
Abstract
Abstract
Background and Purpose:
Bilateral adrenalectomy or unilateral adrenalectomy and contralateral partial adrenalectomy are indicated for the treatment of ACTH-independent macronodular adrenal hyperplasia. Independent of the surgical procedure, the prognosis is poor. This article discusses a new treatment method and its efficacy for treating nodular adrenal hyperplasia.
Methods:
We performed a retrospective review of the medical records of 12 patients operated on between January 2008 and October 2014 at the First Affiliated Hospital of Zhengzhou University. All patients were treated by laparoscopic subcutaneous transposition of a pedicled adrenal. We performed postoperative monitoring of patients, including clinical symptoms and 24-hour levels of serum-free and urinary-free cortisol.
Results:
All 12 patients were pathologically confirmed to have nodular adrenal hyperplasia and were followed for an average of 45.5 months (range 24–60 months). The clinical symptoms of all patients disappeared, and the 24-hour plasma-free cortisol and urinary-free cortisol levels were within the normal range.
Conclusions:
Laparoscopic subcutaneous transposition of a pedicled adrenal is a new and effective method for treating bilateral macronodular adrenal hyperplasia and can achieve long-term remission of Cushing's syndrome.
Introduction
M
Since the 1990s, we have been performing this surgery; it is not laparoscopic, but rather open surgery. After many years of clinical validation, we suggest that this surgical procedure is safer and has a lower postoperative recurrence rate than bilateral adrenalectomy and unilateral adrenalectomy, but contralateral partial adrenalectomy.
Materials
Between January 2008 and October 2014, 12 patients went to the First Affiliated Hospital of Zhengzhou University for treatment of bilateral macronodular adrenal hyperplasia. Of these patients, there were 2 males and 10 females, aged 14–42 years (average 27.5 years). All patients had the clinical manifestations typical of CS (central obesity, moon face, and buffalo hump). In addition, there were 10 patients with hypertension, 8 female patients with menstrual disorders, and 2 male patients with sexual dysfunction.
All patients had preoperative levels of plasma-free cortisol, 24-hour urinary-free cortisol, and plasma ACTH measured (Table 2). The cortisone level of all patients could not be obtained from high- and low-dose dexamethasone suppression tests (Table 1). The results of computed tomography imaging examinations showed multiple nodules in both adrenals (Fig. 1), and a normal pituitary was seen in magnetic resonance imaging.

Computed tomography images. The white arrows point to the nodule of the adrenal gland.
cop, comparison; high, high-dose dexamethasone suppression test; low, low-dose dexamethasone suppression test; N, negative; R, result; Ufc, 24-hour urinary-free cortisol.
Ufc, the normal range (130–304 nmol/24 h); plasma ACTH, the normal range (EO = 7.3–63.6 ng/L, SXO = 4–33 ng/L); plasma-free cortisol, the normal range (EO = 172–537 μg/L, SXO = 64–327 μg/L).
EO, eight o'clock; m, month; SXO, sixteen o'clock; Ufc, 24-hour urinary-free cortisol.
Methods
Laparoscopic subcutaneous transposition of a pedicled adrenal was performed on all patients, as detailed in this section. The patient was initially placed in the supine position for intravenous access, induction of general anesthesia, and endotracheal intubation. The umbilicus was placed over the break in the operating table, and the patient was positioned in the modified right lateral decubitus position. An inflatable balloon was positioned under the patient at the level of the umbilicus; padding was used to support the buttocks and the dorsum, and all potential pressure points were cushioned.
After creating a left rectus abdominis flat umbilical incision of ∼1 cm, a 10-mm trocar was introduced through the incision, perpendicular to the abdominal wall. A connection to the pneumoperitoneum confirmed that the trocar was correctly placed inside the abdomen. The fiber optic was then introduced through the trocar after creating a left subclavian midline subcostal incision of about 0.5 cm and a 1-cm incision on the anterior axillary line and the iliac crest two fingerbreadths. Then, the 10-mm trocar and 5-mm trocar were placed, respectively (Fig. 2A). The splenorenal and lienocolic ligaments were incised, allowing the spleen and the tail of the pancreas to be separated from the upper pole of the kidney.
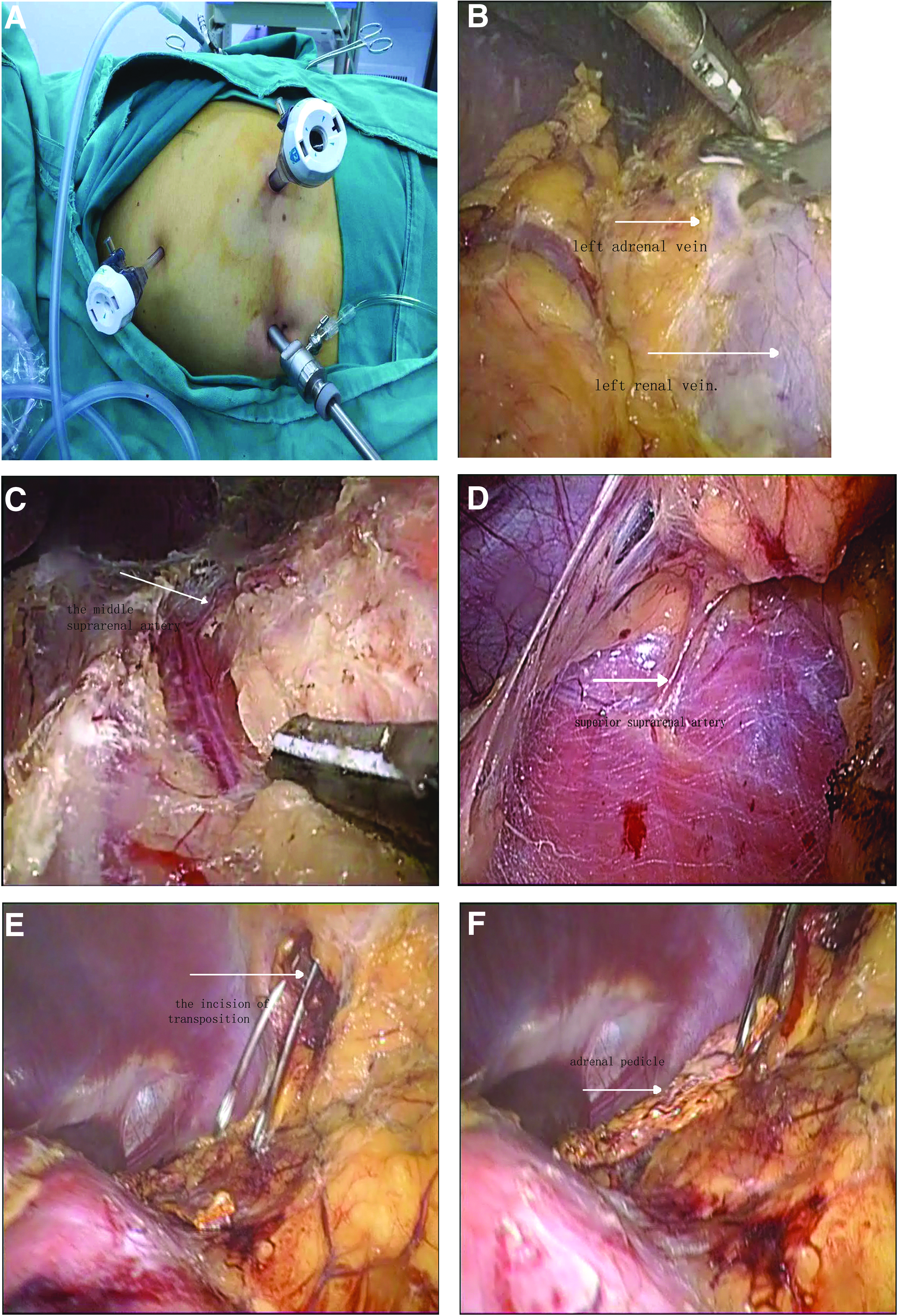
Illustrations of the operative procedures of the transposition:
The en bloc dissection of the colon, spleen, and pancreas must be completed for adequate exposure of the renal vein. Exposure and subsequent ligature of the left adrenal vein were then done (Fig. 2B). Gerota's fascia was gently peeled off circumferentially above the upper pole of the kidney, and mobilization of the left adrenal gland and ligation of the middle suprarenal artery and inferior suprarenal artery were completed (Fig. 2C). At this point of the dissection, care must be taken with the superior suprarenal artery and connective tissue surrounding the adrenal gland, which is connected to the diaphragm (Fig. 2D).
Half of the adrenal gland was removed and sent to the pathology laboratory; the pedicle should be kept at a length of 5–6 cm and a width of 2–3 cm. Making a posterior axillary line incision of about 2 cm between the 11 and the 12 intercostal, we then dissected the fatty tissue and intercostal muscles (Fig. 2E). The pedicle was clamped to the subcutaneous fat (Fig. 2F), and we then clamped the periadrenal fat to the peritoneum and sutured the incision. We treated the right adrenal gland with the same method after 1 month. The patient was given corticosteroids and immobilized for 2 weeks.
Results
All patients were followed up for 24–60 months. There were no deaths or recurrences, and the clinical symptoms (central obesity, moon face, and buffalo hump) of all patients disappeared. In addition, blood pressure and menstruation returned to normal. The results of the preoperative plasma-free cortisol, 24-hour urinary-free cortisol, and plasma ACTH assays are detailed in Table 2. All patients accepted abdominal CT 1 year after treatment. It showed the good, survived, transposition adrenal glands on the CT image (Fig. 3). Pathology of the resected glands revealed bilateral nodular adrenal hyperplasia.

Computed tomography images. One year after the transposition. The white arrows point to the transposition of the adrenal gland.
Discussion
CS results from chronic exposure to excessive concentrations of glucocorticoids and includes both corticotrophin-independent and corticotrophin-dependent diseases. Patients with untreated CS have a fivefold increased mortality rate and a mean survival time of 5 years from their initial presentation.1,10–13 Therefore, effective treatment is critical. This article focuses on a new treatment for corticotrophin-independent, bilateral nodular adrenal hyperplasia.
In the past, bilateral adrenalectomy was the treatment of choice, boasting a high success rate in reversing hypercortisolism.14,15 Eventually, however, it was found that there was a significant risk of developing Nelson's syndrome and patients have to take glucocorticoids for the rest of their life.3,8,16 Unilateral adrenalectomy and contralateral partial nephrectomy were proven to be better than bilateral adrenalectomy, but there is a lot of controversy about how much adrenal gland should be removed.6,10,17,18 At the same time, it often leads to disease recurrence and a difficult reoperation.
Subcutaneous transposition of a pedicled adrenal is our original procedure. Through this method, we have cured many patients. After many years of clinical validation, we suggest that the key factors for successful operation are as follows.
First, the choice of incision is very important. A suitable incision determines the success of the surgery; incision of the 11 and the 12 intercostal should be closer to the sacrospinalis, which makes it easy to pull a vascular pedicle. Second, the upper pole of the adrenal gland should not be dissected too much. Otherwise, it may damage the pedicle during the transposition of the adrenal, which is not conducive to survival. Third, care must be taken with the superior suprarenal artery, which is the main blood supply for the transposition of the adrenal. Fourth, the incision should be disinfected every 2 days to avoid wound infection, which will lead to adrenal necrosis.
It is generally believed that only one adrenal vein plays a major role.9,16,19 While the artery of the adrenal gland has accompanying veins, their function is secondary, and they are difficult to find due to their small diameter. The accompanying veins play an important role when the adrenal vein is ligated. Because the superior suprarenal artery is the main blood supply for the adrenal gland, we have retained this artery. These characteristics are the basis for survival of patients undergoing the transposition of their adrenal.
We suggest that subcutaneous transposition of a pedicled adrenal is an effective and safe alternative treatment for patients with nodular adrenal hyperplasia. There is some concern about the possibility of gradual growth of the transpositioned gland, with a parallel increase in cortisol secretion. Our experience does not support this concept; morphological studies did not show any significant enlargement in all patients 24–60 months after surgery. In addition, the 24-hour urinary cortisol levels stayed within the normal range in all patients. No adrenal enlargement was found in patients with subcutaneous transposition of a pedicled adrenal.
At our institution, we have seen a gradual shift from laparoscopic bilateral adrenalectomy to laparoscopic bilateral subcutaneous transposition of a pedicled adrenal for patients with nodular adrenal hyperplasia. Follow-up information was obtained for all patients. During the follow-up time, there were no deaths or recurrences, the clinical symptoms (central obesity, moon face, and buffalo hump) of all patients disappeared, and blood pressure and menstruation returned to normal. A second surgery to remove the transposed gland could be done if clinical symptoms recurred during follow-up, but long-term follow-up of all patients (mean = 45.5 months, range = 24–60 months) suggested that this eventuality is not expected.
Conclusion
Nodular adrenal hyperplasia is a rare disease, which presents with the typical clinical manifestations of CS. Laparoscopic bilateral subcutaneous transposition of a pedicled adrenal is an effective and safe treatment for ACTH-independent macronodular adrenal hyperplasia. After many years of clinical validation, we have not found any complications related to this procedure. Although a longer follow-up period might be needed, this procedure may still be a good choice for patients.
Footnotes
Disclosure Statement
No competing financial interests exist.