
Abstract
Abstract
Background:
After reports on laparoendoscopic single-site (LESS) cholecystectomy, concerns have been raised over the level of difficulty and a potential increase in complications when moving away from conventional gold standard multiport laparoscopy due to incomplete exposure and larger umbilical incisions. With continued development of technique and technology, it has now become possible to fully replicate this gold standard procedure through an LESS approach. First experiences with the newly developed technique and instrument are reported.
Methods:
Fifteen patients presenting with cholelithiasis without signs of inflammation were operated using all surgical steps considered appropriate for the conventional four-port laparoscopic approach, but applied through a single access device. Operation-centered outcomes are presented.
Results:
There were no peri- or postoperative complications. Mean operating time was 32.3 minutes. No conversion to regular laparoscopy was required. The critical view of safety was achieved in all cases. Mean skin incision length was 2.2 cm.
Conclusion:
The application of a standardized technique combined with the use of a four-port LESS device allows us to perform LESS cholecystectomy, giving us a correct exposure of the structures and without increasing the mean operating time combining previously reported advantages of LESS. A universal trait of any new technique should be safety and reproducibility. This will enhance its applicability by large number of surgeons and to large number of patients requiring cholecystectomy.
Introduction
L
In addition to the four-port cholecystectomy, surgeons have been looking to minimize surgical trauma even further by reducing the number of ports needed from four to three. More recently this procedure is now routinely being performed through a single umbilical incision starting with Navarra et al. 2 Although reports on this approach indicate comparable complication rates so far following laparoendoscopic single-site (LESS) surgery of the gallbladder, it is more challenging than conventional laparoscopy. One retracting instrument and triangulation are sacrificed to complete the procedure through one small umbilical incision, while at the same time the range of movement is limited.
The only way to avoid an increase in complications is to adhere to the surgically accepted principles for laparoscopic cholecystectomy. The concept of the critical view of safety for instance improves safety for both experienced laparoscopists and trainees alike and should not be abandoned.3,4
This article is the first description of a series of cases using an LESS technique that fully replicates the conventional laparoscopic technique, with complete retraction of the gallbladder and complete exposure of Calot's triangle using four laparoscopic instruments and a new dedicated access device, through an incision size that is comparable in size to a regular Hasson trocar.
Methods
Patients were selected based on having no previous upper abdominal surgery, and having no signs of acute inflammation. Patients were consented according to requirements by our Internal Review Board.
Patients were placed in supine position with surgeon and assistant standing on the patient's left side, just like in conventional laparoscopy. To improve ergonomics, the patient was positioned slightly off-center toward the left side of the operating table.
Draping is as per usual, but extra care was taken to scrub the umbilicus well. Intraperitoneal access was created transumbilically making a transverse skin incision well within the umbilical ring and a transverse fascial incision of 1.5 cm. After introduction of the TriPort+ access device (Olympus co., Tokyo, Japan), the operating table was placed in the usual anti-Trendelenburg position tilted to the left. Instruments used were regular readily available bariatric length reusable graspers, dissectors, and scissors, with the exception of one novel reusable grasper that had a fixed 70° curve at the distal end. As per our usual laparoscopic cholecystectomy, the assistant operated a 5 mm 30° laparoscope and pushed the fundus of the gallbladder upward retracting the liver. The surgeon manipulated the infundibulum using the curved instrument alternating exposure of the lateral and medial side of the gallbladder. The curve prevents internal instrument clashes. This leaves the fourth valve of the access device for the surgeon to use his dissecting instrument of choice. A generous release of the gallbladder was performed by incising the peritoneum on both sides of the gallbladder, providing mobility needed to comfortably swing the gallbladder to either side. As with conventional laparoscopy, each instrument was used through a specific valve, and it was this choreography of instruments that enabled retraction and dissection using three instruments and a laparoscope through a single 1.5 cm fascial incision. The use of the valves on the access device is explained in Figure 1.
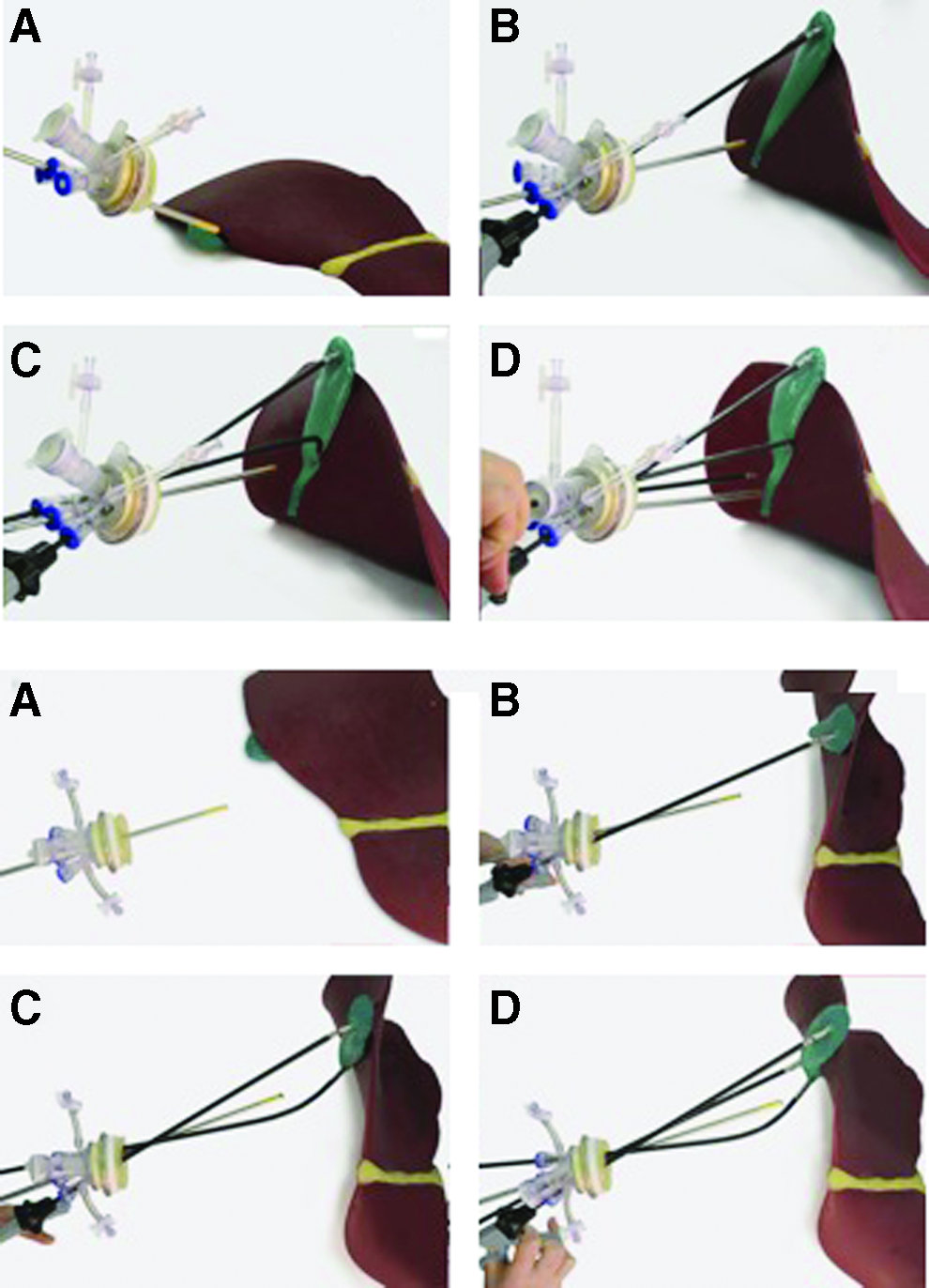
Side and top views to show step by step our standardized technique.
All parameters, such as operative times, peri- and postoperative complications, discharge, and so on, were recorded prospectively.
Results
Fifteen patients were operated by one team of surgeons. Indications for cholecystectomy were mainly billiary colics, one case of previous choledocholithiasis treated by endoscopic retrograde cholangiopancreatography, and one case of previous pancreatitis. None of the patients had a history of cholecystitis. Mean age of the group of patients was 39 years. Mean body mass index was 27.1. The group consisted of 14 females and 1 male.
All procedures were completed successfully. There were no perioperative complications such as gallbladder perforation and bile leakage of bleeding. Mean operative time was 32.3 ± 12.1 minutes (skin-to-skin time). Although we insist on introducing a second laparoscopic port (“conversion to laparoscopy”) in case of surgical difficulties or incomplete exposure of the surgical field, no additional ports were required in any of these patients. In all cases, the critical view of safety was confirmed by both operating and assisting surgeons.
As is the case of conventional laparoscopy in our institution, all patients were discharged on day 1 postoperatively. There were no postoperative complications such as wound infection, bleeding, complications from general anesthesia, leakage of bile ducts, cardiac, vascular, or thoracic diseases, and none of them required readmissions.
Discussion
Although the authors are laparoscopic surgeons experienced in LESS colorectal and LESS bariatric procedures, gallbladder surgery at our institution was performed by minilaparoscopy until now. Previous experiences with LESS cholecystectomy required an incision larger than 2–2.5 cm, and the lack of a fourth instrument introduced through the single incision resulted in either unsatisfactory exposure of the surgical field or a transabdominal suture passing through the gallbladder. In our opinion, minilaparoscopic resection used to be superior because of these reasons. Introduction of a new access device and dedicated instrument has enabled the development of a four-instrument technique applied through a single incision no larger than 1.5 cm, mimicking all steps we are comfortable with in conventional laparoscopic cholecystectomy and resulting in a proper critical view of safety in all cases.
Operating times in the main series in the literature decreased considerably after the first cases, with more recent series showing times comparable to conventional laparoscopic cholecystectomy, although still being longer. Differences may be based on surgeons being significantly less experienced in the LESS procedure compared with conventional laparoscopic resection. Besides surgical experience with LESS, it should be noted that now having a device that accommodates up to four instruments (including a laparoscope) instead of three further reduces operating time (Table 1).4–17
LC, conventional laparoscopy.
More experience is needed and more data required to define the place of LESS cholecystectomy in the repertoire of laparoscopic surgeons, but at least now there is a method that seems to consistently be able to achieve the level of dissection and exposure that may have been lacking in reduced port surgery. It provides an excellent basis for standardization needed to perform and teach this technique safely. Although all our patients were extremely pleased with the results of the procedures, data are required on patient-centered outcomes from randomized trials. Only now are results from trials becoming available, and randomized results appear to show advantages of LESS cholecystectomy over laparoscopic cholecystectomy.5,6 As with any new technique, LESS has been the domain of a select group of experienced laparoscopic surgeons, which makes results difficult to generalize especially since for many hospitals cholecystectomy is a procedure performed by more junior surgeons. Our current focus is on studying the learning curve and establishes whether the technique and skills described here can be transferred safely and consistently to surgical residents in a controlled manner.
Footnotes
Disclosure Statement
No competing financial interests exist.