
Abstract
Abstract
Insulinoma is a functioning endocrine neoplasm appearing primarily in the tail and body of the pancreas, although it is also rarely found in the uncinate process. The sole treatment for insulinoma is surgical resection. However, for insulinoma in the uncinate process, traditional laparoscopic surgery is controversial owing to the fact that it is a complex operation and carries a high surgical risk. Herein, we report a novel approach to complete the exposure of uncinate process and tumor resections starting from the root of the mesentery.
Introduction
I
To expose the insulinoma located in the uncinate process, traditional laparoscopic surgery always follows the route of the lesser sac, which requires considerable dissection as it necessitates dissecting open the gastrocolic ligament and mesentery. Herein, we report a new laparoscopic approach successfully applied in a specific case of pancreatic uncinate insulinoma, wherein we followed the root of mesentery.
Case
A 75-year-old man was referred to our hospital with recurrent vertigo and loss of consciousness over a period of 40 years (about once annually), but which had exacerbated over the previous 7 months (about once per month). A diagnosis of epilepsy was suspected at the local hospital, but there was no obvious improvement with medical therapy. A brain computed tomography scan showed a small degree of encephalatrophy. When an episode occurred, we found that serum glucose fluctuated between 2.1 and 2.4 mmol/L (minimum 1.3 mmol/L) and insulin fluctuated between 7.55 and 8.52 μU/ml. The resulting insulin/glucose ratio was 0.308. The symptoms resolved after the patient consumed glucose. In addition, magnetic resonance imaging (MRI) showed a nodule 1.3 cm in diameter with a clear boundary in the pancreatic uncinate process (Fig. 1A, B). The clinical symptoms, combined with laboratory and imaging results, led to a diagnosis of insulinoma.
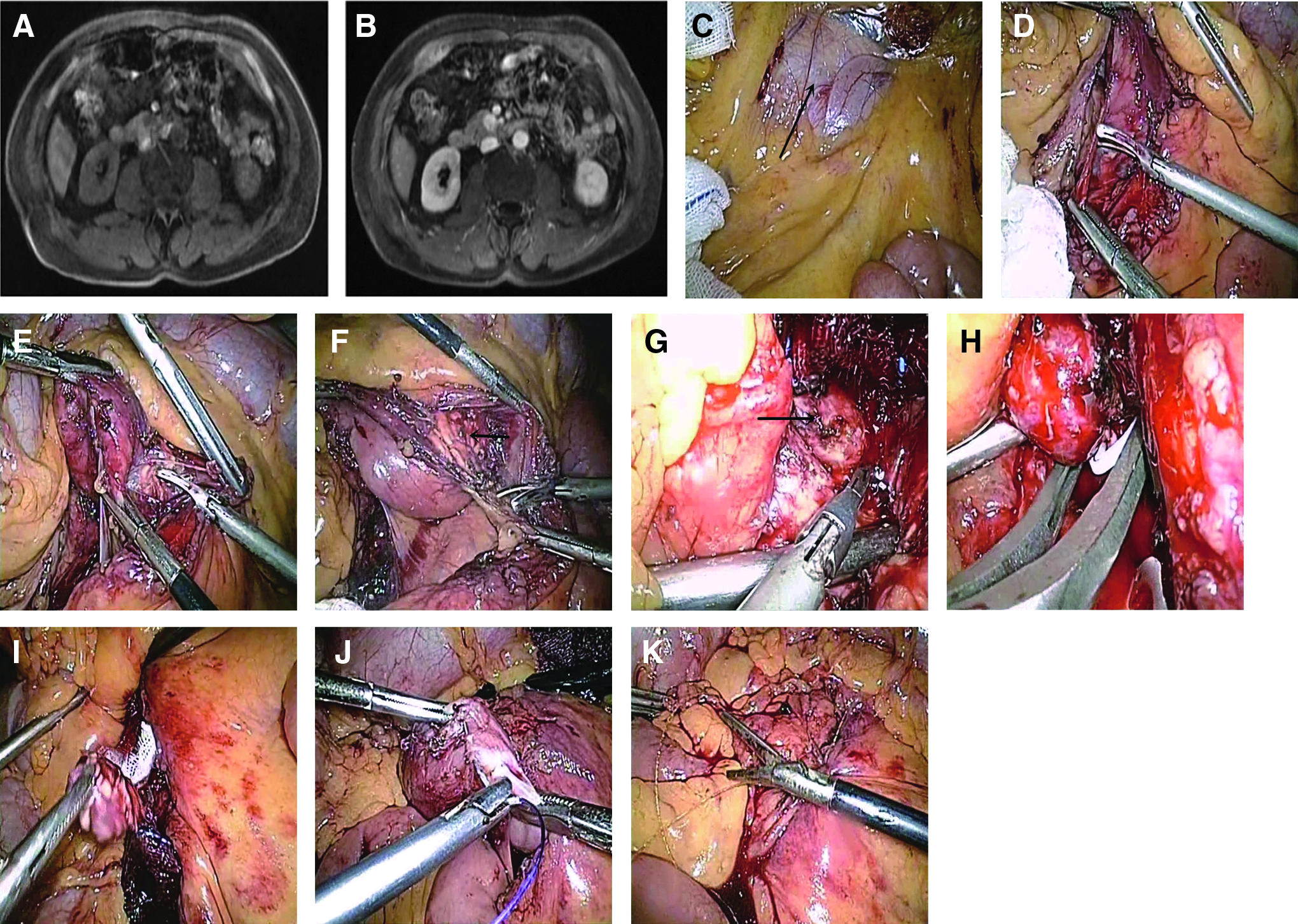
MRI revealed a tumor located inside the uncinate process and behind the superior mesenteric vessel. Using the traditional operative approach, this would have been a difficult and challenging resection and would have required a time-consuming dissection of the gastrocolic ligament and lesser sac.
However, we noted that the root of the mesentery covered the pancreatic uncinate process, and a natively avascular area was located on the right side of the root of mesentery. The descending duodenum was located posterior to this area, which suggested that we would be able to expose the tumor through this novel approach. Furthermore, we believed the advantage of this approach may be magnified using a laparoscopic technique.
Surgical Procedure
Five trocars were used for the operation: one optic, one retraction, and three working trocars. An avascular area was found on the right side of the root of mesentery after elevation of the transverse colon (Fig. 1C). The descending duodenum was immediately posterior to this area (Fig. 1D). After cutting open this area and carefully dissecting the mesentery and duodenum, the pancreatic head and uncinate process were exposed (Fig. 1E, F). A 1.3 × 1.5 cm2 tumor, part of which bulged out of the pancreas, was found at the expected site, and an enucleation procedure was applied (Fig. 1G–I). An intraoperative pathological report confirmed the diagnosis of insulinoma. After hemostasis, the surface of the wound was sutured, followed by closure of the mesentery (Fig. 1J, K). Two drainage tubes were placed near the wound surface.
The operative time was 210 minutes and blood loss was about 200 mL. Blood glucose was 2.6, 3.5, 4.1, 4.4, 4.7, 4.3, and 5.8 mmol/L at 0, 15, 30, 45, 60, 90, and 120 minutes, respectively, after resection. A grade A pancreatic fistula was found after surgery. The concentration of amylase in the drainage fluid was 154 U/L, and no special measures were taken, except observation and reexamination of amylase in the drainage fluid.
The patient recovered well and was discharged from the hospital with the drainage tubes intact 11 days after the surgery. At 23 days postsurgery, serum glucose was 5.7 mmol/L 23 days, and the concentration of amylase was 177 U/L. The drainage tubes were removed because of no drainage fluid for 3 days.
The pathology report confirmed a diagnosis of insulinoma (G2) with a 1.7 × 1.4 cm2 section area. The histopathologic examination indicated positive expression of insulin, Synaptophysin (Syn), ChromograninA (CgA), and Progesterone Receptor and negative expression of CD10 and β-catenin; the positive rate of Ki67 was 3%.
Discussion
Insulinoma is the most common functioning endocrine neoplasm of the pancreas, and surgical resection is the only effective treatment. Usually, the choice of surgery is made based on tumor size and position. 8 Most surgeons believe that laparoscopic surgery is feasible for tumors located at the body and tail of the pancreas. However, for tumors located at the head of the pancreas or close to the main pancreatic duct and portal vein, laparoscopic surgery is still controversial because of the operative difficulty and higher rate of complication. 9 Accordingly, there are few reports concerning laparoscopic resection for tumors in the uncinate process.10,11
Traditional surgery for tumors located in the uncinate process has always followed the route of the lesser sac.12,13 As an open procedure, it can be inconvenient for tumor dissection, especially for those located behind the root of the superior mesenteric vessel. By contrast, a laparoscopic technique is more convenient for maneuvers in this location. However, to expose the pancreatic head and uncinate process, the gastrocolic ligament and mesentery must be dissected, which requires considerable time. In addition, the angle of the maneuver must be designed meticulously to ensure safety of the main pancreatic duct and superior mesenteric vessel. Consequently, laparoscopic surgery for tumors in the uncinate process of the pancreas is a challenging process. 14
Alternatively, our new approach started at the root of the mesentery. Opening of the avascular area (Fig. 2) exposed the uncinate process with considerably less dissection. Compared with the duration of the traditional approach, the duration of the entire process is shorter, especially the time required for dissection of the uncinate process. In addition, this preserves the integrity of the lesser sac, which can increase the efficiency of drainage. Meanwhile, the safety of dissection can be ensured owing to the better angle of maneuver and observation.
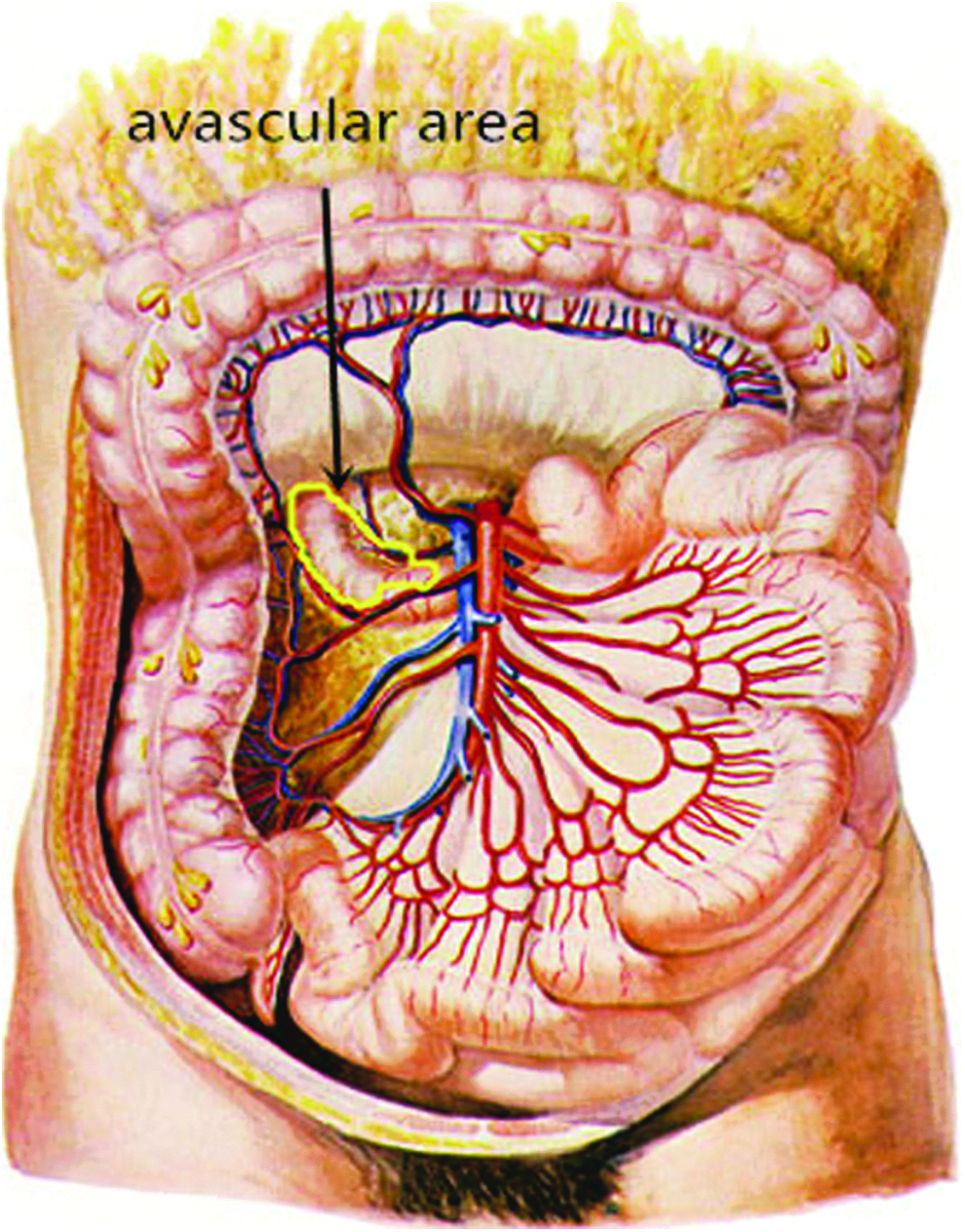
The “avascular area” (the area marked by yellow lines).
In summary, compared with traditional laparoscopic surgery for tumors in the uncinate process, this new surgical approach is safe and effective with less operative time and a lower rate of complications. Above all, less dissection, especially preservation of the lesser sac, leads to sufficient drainage and faster recovery. The success rate of the operation can likely be improved by using preoperative imaging and repeatedly checking the laparoscopic ultrasonography during the operation.15–17
Footnotes
Disclosure Statement
No competing financial interests exist.