
Abstract
Abstract
Background:
Generally, single-incision laparoscopic cholecystectomy (SILC) requires the use of articulating devices or additional trocars because of the technical difficulties caused by the lack of ergonomics. We developed a novel procedure comprising mainly two simple ideas, “the teres hanging technique combined with fundus-first, dome-down separation,” which mainly uses conventional rigid laparoscopic instruments. In this study, we demonstrated our technique and retrospectively evaluated the clinical outcomes.
Subjects and Methods:
Three trocars were set through a 2.0-cm transumbilical minilaparotomy that was covered with an EZ Access™ combined with a lap protector. To create an adequate surgical field, the teres ligament was laparoscopically hung up with a suture on a straight needle. The gall bladder was then dissected through the fundus to the neck using rigid laparoscopic instruments without any additional trocars. At our institution, 18 consecutive patients underwent SILC using our technique from January 2014 to August 2015. Each patient had a symptomatic gallbladder (GB) stone or polyp. All operations were performed by surgeons who had never performed SILC until this study.
Results:
In all operations, our technique was successfully completed without GB perforation or other intraoperative complications. Additional trocars or open laparotomy were not required. The median operation time was 79 minutes, and blood loss was negligible. No postoperative complications were encountered.
Conclusions:
Our novel procedure is safe and feasible. Even for surgeons who have never performed SILC before, our technique may become a standard for benign GB disease without requiring the use of articulating devices or additional trocars.
Introduction
L
Subjects and Methods
Patients
We retrospectively reviewed 18 consecutive patients who had undergone SILC using our technique at our institution from January 2014 to August 2015. Every patient had a symptomatic GB stone or benign GB polyp and hoped to undergo a single-incision laparoscopic treatment. The exclusion criteria included the following: (1) patients with Mirizzi's syndrome, (2) patients with suspected common bile duct stones, (3) patients with a suspected malignancy, (4) patients who had undergone previous major upper abdominal surgery, and (5) patients with severe cholangitis or cholecystitis. All operations were performed by general surgeons who had never performed SILC until this study. Each patient gave written informed consent to be treated with the following procedure. The study was approved by the institutional ethics board at our institution.
Operative procedure
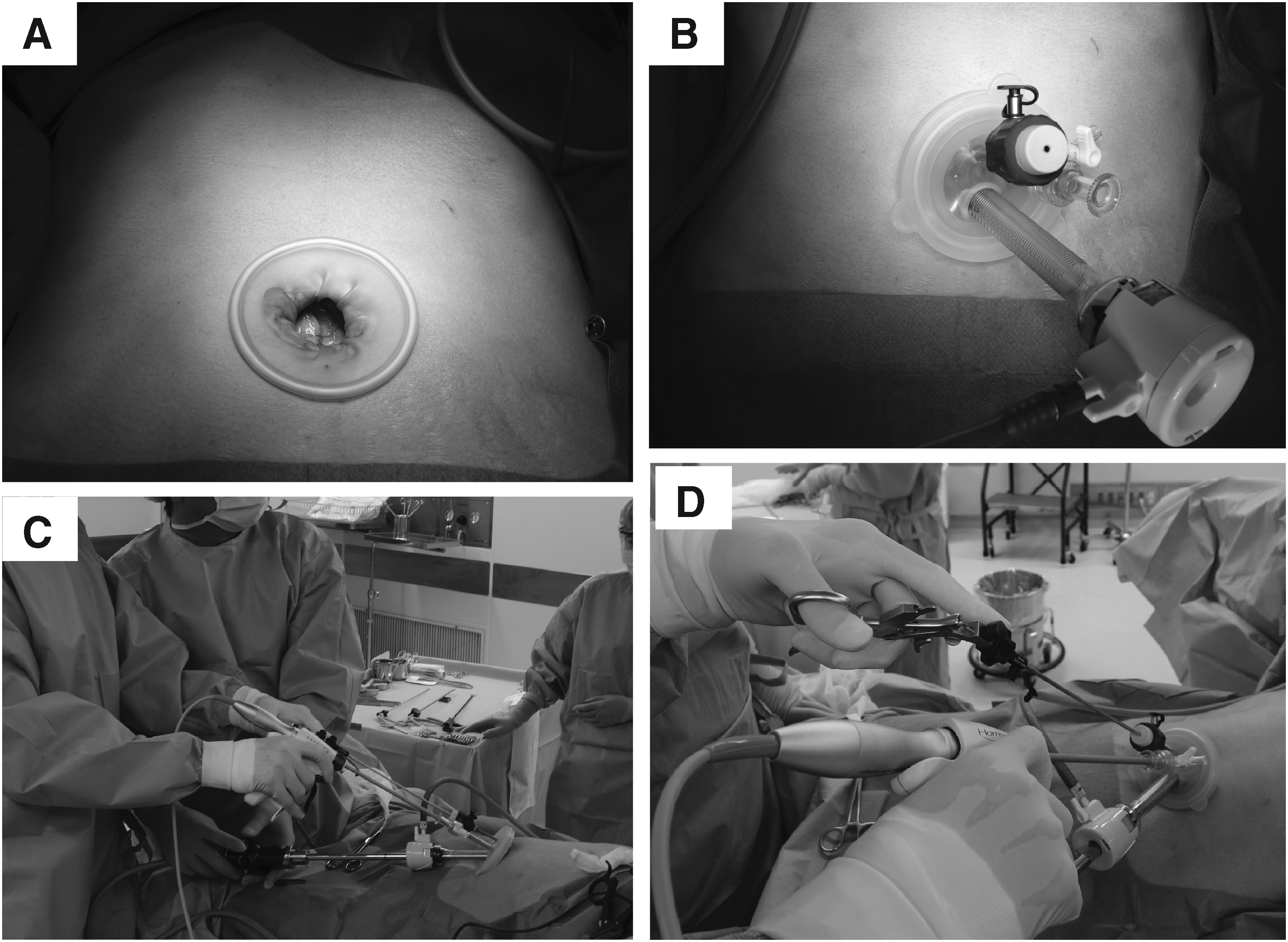
The patient was placed in the supine position with his/her legs spread. A 2.0-cm transumbilical minilaparotomy was created. A lap protector mini (LP; Hakkou-Shoji) was placed around the minilaparotomy (Fig. 1A) for wound protection. An EZ Access™ (Hakkou-Shoji) was mounted to the LP, and a 12-mm trocar (Kii Access System; Applied Medical Resources Corporation), a 5-mm trocar (Hakkou-Shoji), and a 3-mm reusable trocar (Karl Storz) were placed on it (Fig. 1B); CO2 insufflation was then started. The pressure for the pneumoperitoneum was set at 8 mmHg. The operating surgeon stood on the left side of the patient, with the scope operator between the patient's legs (Fig. 1C). A 10-mm flexible telescope (Olympus) was introduced through the 12-mm trocar. The operating surgeons always used straight rigid instruments as follows: reusable 5-mm atraumatic graspers (Karl Storz), an electrocautery, and a HARMONIC ACE™ (Johnson and Johnson), which were managed in the right hand for the main surgery, while the left hand was used for traction with a 3-mm grasper (Fig. 1D). Intraoperative cholangiograms were not performed on any patient.
SILC port site and extracorporeal view using the teres hanging technique combined with fundus-first, dome-down separation
The teres hanging technique
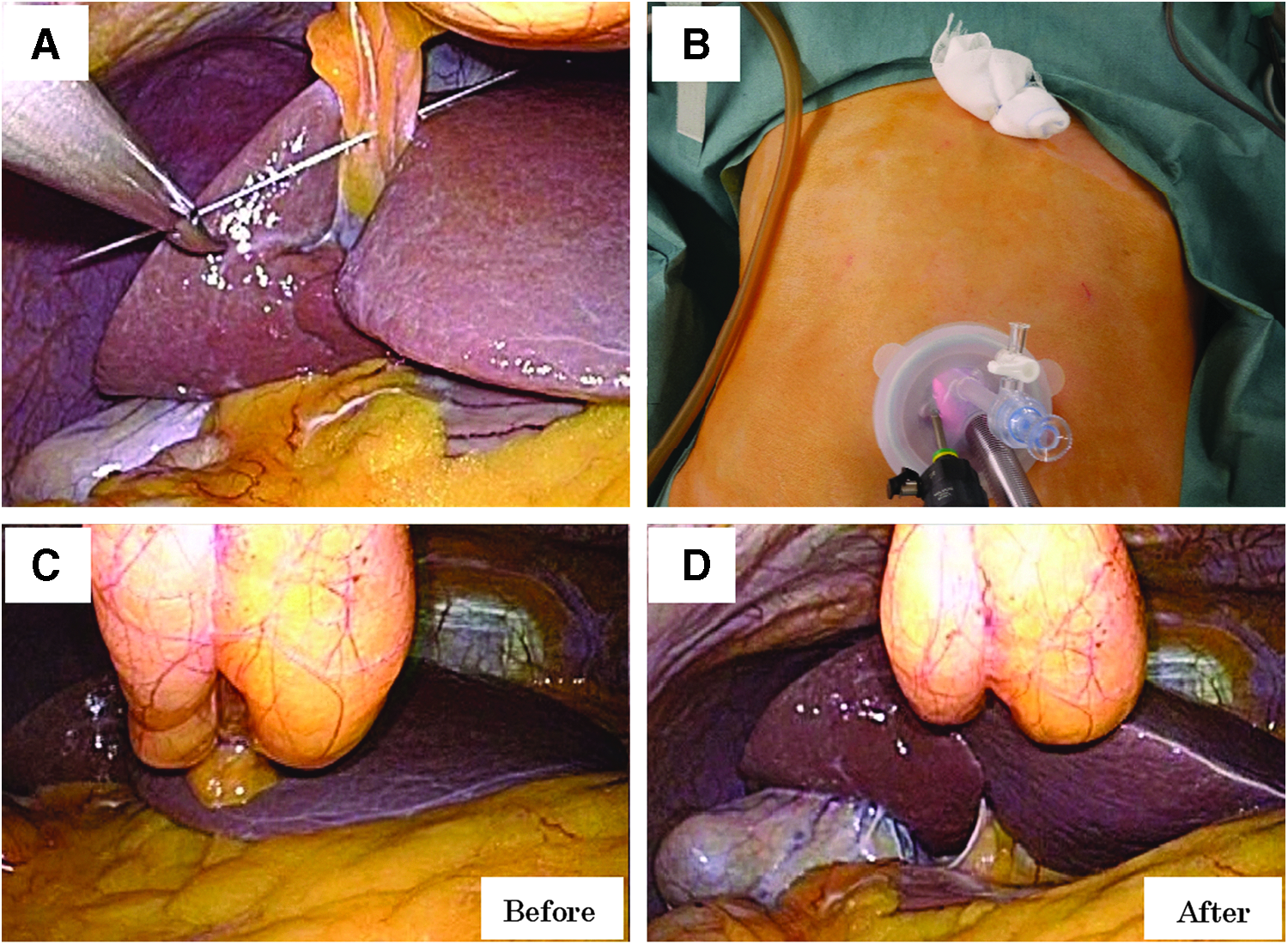
First, a 2/0 polypropylene suture on a 70-mm straight cutting needle (Johnson and Johnson) was vertically introduced through the subxiphoid abdominal wall under direct laparoscopic surveillance. The optimum site for the insertion of the needle is as cranial as possible to effectively elevate the inferior surface of the liver.
Second, the needle was taken down with a laparoscopic needle holder and passed through the teres ligament as close to its attachment point as possible to elevate the inferior surface of the liver (Fig. 2A). The needle was passed back up through the abdominal wall and then passed out on the outside of the abdomen. A tight extracorporeal ligation of this suture was performed while placing a piece of gauze between its knot and the skin (Fig. 2B). With this tight hanging of the teres, the inferior surface of the liver was lifted to the anterior abdominal wall with the GB, consequently exposing Calot's triangle and ventrally stretching the liver bed (Fig. 2C, D).
The outline of the teres hanging technique
Third, the patient was then placed in the reverse Trendelenburg position with the right side up. In this body position, the hepatoduodenal ligament was caudally retracted by gravity. As a result, Calot's triangle was better visualized. We called this procedure “the teres hanging technique.”
Fundus-first, dome-down separation
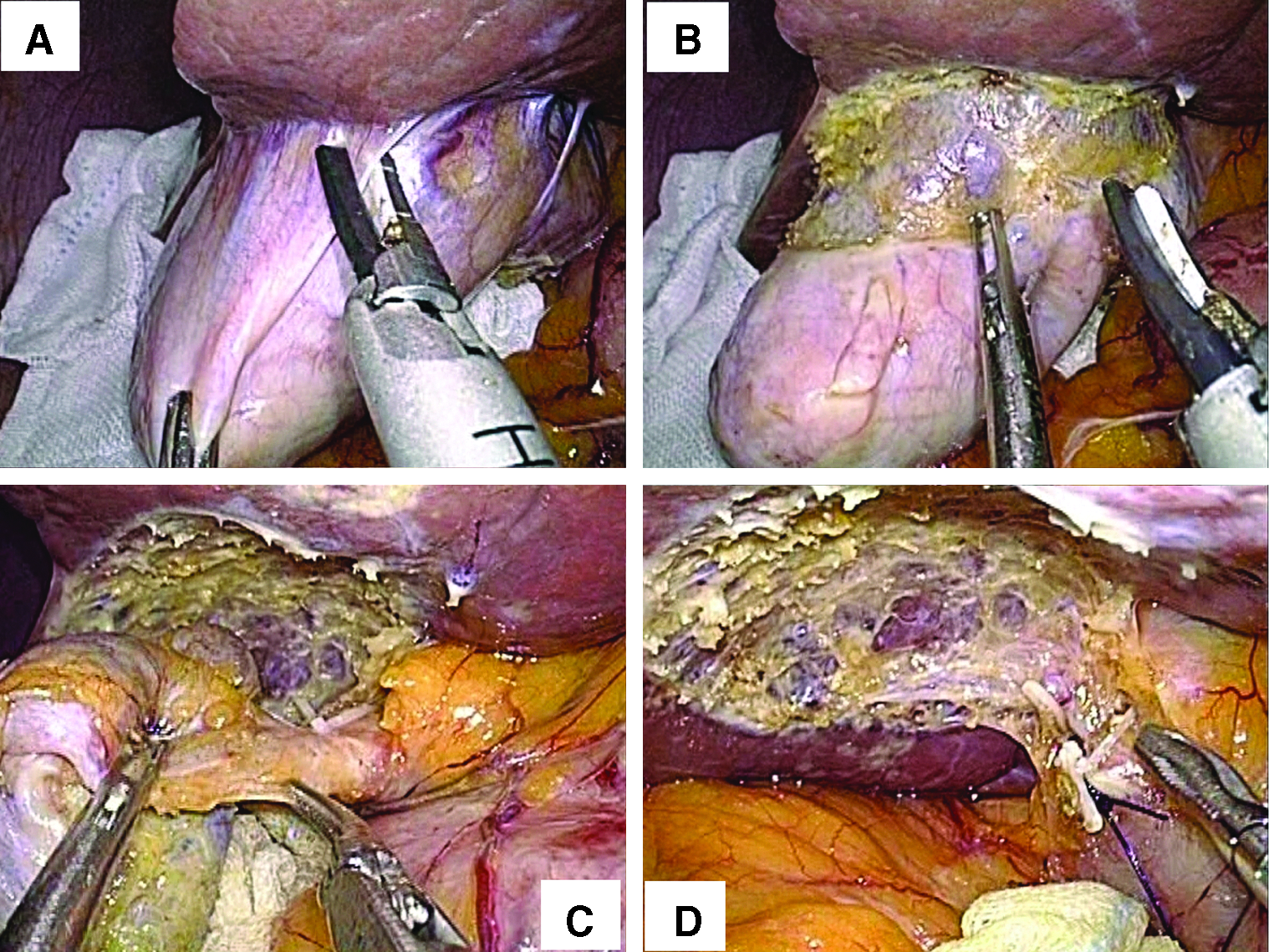
After the teres hanging, the GB was dissected free from the liver bed starting at the fundus toward the GB neck using a HARMONIC ACE or an electrocautery (Fig. 3A, B); we called this “fundus-first, dome-down separation”. 8 The cephalic traction and ventral stretching of the liver bed were maintained with the teres hanging technique. The caudal traction of the fundus was affected by gravity and the 3-mm grasper in the left hand. This “fundus-first, dome-down separation” prevented the surgeon's rigid instruments from clashing (Fig. 1D). After the GB separation until the GB neck was completed, Calot's triangle was dissected while still maintaining an adequate operative field with the teres hanging (Fig. 3C). Each cystic duct and artery were identified; “critical view of safety” was clipped using 5-mm Hem-o-lok® clips (Weck Closure Systems, Research Triangle Park) or the ENDOLOOP™ Ligature (Johnson and Johnson) and then divided in the conventional manner (Fig. 3D).
The outline of the fundus-first, dome-down separation cholecystectomy.
The GB was retrieved through the umbilical site protected by LP with the assistance of a grasper. An endopouch was not routinely used unless the GB was severely swollen and posed a risk of bile leakage. Finally, the umbilical wall incision was closed with 2/0 absorbable sutures and the skin was closed with 5/0 absorbable sutures.
Results
In all cases, SILC with “the teres hanging technique combined with fundus-first, dome-down separation” was successfully completed. There were no intraoperative complications such as GB perforation, massive bleeding, or injuries to organs (Table 1). The median operative time was 79 minutes (range, 53–157 minutes). The longest operative time was 157 minutes and involved two cases of acute cholecystitis. Three trocars were used only through the umbilical site in all cases; no additional trocars were required. No conversion to open laparotomy was required in any of the cases. All operations were completed with negligible blood loss. No postoperative complications were encountered, and all patients were postoperatively discharged within 4 days (Table 1).
BMI, body mass index; SILC, single-incision laparoscopic cholecystectomy.
The teres hanging completion time, from the introduction of the straight needle until tight ligation, was 104 seconds (range 70–157 seconds) (Table 1).
Discussion
In this study, we made two important clinical observations. First, the teres hanging technique combined with the fundus-first, dome-down separation for SILC is safe and feasible. Second, the teres hanging process with a straight needle is simple, safe, and not time consuming.
SILC has become more popular with the improvements in surgical techniques and instruments. However, we believe that it has three major technical problems caused by the lack of ergonomics. First problem, it is difficult to adequately create the surgical field, including Calot's triangle. To overcome this difficulty, many authors have reported that additional trocars should be introduced into another site to assist with GB retraction.9–13 However, this procedure would not be “SILC”; moreover, additional trocars are associated with inferior postoperative pain and cosmetic outcomes compared with those of SILC. Second problem, straight rigid instruments usually interfere with each other both intra-abdominally and extra-abdominally. 14 This interference, so-called “clashing,” is rather uncomfortable. 15 Several authors have reported that the use of articulating instruments can effectively avoid clashing.2,7,10,16–24 However, some surgeons have also noted discomfort while using articulating instruments because the right hand had to operate the left-sided instrument at the GB site, which is known as the “mirror effect”. 15 In addition, most articulating instruments are expensive and not reusable. Third problem, the principle of the SILC procedure is the same as that of the traditional four-port approach in most technical reports. 1 Generally, to try to produce the desired exposure around Calot's triangle for SILC, the fundus is cranially pushed away with a left hand grasper.1,7,18,25,26 Under this surgical field, each cystic duct and cystic artery are first divided and then the antegrade cholecystectomy, from the neck through to the fundus, is commonly performed.1,7,15,25–27 We believe that this antegrade cholecystectomy for SILC has two drawbacks. First, while pushing the fundus cranially using only an umbilical grasper, the cystic duct tends to be parallel to the common bile duct. As a result, the cystic duct might be mistaken for the common bile duct. In fact, SILC has been associated with a higher bile duct injury rate. 6 Second, umbilical graspers increase the risk of GB perforation during the push, as if the tip of the grasper stabbed into it. The most common intraoperative complications for SILC are reportedly GB perforation/bile spillage (2.2%). 15
To overcome these three major technical problems for SILC, we developed a novel procedure called the “teres hanging technique combined with fundus-first, dome-down separation.” This technique, which mainly uses conventional rigid instruments and does not require additional trocars, articulating instruments, or GB stay sutures, has the following three advantages. First advantage, “the teres hanging technique” lifts the inferior surface of the liver with the GB and ventrally stretches the liver bed. As a result, we succeeded in achieving a suitable surgical field, including Calot's triangle (Fig. 2D).
Second advantage, “fundus-first, dome-down separation” allows the surgical triangulation, including the liver elevation by teres hanging, left caudal retraction of the hepatoduodenal ligament by the reverse Trendelenburg position, and right caudal fundic retraction by the surgeon's left hand 3-mm grasper (Fig. 3). As the fundus is separated from the liver bed, the GB is simultaneously and progressively retracted caudally under its own weight, thus further improving the surgical triangulation (Fig. 3B). As a result, the dome-down separation causes little clashing because there is no need to swing the left hand grasper, that is, it is sufficient for the surgeon's left hand to just touch and gently withdraw the GB (Fig. 3). Moreover, it is easy to separate the GB from the liver bed, which is kept stretched by the teres hanging technique, particularly in the dome-down manner (Fig. 3A, B).
To minimize instrumental clashing, we used a 3-mm thin grasper, which had a more reliable stiff shaft, and a 10-mm flexible telescope. The flexible telescope, which is commonly used in Japan, as well as a 30 or 45-degree rigid telescope, allowed the detection of moving angles between the operating surgeon and the scope operator (Fig. 1C). The majority of reported series on SILC have used articulating or curved instruments and their recommendations included these instruments.19–23,25,26 Rigid instruments have been less frequently used.28–30 In fact, one report suggested that if more than two rigid instruments were placed through the umbilicus, causing instrumental clashing, surgeons should shift to one rigid and one articulating instrument. 31 We do not agree with these opinions because we believe that these technical problems can be resolved by our present technique.
Third advantage, dome-down separation creates a 360-degree view of the GB-cystic duct junction, reducing the risk of any anatomic misidentification. 8 The inferior surface of the liver is elevated by the teres hanging, and the surgical field around Calot's triangle is still maintained (Fig. 3C). Moreover, the cystic duct is readily and simultaneously retracted caudally by the GB's own weight; therefore, it does not run parallel to the common bile duct. As a result, surgeons are less likely to mistake the cystic duct for the common bile duct (Fig. 3C). Similarly, the cystic artery in Calot's triangle is also easily detected and isolated.
Thanks to these three advantages, our teres hanging technique always achieved exposure of Calot's triangle, and the combination with “fundus-first, dome-down separation” was useful for more meticulous and safe dissection without instrumental clashing. In addition, our technique did not require articulating devices or additional trocars. There were no cases in which we had difficulty creating an operative field. Additional trocars or conversion to open laparotomy were not required. No bile duct injury, GB perforation, or bile leakage was observed in our series. The amount of bleeding was negligible in all cases, and our median operation time was comparable with those of other SILC reports9,14,32–34 with consideration of the learning curve.
For obese and morbidly obese patients, the teres hanging technique may be less effective for achieving the surgical field around Calot's triangle. Initially, it is not always necessary to completely expose the GB neck. At the end of dome-down separation, Calot's triangle can be visualized by the assistance of the left hand grasper, which is freed by the caudal retraction of the dissected cystic duct by gravity.
In our study, we did not attempt to perform intraoperative cholangiography. However, we believe that our present technique makes it possible to perform intraoperative cholangiography without requiring any additional trocars within our preoperative indication. At the end of dome-down separation, both hands are nearly unoccupied as previously described. Moreover, as the operative point approaches the umbilical site, the moving angle of both hands spreads out progressively, thus reducing instrumental clashing. Considering this evidence, tube cannulation into the cystic duct and common bile duct exploration may not be technically demanding using our technique.
The teres hanging procedure with a straight needle under SILC was not complicated or time consuming, and the procedure did not require special devices. Our teres hanging procedure did not cause any intraoperative complications such as bleeding or other organ injury, and the completion time was 104 seconds (median) (Table 1). We used a 70-mm straight needle. We believe that a shorter straight needle would have made our teres hanging procedure easier to perform. The scars at the subxiphoid and the umbilicus were no longer visible 1 month postsurgery (Fig. 4).
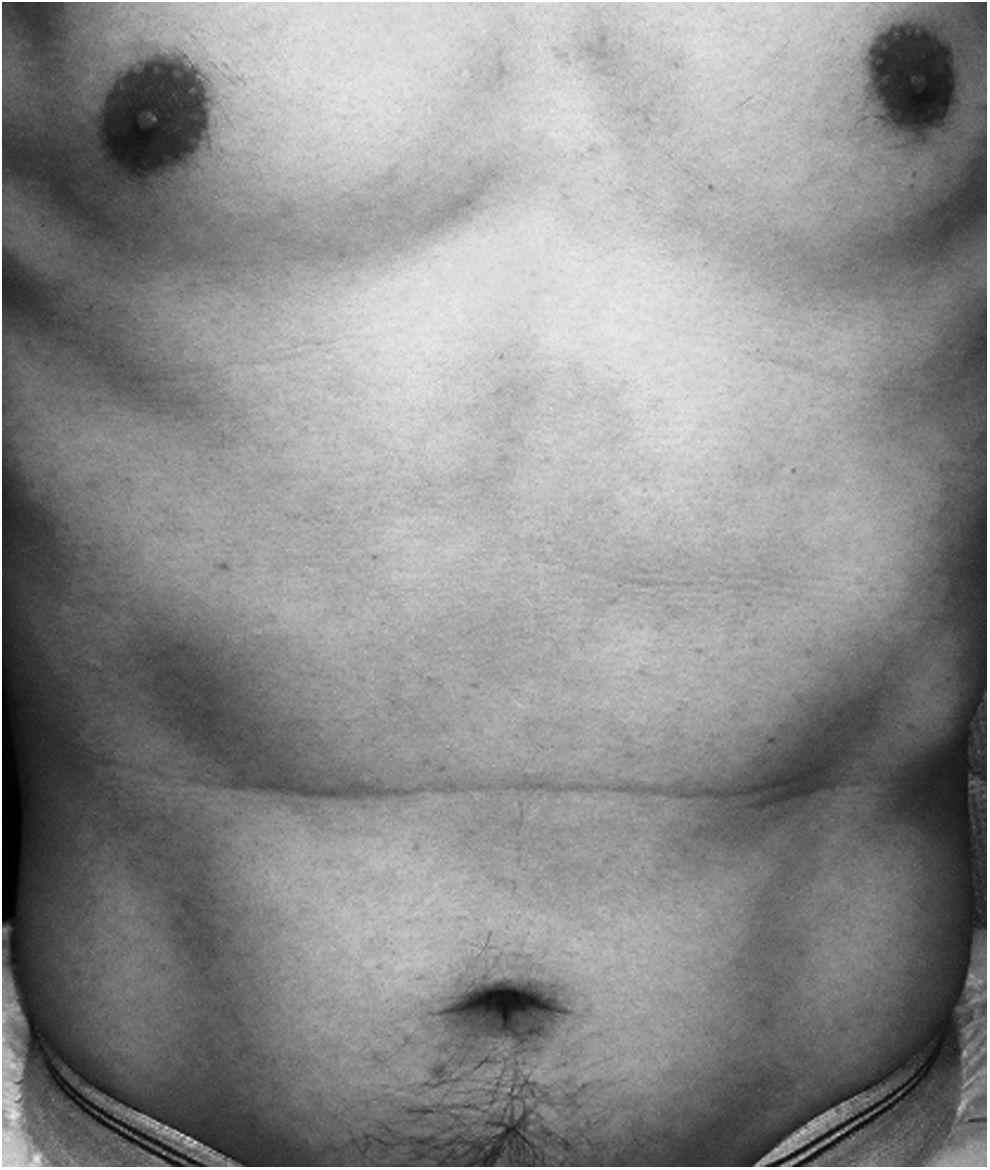
Umbilicus and subxiphoid scars at 4 weeks.
The use of an additional 2-mm or 3-mm thin grasper during SILC has acceptable cosmetic outcomes and would have allowed more advanced and comfortable operative conditions in our technique. However, it has also been reported3–5 that pure SILC (umbilical incision only) reduces wound pain, improves cosmesis, results in an expedited return to routine activity, and has higher patient satisfaction compared with SILC using additional thin trocars. Moreover, to overcome the technical difficulties of SILC, many new techniques and devices have been developed. Our present technique may lead to progress in minimally invasive surgery.
In the present study, every SILC was successfully performed even by surgeons who had never performed SILC before. Our novel technique made SILC as simple as a conventional four-port LC and did not require special training. However, some expensive disposable instruments were used. In the future, it is expected that our present technique will be performed using only inexpensive instruments without a loss of safety.
This study had several limitations. The sample size of the study was small. There was no control group, and the study was not randomized. In addition, this report represented a selected group of patients and excluded those with severe acute cholecystitis. However, we believe that our technique significantly expands the indications for SILC.
In conclusion, we developed a novel procedure for SILC, “the teres hanging technique combined with fundus-first, dome-down separation,” with a straight needle, which is safe, feasible, and not time consuming. Although further work in the form of randomized controlled trials is required to evaluate the potential benefit of our novel technique, we believe that the teres hanging technique combined with fundus-first, dome-down separation for SILC may become a primary treatment for benign GB disease even for inexperienced surgeons.
Footnotes
Disclosure Statement
No competing financial interests exist.