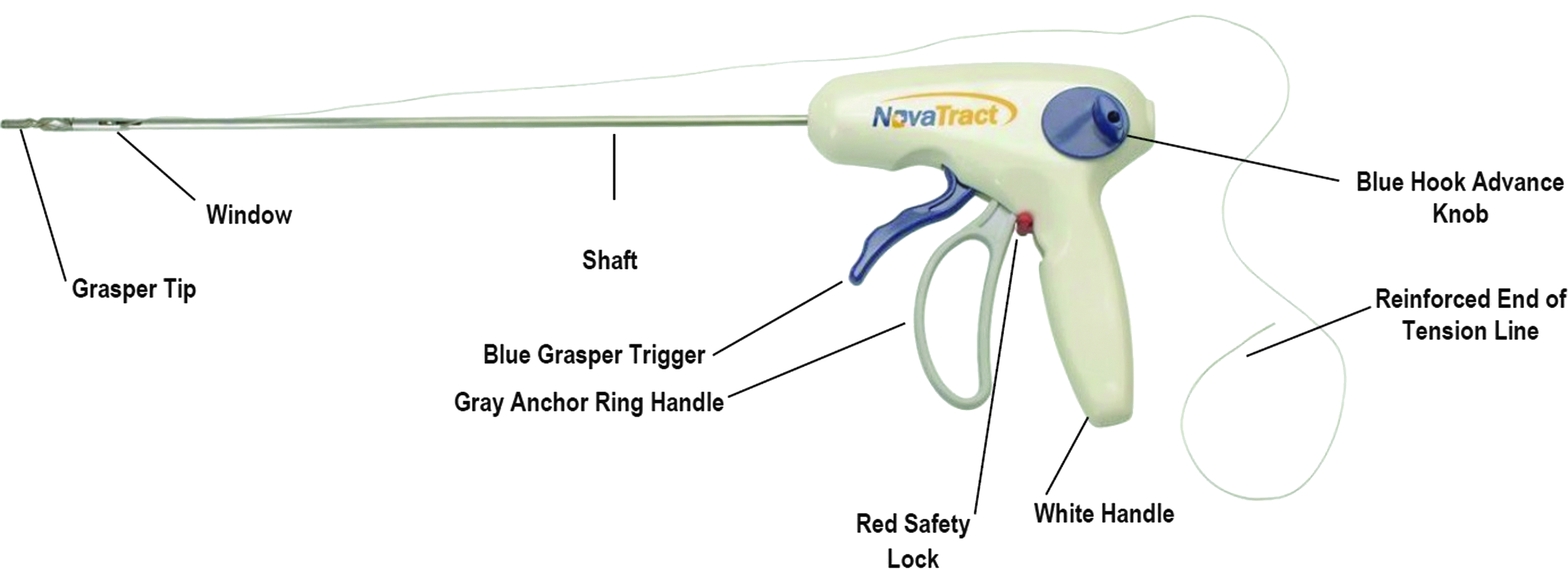
NovaTract™ laparoscopic dynamic retractor.
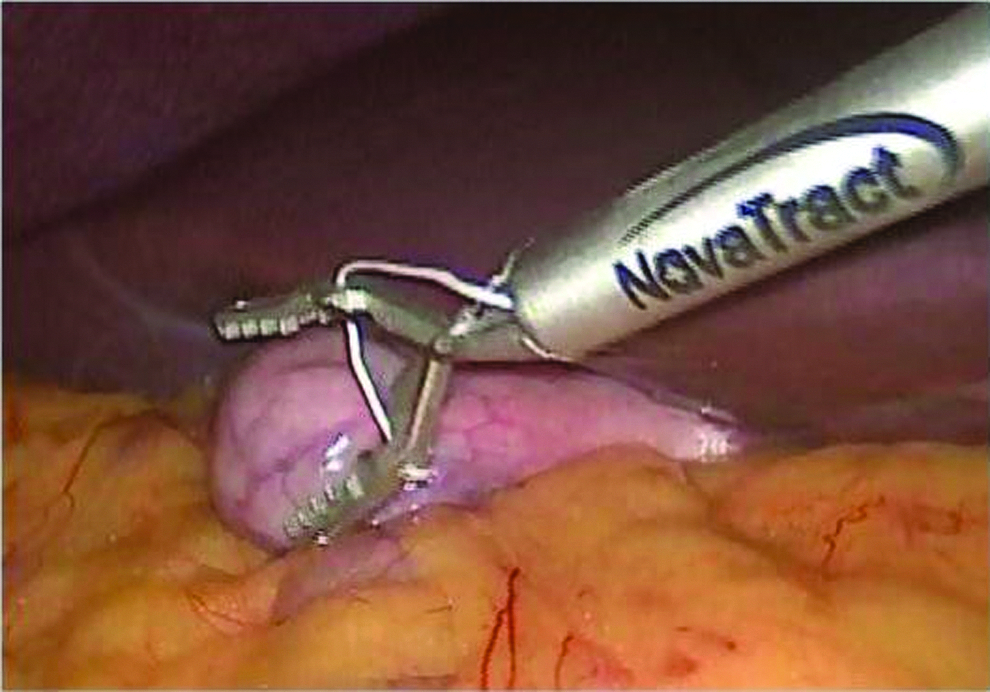
Device deploying atraumatic grasper on gallbladder fundus.
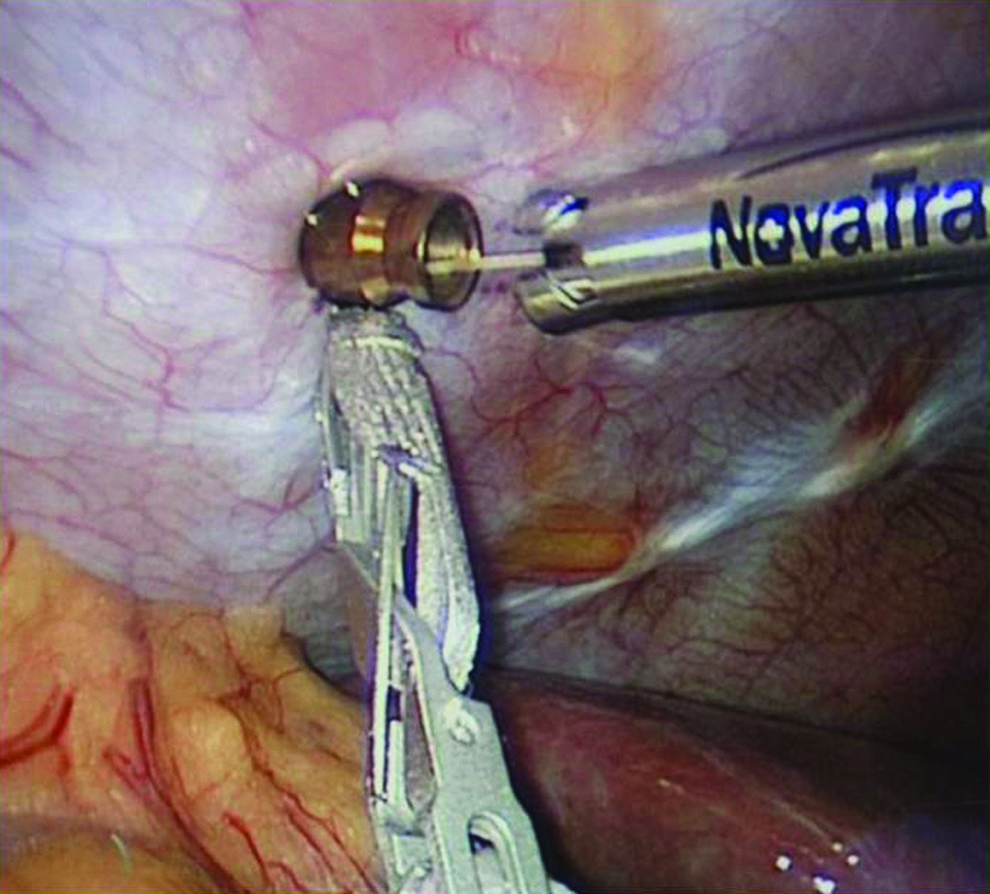
Device deploying anchor to the abdominal wall.
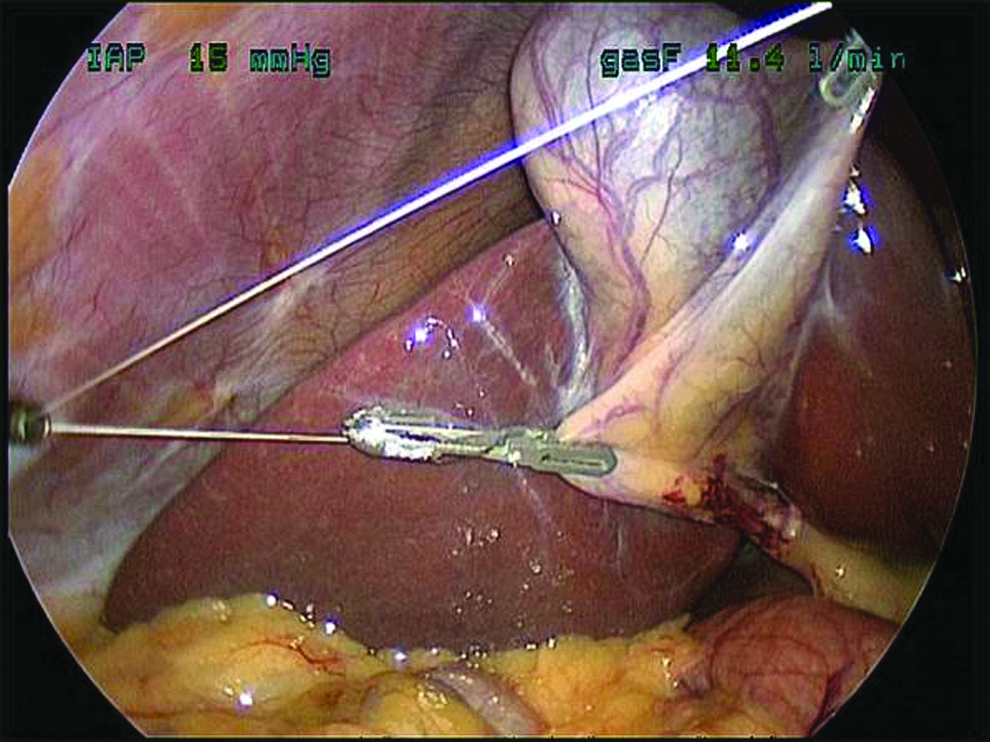
Adjustable traction on the tension line facilitates tissue dissections.
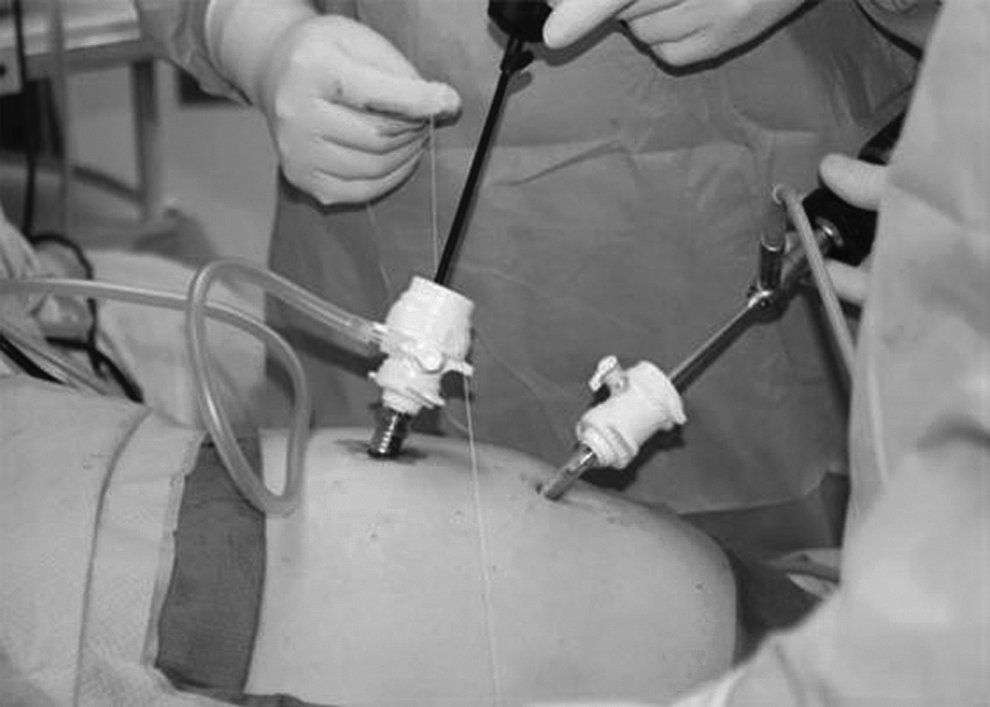
Outside view of the tension line, which can be manually adjusted during tissue dissections. Two standard 5-mm right upper quadrant retraction ports typically used in conventional four-port laparoscopic cholecystectomy are no longer necessary.
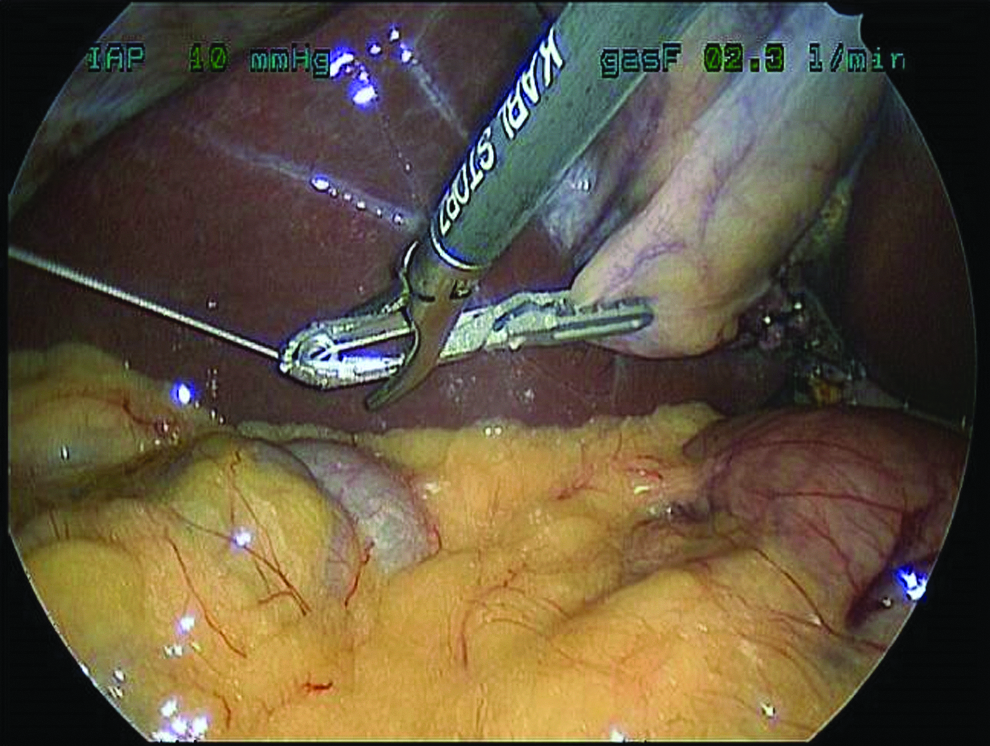
Easy adjustment and repositioning of the atraumatic grasper using a laparoscopic Maryland to gain an optimal tissue counter-traction.
Results
Eighteen consecutive patients (Female:Male = 14:4) underwent successful two-port LC with a preoperative diagnosis of symptomatic cholelithiasis. Mean age was 39.9 years (range 22–72) and mean body mass index (BMI) of 28.1 kg/m2 (range 21–39.4) with no statistical difference among the groups (Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/lap). All cases were scheduled electively after an appropriate informed consent. The overall mean operative time was 65 minutes (range 42–105), with Group A of 70 minutes, Group B of 65 minutes, and Group C of 58 minutes (P = .58) (Supplementary Fig. S1 shows an overall progressive downtrend in the operative time as the operator gained technical experience). All cases were completed laparoscopically without conversion to a three-port, conventional four-port, or open cholecystectomy. Estimated blood loss was less than 50 mL in all of the cases. Intraoperative cholangiography was not necessary in any of these patients. There were no intra- or postoperative complications. There were no injuries or clinically significant bleeding at the peritoneal anchoring sites after removal of the NovaTract anchors. All patients were discharged on the same day of their cholecystectomies. Final pathology reports were consistent with cholelithiasis and chronic cholecystitis. No complications were noted at the 2-week postoperative follow-up. All patients were able to fully resume their routine activities within 2 weeks of the cholecystectomy. No mortality was found in this series.
Discussion
Conventional four-port LC has been the cornerstone for treatment of gallbladder diseases after the first description of laparoscopic cholecystectomy in 1985.1,2 Subsequent large-scale studies reaffirmed this technique as the gold standard treatment of benign gallbladder pathologies.3,4 In the last several years, single-port LC gained significant publications based on its cosmesis advantage, which leaves a nearly scarless wound. However, the single-port technique has not been proven to provide consistent additional benefits such as reduced postoperative pain, fewer wound complications, shorter recovery, earlier return to work, and higher overall patient satisfaction.5–8 In a meta-analysis of 45 studies (total of 2626 patients), the rate of biliary tract injury was significantly higher in the single-port approach when compared with that of the conventional four port (0.72% versus 0.5%, respectively). 9 This has been attributed to difficulties in achieving a critical view of safety during dissection of the Calot triangle. This technical challenge is partly related to parallel instrumental alignment and loss of triangulation, which are commonly seen during the single-port laparoscopy.9–12 Single-port LC therefore did not maintain its traction as the preferred technique among general surgeons.
Two-port LC was subsequently developed with the aim to achieve comparable outcomes as those of the conventional LC, while providing the benefits of reduced port surgery. Lee et al. 2 published a comparative study of two-port versus standard four-port LC, which results in similar operative duration, conversion rates, total analgesic requirements, length of hospital stay, and rate of complications. There have been several alternative retraction methods described in the literature and released in the market that allow retraction of intra-abdominal organs while obviating placement of standard retraction ports. Each method has its disadvantages with variable degrees of retraction and exposure success. Suboptimal retraction in a commonly performed procedure (such as LC) is oftentimes tolerated by experienced operators, as long as the operation could still be accomplished safely and efficiently. Several minimally invasive retraction methods such as transabdominal stay sutures, transabdominal endoloop, Magnetic Anchoring and Guidance System (MAGS), Endograb™, VERSA Lifter™, and modified laparoscopic bulldog clamp have been used in clinical practice.13–18
The transabdominal stay sutures are placed through the fundus and infundibulum of the gallbladder using straight Keith needles and then transabdominally externalized to allow continuous extracorporeal adjustments and manipulations. This retraction method only leaves negligible puncture marks where the needles are passed through the skin. However, there are several anatomical limitations associated with this method. The straight Keith needles and stay sutures must be passed/placed inferior to the rib cage to avoid entering the thoracic cavity, which could potentially create a right pneumothorax. This kind of stay suture placement leads to an anterior–inferior retraction of the gallbladder fundus, rather than an anterosuperior fundal retraction, which is the goal during LC. A potential gallbladder wall tear with subsequent intraperitoneal bile leakage and gallstone spillage as the needle is passed through the gallbladder wall is the main issue with this retraction technique. In addition, sudden loss of tension on the gallbladder when the stay sutures pull through may adversely affect the dissection. 13 Concerns have also been raised in cases of LC performed for large gallbladder polyps or porcelain gallbladders, where the potential presence of occult cholangiocarcinoma could not be ignored. Tian et al. reported their experience with 107 patients who underwent two-port laparoscopic cholecystectomy using the suture retraction technique. 14 The two-port LC provides similar outcomes without perioperative complications when compared with those of the conventional four-port method. Approximately, in 7.5% of cases, however, a placement of an additional port to assist with retraction and dissection of pericholecystic adhesions was required.
Transabdominal endoloop has been reported by Uras et al. 13 and Schlager et al. 15 to be useful in reduced port LC. The endoloop (Ethicon Endo-Surgery, Cincinnati, OH) is introduced through a 5-mm port and placed at the gallbladder fundus. Conceptually, it is similar to the transabdominal stay sutures without risks of gallbladder wall tear and subsequent bile and gallstone spillage. Inability to provide anterosuperior fundal retraction because it must also be introduced inferior to the rib cage is a major disadvantage, similar to that of the transabdominal stay suture method. In addition, fastening of the endoloops may prove very challenging in cases of scarred, edematous, distended, or intrahepatic gallbladder. In such cases, the gallbladder fundus must be separated from the liver bed in an antegrade manner to create a suitable tip for placement of the endoloop. This maneuver may increase the operative time and potentiate bleeding complication from the liver bed.
MAGS was developed by the groups of Scott et al. in 2001, which used intra-abdominal magnetically anchored instruments to perform trocar sparing laparoscopic surgery. 16 The MAGS uses two internal neodymium–iron–boron magnetic platforms, which are introduced into the abdomen through a 12-mm port. The internal platforms are magnetically anchored to the external platform on the patient's skin and are capable of use for intraoperative manipulations.16,17 Aside from issues of cost and its associated learning curve, a significant obstacle to widespread use of MAGS is the exponential decrease in magnetic couple strength as a function of distance (i.e., thickness of abdominal wall in morbidly obese patients). At the current time, the magnetic retraction system can only be used for tissue thickness <1.5 cm, thereby restricting its use mainly to thin and pediatric patients. 17 This is a major drawback since the majority of gallbladder pathologies are seen in obese populations.
The Endograb (Virtual Ports, Misgav, Israel) is an internally anchored retracting device that can be introduced into the abdomen through a 5-mm port. 15 Once deployed, one of the two gasping ends is attached to the gallbladder, while the other is anchored to the abdominal wall. This device allows anterosuperior placement of anchor above the costal margin, thereby allowing appropriate retraction mimicking conventional multiport LC. Retraction can be adjusted repeatedly throughout the operation by relocating the abdominal wall anchor to different sites. Schlager et al. 15 reported average operative time of 136 minutes with one cystic duct stump leak and one conversion to four-port technique during laparoscopic single-incision cholecystectomy in 20 patients.
Using the similar concept of Endograb, Colon et al. 18 described a novel use of modified laparoscopic bulldog clamp fitted with a small metal hook during a single-site LC for symptomatic cholelithiasis. The operative time was 120 minutes without intraoperative complications. VERSA Lifter (Surgical Perspective SAS, Strasbourg, France) is another internal adjustable retractor utilizing a pulley system described by Dhumane et al. 19 One clip is placed on the gallbladder fundus and the other is anchored to the anterior abdominal wall peritoneum. They concluded that the system is efficient, ergonomic, easy to use, and the spring-toothed design of the clips allows for a strong but atraumatic grip of the organs of interest.
The NovaTract dynamic laparoscopic internal retractor was designed to refine the previously described retraction methods. The ability of this system to accomplish reliable anterosuperior retraction of the gallbladder fundus with easily adjusted traction force during LC is an advantage. Because it is internally deployed, it can be placed high up on the anterior rib cage just below the diaphragm without concerns of creating right-sided pneumothorax. Simple positional adjustments of the abdominal wall anchor (frequency 0–1/case) and the atraumatic toothed grasper (frequency 0–2/case) are sometimes necessary to achieve optimum target organ retraction and/or to improve visualization. This did not change over the course of the three groups. We have now performed 18 initial cases of two-port LC using the internal retractor system. High BMI is not a contraindication for using the NovaTract. In our initial experience, we have performed two-port LC in obese patients with BMI above 35 mg/m2 without significant technical difficulties. The overall mean operative time was comparable with that of conventional four-port LC. As we gained more experience with this system, our operative time gradually decreased from 70 minutes in the first six patients (Group A) to 58 minutes in the last six patients (Group C). Despite no statistically significant differences found among the groups, improvements in the operative time suggest the presence of a mild learning curve. No patients required placement of an additional port or conversion to open cholecystectomy. No intra- or postoperative complications were seen, which supports the safety of the NovaTract retraction system. Even though the NovaTract dynamic laparoscopic internal retractor can be delivered through a 5-mm working port, in our cases, we used an 11-mm working port for specimen retrieval/extraction utilizing an Endo Catch device. This specimen retrieval system requires at least a 10-mm-diameter port. The NovaTract dynamic laparoscopic internal retractor could also be easily applied to other laparoscopic procedures such as colon resections, gastrectomy, or minimally invasive solid organ removal. We believe that this internal retraction system is a valuable addition to our minimally invasive surgical toolbox. The internal retraction system can also prove to be very useful when a suboptimal retraction or visualization is encountered intraoperatively or when reduced-port laparoscopy is desired by the patients. Further investigations with a larger number of patients are needed to establish definitive advantages and outcome–cost relationship of the NovaTract internal retraction system in clinical surgery practice.
Conclusions
The NovaTract Laparoscopic Dynamic Retractor appears to have met the initial objectives. It is safe and easy to use with a minimal learning curve, reflected by standard operative time for an LC using only two ports. It allows the surgical approach to mimic the conventional laparoscopic techniques, while eliminating dedicated right upper quadrant retraction ports.
Footnotes
Disclosure Statement
The senior author Dr. K.E.R. is an inventor of this device.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.